
44yoF with a PMHxf DVT/PE (on warfarin), asthma, GERD, anxiety/depression, MEN type 1 with neuroendocrine tumors involving duodenum, stomach, and pancreas, pituitary adenoma, primary hyperparathyroidism s/p parathyroidectomy and two later resections of auto-transplanted tissue in the left arm, Whipple 5 years ago for multi-centric gastrinomas,
Patient presenting with intermittent chest pain starting day prior to admission. Characteristics of her chest pain have varied. Initially her pain was pleuritic and occurred while inhaling deeply to use her inhaler. Earlier today, she experienced chest heaviness/tightness and now, she reports her chest feels aching and sore. No recurrence of her symptoms since admission.
She arrived in the ED tachycardic to the low 100s with otherwise stable vital signs, afebrile. Initial troponin just above assay at 0.013. Subsequent troponin downtrended to normal. Lipase normal. ECG nonischemic. CTPA negative for PE; however, has findings suggestive of anomalous aortic origin of the right coronary artery. Cardiology consulted. Patient had TTE that was unremarkable. She had coronary CTA with results pending on discharge. Per cardiology, does appear to have anomalous origin of the right coronary artery from left coronary cusp and takes an interarterial course. Patient will require follow-up with congential heart disease specialist to decide if surgery needed. They did not think this was the cause of her chest pain.
TTE
Interpretation Summary
There is normal left ventricular wall thickness.
Proximal septal thickening (septal knuckle) is present.
Left ventricular systolic function is normal.
Estimated LVEF is 60%
No regional wall motion abnormalities noted.
Normal LV diastolic function.
Normal RV size and function.
The inferior vena cava is < 2.1 cm and exhibits normal respiratory variabilityconsistent with a right atrial pressure of ~ 3 mm Hg.
There is no pericardial effusion.
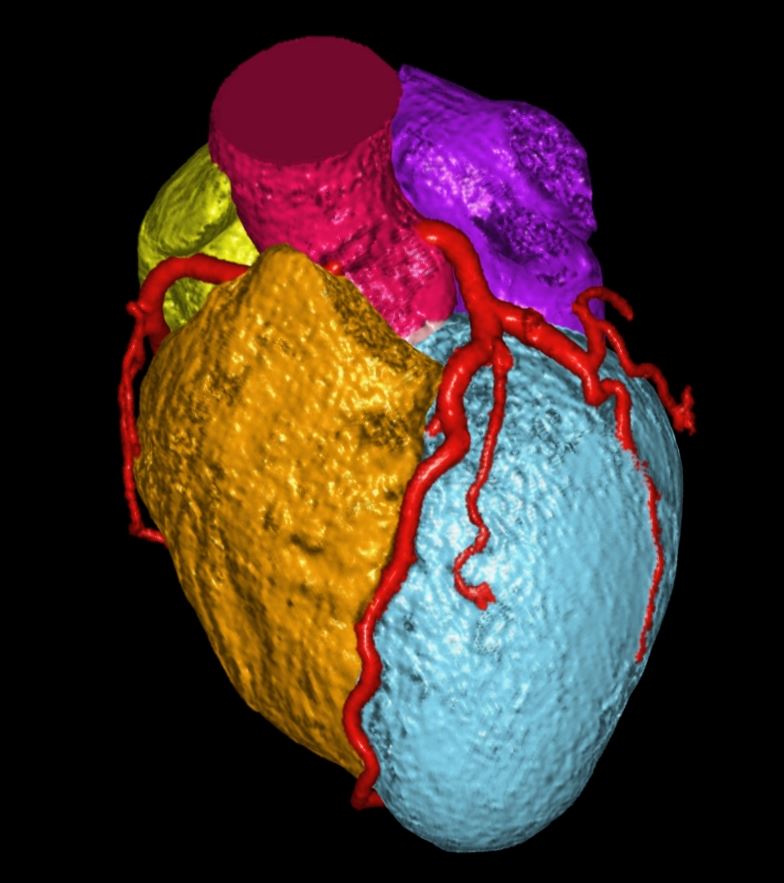
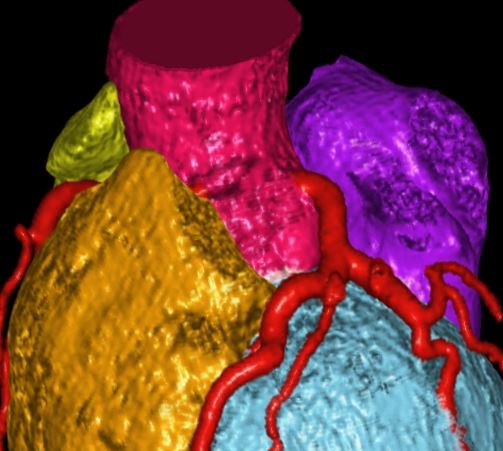
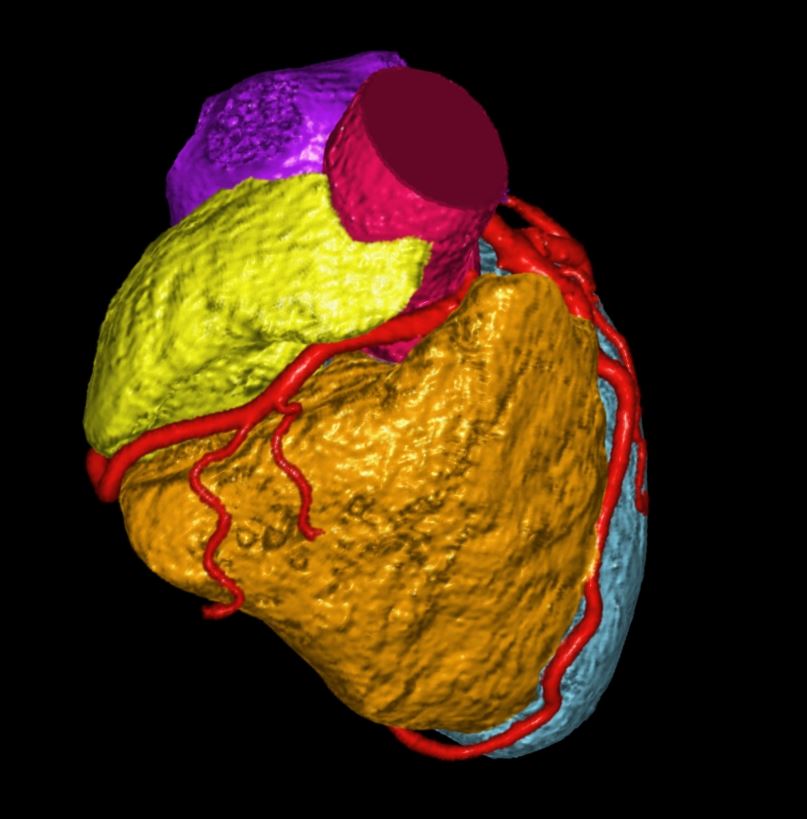
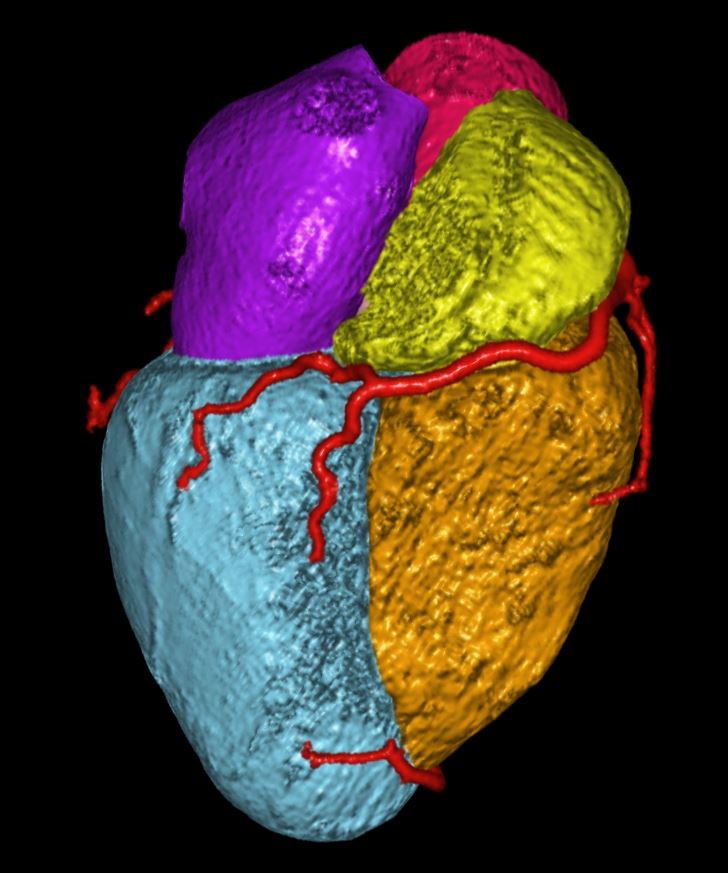
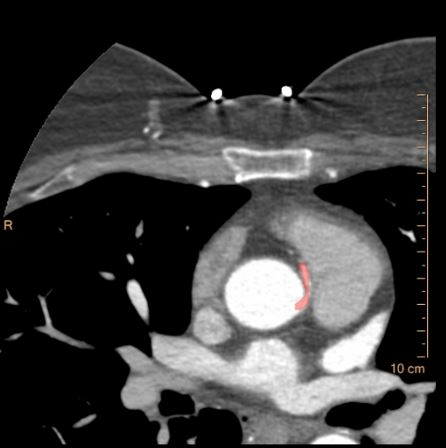
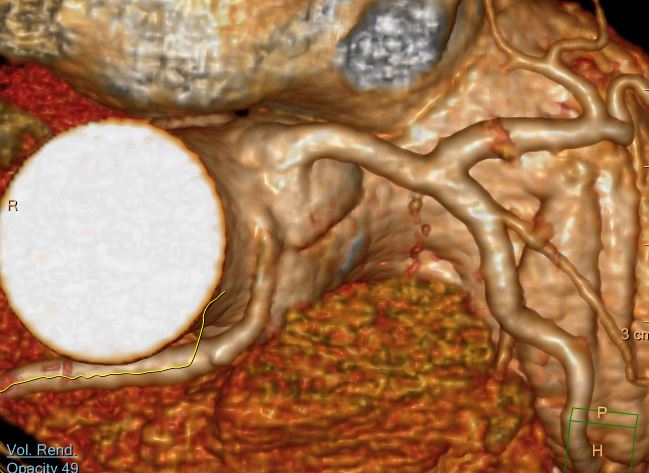
Coronary CTA
HX chest pain, anginal equivalent, with negative CTPA, which time an anomalous origin of the right coronary artery from the left coronary cusp was questioned
CT of the coronary arteries reveals following.
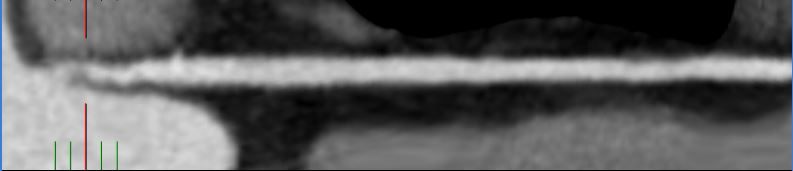
1. Anomalous origin of the RCA off the left sinus of Valsalva with
interarterial course. There is severe narrowing of the RCA origin with a slit-like orifice, with suggestion that it traverses the wall of the aorta and is near its origin. Its course reveals a relatively acute angle at its origin
2. No significant coronary artery plaque or stenosis.
3. Agatston Calcium Score = 0.
Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net

Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net

Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net