
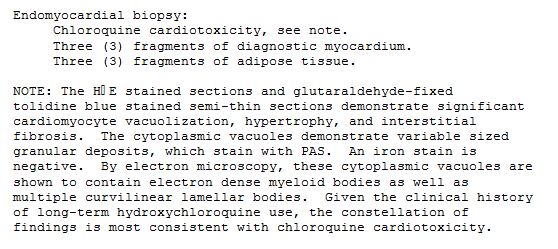
65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s

65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s Xray shows non erosive arthropathy with ulnar deviation of 2nd through 5th MCP joints
Ashley Davidoff MD
See TCV Jaccoud’s Arthropathy
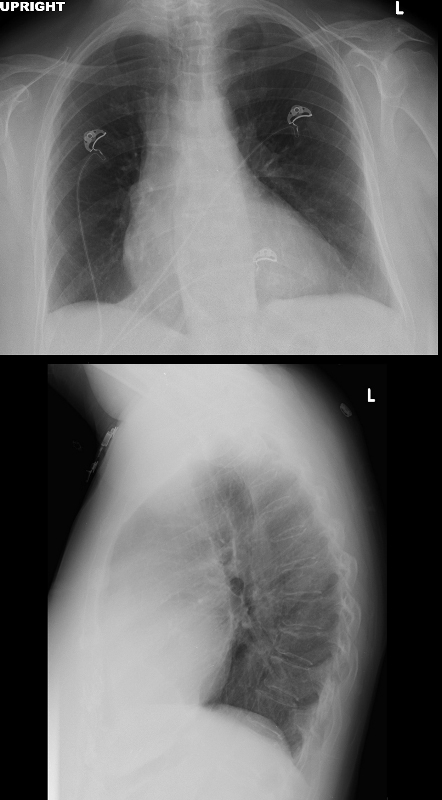
Chest Xray of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. At surgery there were adhesions and the surgeon was unable to identify the coronaries as a result of the fibrosis. She was closed without surgery. She subsequently had a diagnostic MRI and endomyocardial biopsy which showed chloroquine related cardiomyopathy
Ashley Davidoff MD

Chest X-ray of a 65-year-old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. CXR on the frontal view shows a CT ratio that is probably normal, equivocal carinal angle and no evidence of CHF. Lateral exam suggests RVE with RV : sternal ration being >30% and LV: diaphragm ratio being >33%
Ashley Davidoff MD
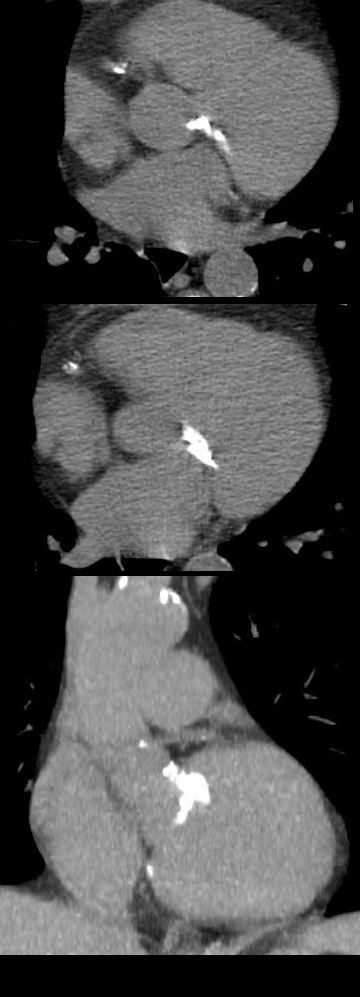
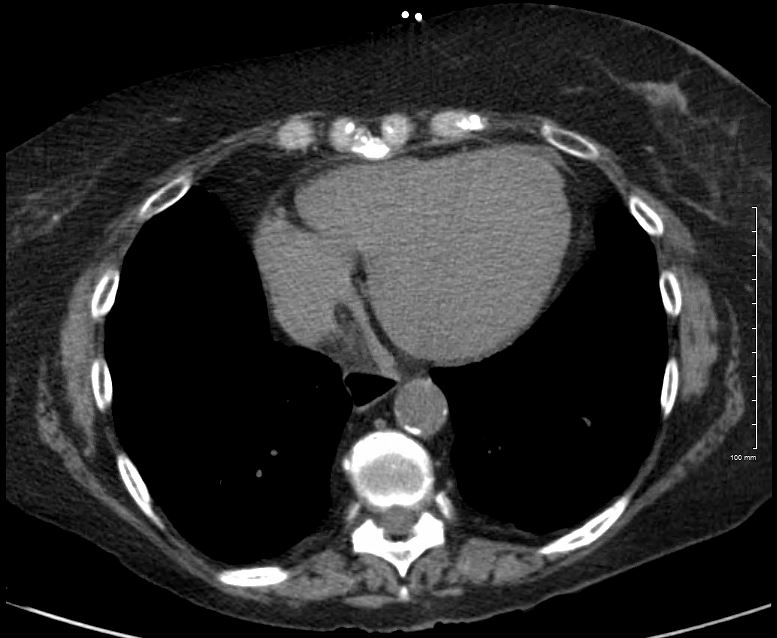
CT scan of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. At surgery there were adhesions and the surgeon was unable to identify the coronaries as a result of the fibrosis. She was closed without surgery. She subsequently had a diagnostic MRI and endomyocardial biopsy which showed chloroquine related cardiomyopathy
Ashley Davidoff MD

CT scan of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. At surgery there were adhesions and the surgeon was unable to identify the coronaries as a result of the fibrosis. She was closed without surgery. She subsequently had a diagnostic MRI and endomyocardial biopsy which showed chloroquine related cardiomyopathy
Ashley Davidoff MD
CT scan of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. At surgery there were adhesions and the surgeon was unable to identify the coronaries as a result of the fibrosis. She was closed without surgery. She subsequently had a diagnostic MRI and endomyocardial biopsy which showed chloroquine related cardiomyopathy
Ashley Davidoff MD
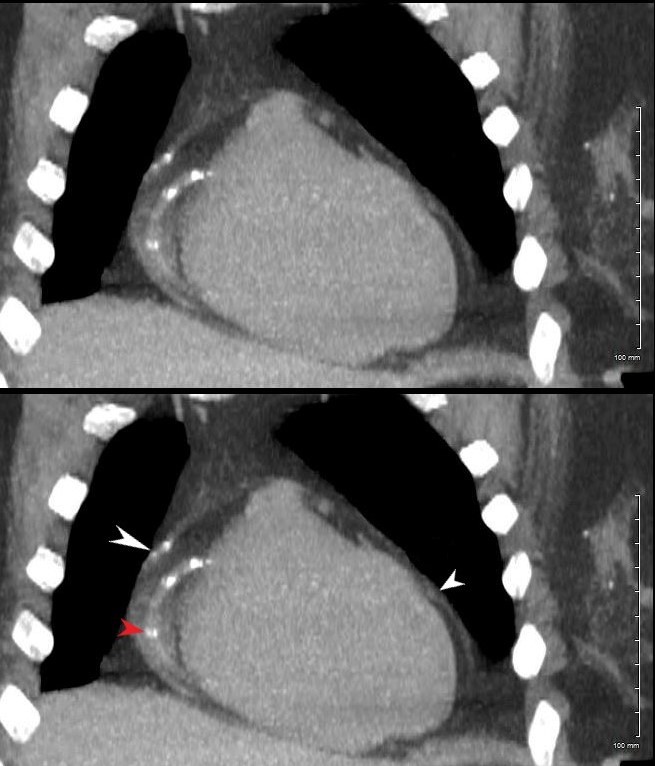
? Signs of Constriction
Size of the Right Atrium

The axial image through the region of the AV valves shows normal sized atria. Constriction would be unlikely in the face of a normal sized right atrium. Note the flattened surface of the right atrium
Ashley Davidoff MD
Size of the Coronary Sinus
The axial image through the region of the normal sized coronary sinus. Constriction would be unlikely in the face of a normal sized coronary sinus. Note the flattened surface of the right atrium.
Ashley Davidoff MD
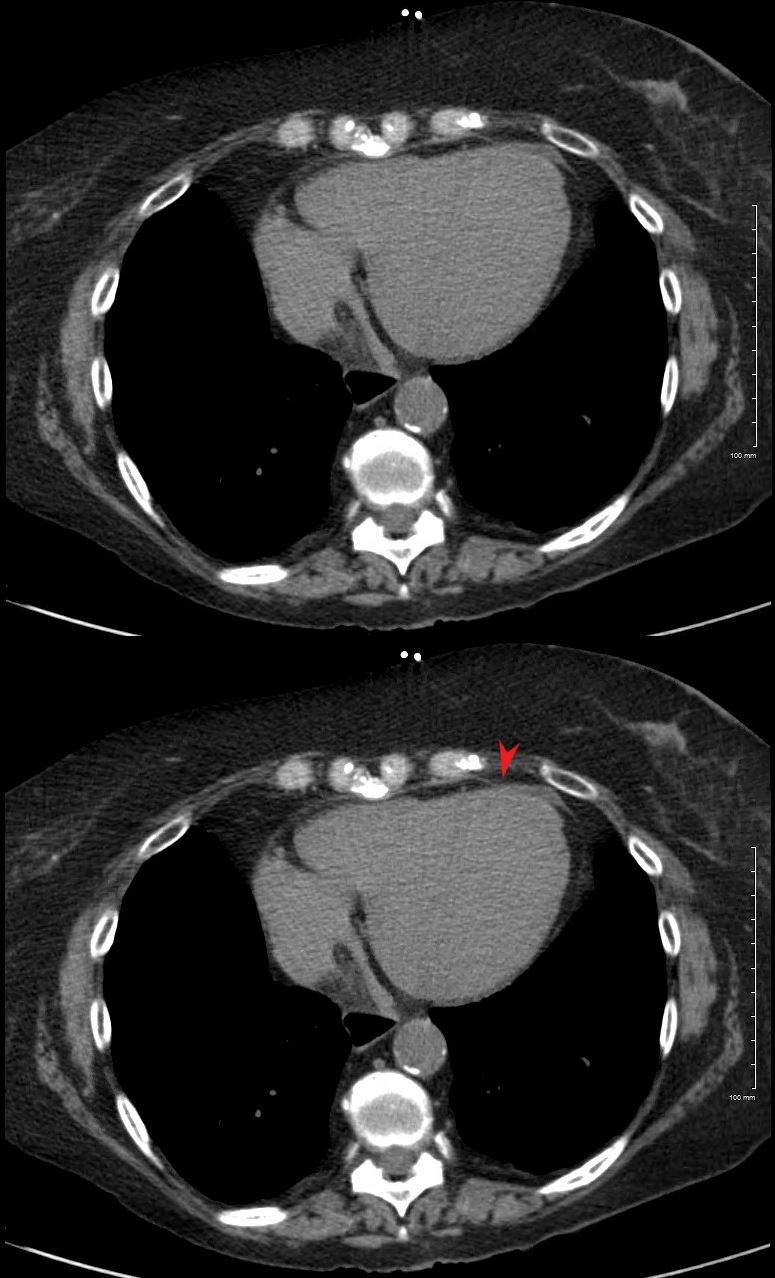
? Size of the Azygos Vein and IVC

The axial image is through the region of the normal azygos vein (above) and the normal sized IVC (below). Constrictive pericarditis would be unlikely in the face of a normal sized azygos vein and IVC.
Ashley DAvidoff MD
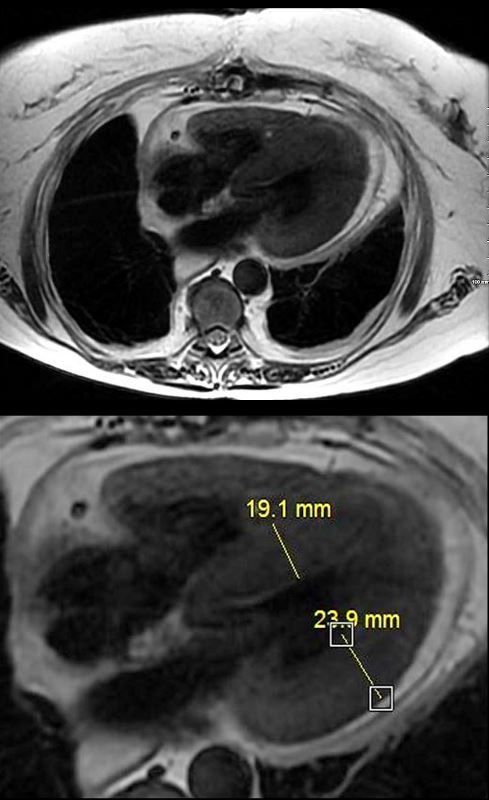
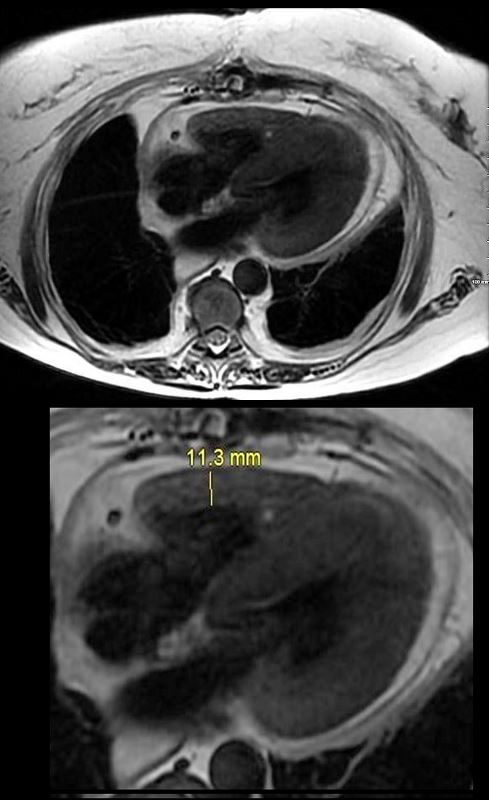
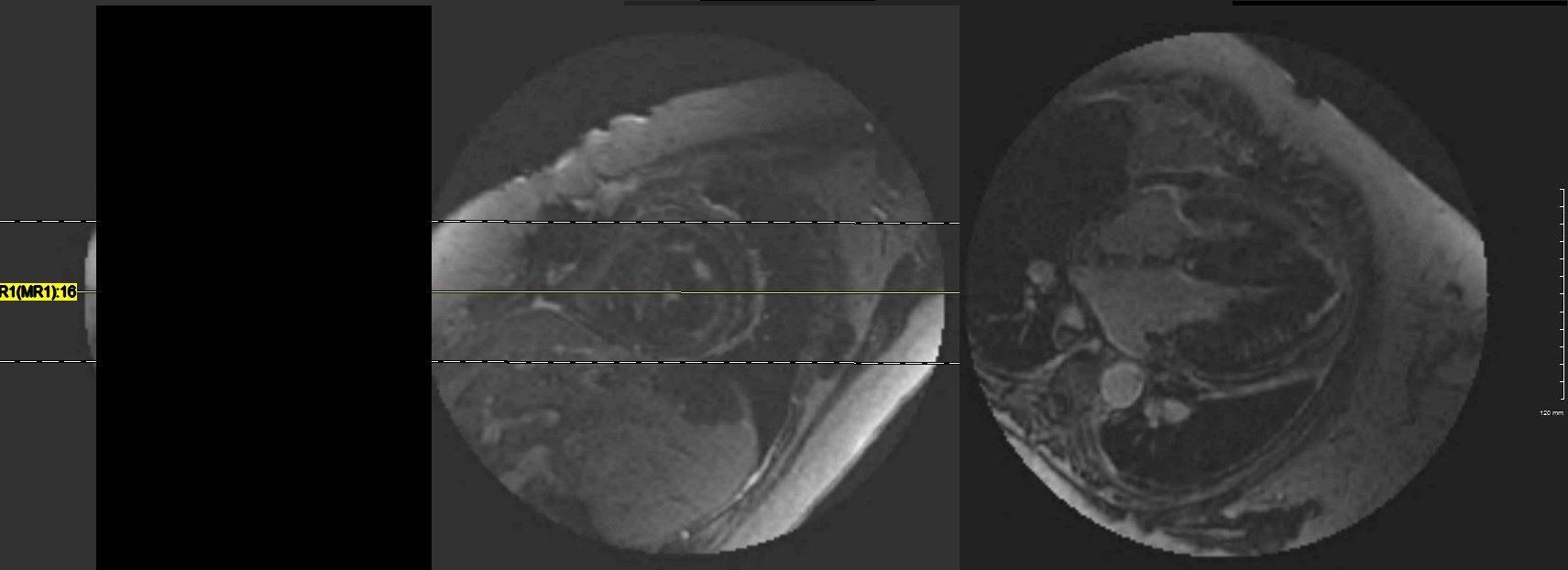
MRI with 4 chamber view from “black blood” T2 weighted imaging of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. At surgery there were adhesions and the surgeon was unable to identify the coronaries as a result of the fibrosis. She was closed without surgery. She subsequently had a diagnostic MRI and endomyocardial biopsy which showed chloroquine related cardiomyopathy
Ashley Davidoff MD
Ashley Davidoff MD

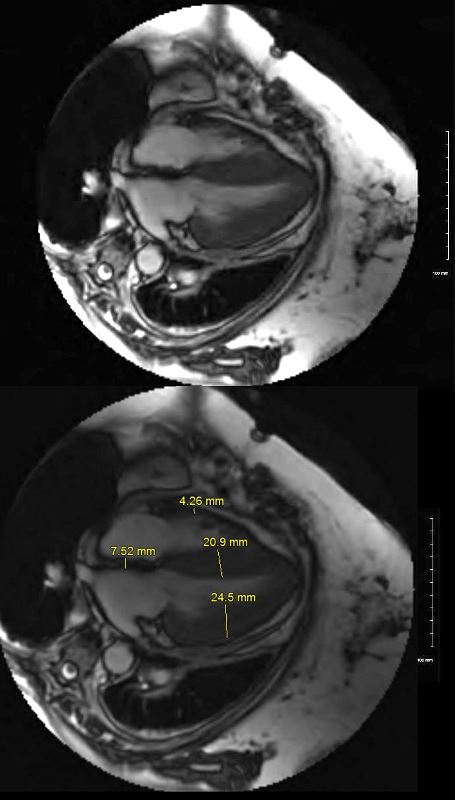
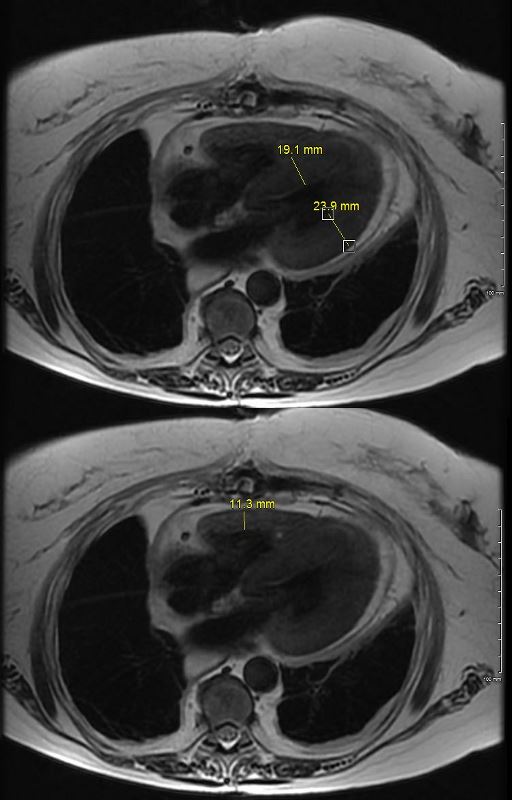
MRI with 2 chamber view in diastole of a 65 year old female with longstanding history of SLE, Lupus Sjogren’s and Raynaud’s presented with 2 weeks of dyspnea and elevated troponins suggestive of a STEMI. Cardiac cath showed 2 vessel disease and she was referred for CABG. At surgery there were adhesions and the surgeon was unable to identify the coronaries as a result of the fibrosis. She was closed without surgery. She subsequently had a diagnostic MRI and endomyocardial biopsy which showed chloroquine related hypertrophic cardiomyopathy

Short axis during first pass while still in RV (above) and then delayed post gadolinium shows diffuse mid myocardial circumferential LGE enhancement consistent with an infiltrative cardiomyopathy
Ashley Davidoff MD

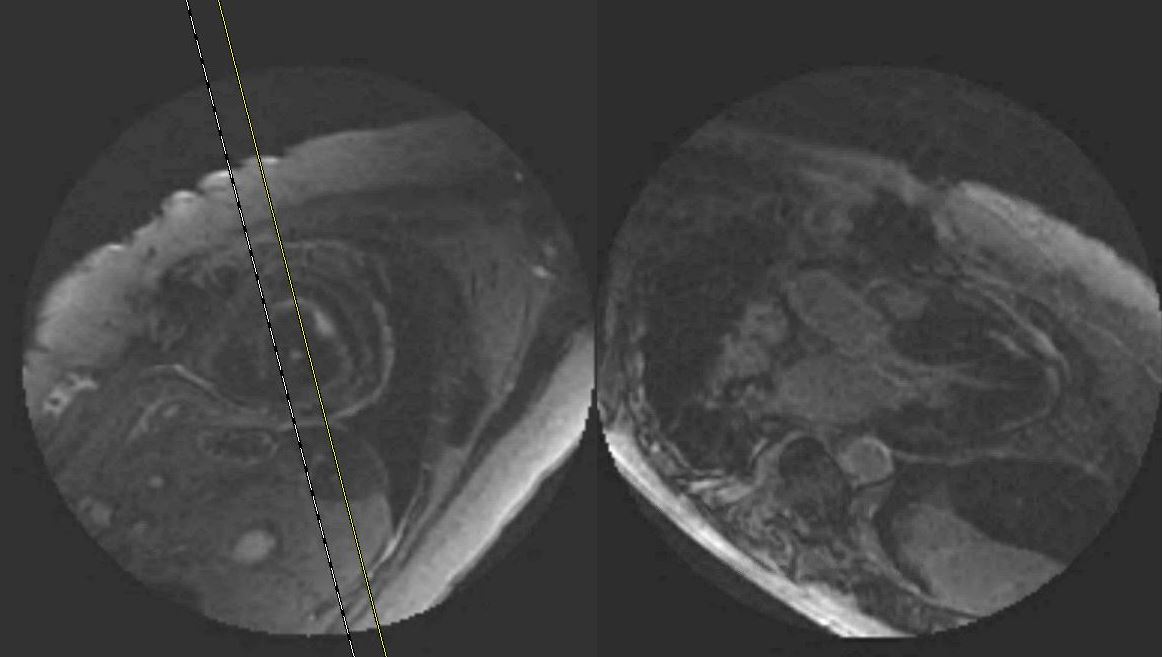
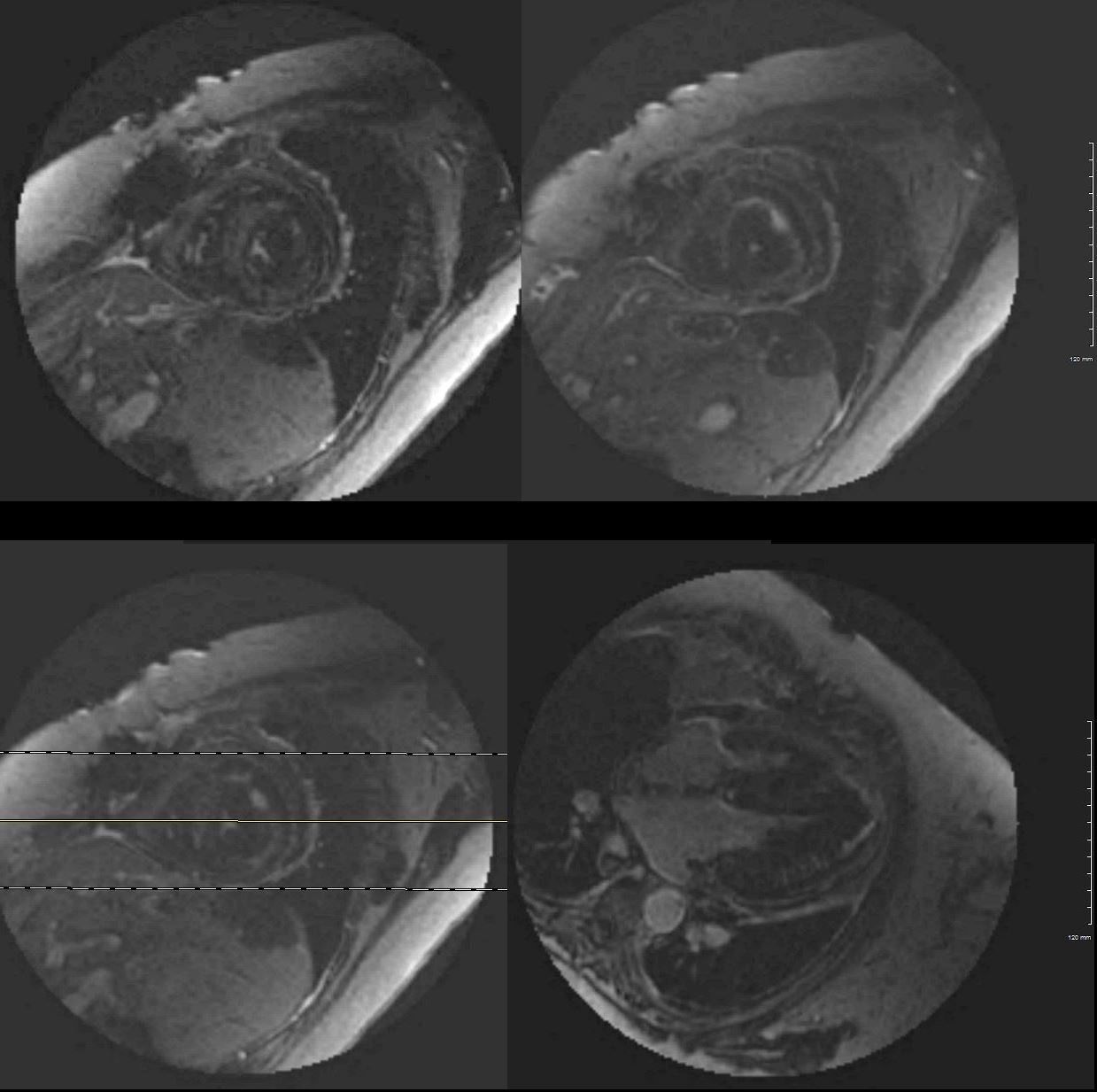
A series of three inversion times , 150, 200 and 250 msec reveals an inability to null the myocardium indicating a diffuse infiltrative process
Ashley Davidoff MD
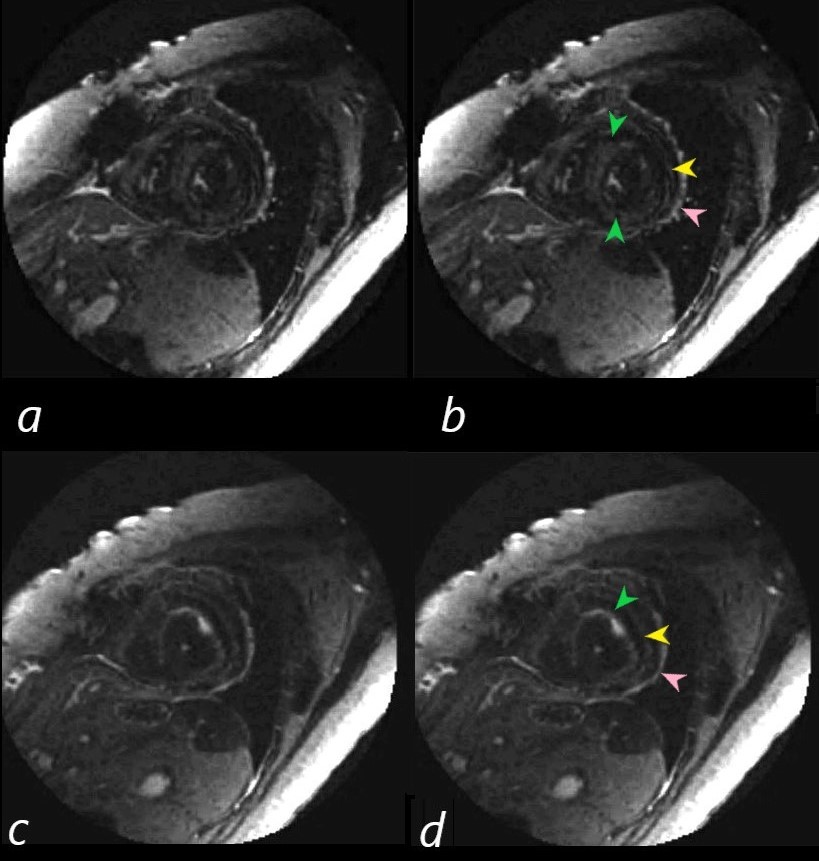
Short axis images on the delayed post Gad images show 3 rings of LGE. Image b (correlate with image a) is through the body of the LV and shows mid myocardial LGE seen as an almost complete ring of diffuse accumulation (green arrowheads), a thin ring of more peripheral mid myocardial LGE (yellow arrowhead) together with probable pericardial LGE (yellow arrow head)
In image d (correlate with image c) near the apex of the heart, there are 2 distinct rings of a linear morphology in the mid myocardium. The inner ring (green arrowhead) has some focal nodularity and an outer mid myocardial ring (yellow arrowhead) . Subepicardial or pericardial enhancement is suggested as well (pink arrowhead).
Ashley Davidoff MD
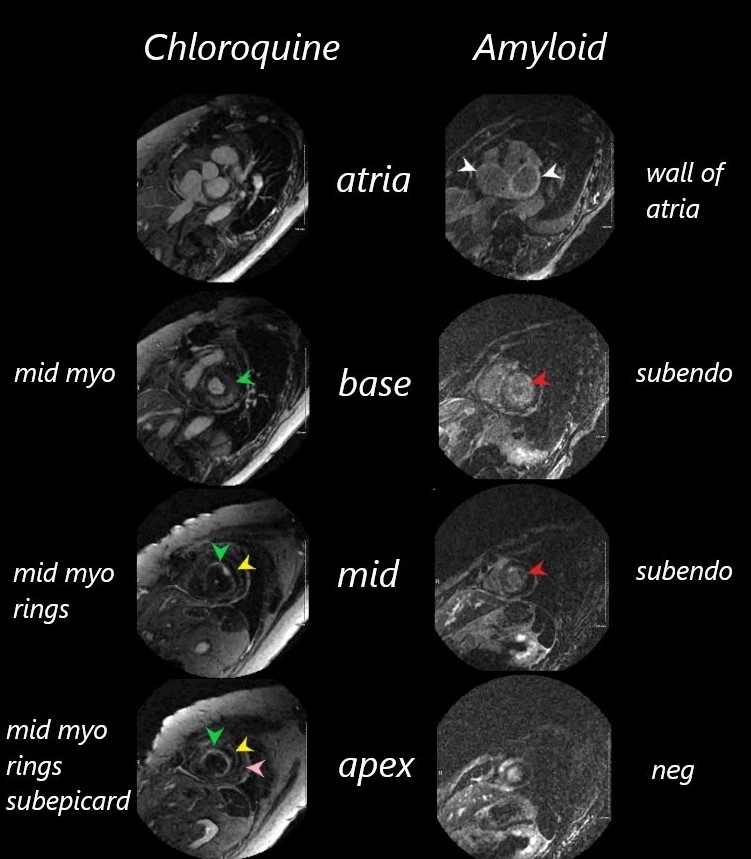
It was difficult to null the myocardium on both these patients.
The images are organized from the atria (top images through the bases, bodies and apices (lowest images) of the left ventricles.
The chloroquine cardiomyopathy shows no LGE of the atria, but progressive linear cicumferential mid- ventricular LGE through to the apex
The amyloid cardiomyopathy hase LGE in both atrial walls, circumferential LGE through the base and body o the LV but sparing of the apex.
Ashley Davidoff MD
ammyloid case 131429
Links and References
Joyce, E et al Hydroxychloroquine cardiotoxicity presenting as a rapidly evolving biventricular cardiomyopathy: key diagnostic features and literature review Eur Heart J Acute Cardiovasc Care. 2013 Mar; 2(1): 77–83.
Yogasundaram H etal Chloroquine‐induced cardiomyopathy: a reversible cause of heart failure ESC Heart Fail v.5(3); 2018 Jun
References and Links
- TCV