
Angina
The Common Vein Copyright 2008
Dima Quraini MD
Ashley Davidoff MD
Definition
Angina is a symptom characterized by chest pressure or discomfort caused by myocardial ischemia. The pain is usually precipitated by exercise or emotional stress, and lasts between 30 seconds and 20-30 minutes. The classic presentation of myocardial ischemia was first described by Dr William Heberden in a lecture before the Royal College of Physicians in 1768. He claimed that “the seat of it, and sense of strangling and anxiety, with which it is attended, may make it not improperly be called angina pectoris”.
The onset is acute, and intensifies within minutes, and is characterized by adjectives such as tightness, pressure, or heaviness, most commonly in the retrosternal region but it may involve the precordium. It is aggravated by continued exercise, and is characteristically relieved when the physical or emotional stress is abated or following administration of nitroglycerine. The discomfort may radiate to the neck, jaw, or left arm. Associated symptoms include an impending sense of doom originally described as “angor animi” which literally means anguish of the soul. This sensation sometimes accompanies other life threatening situations when there is massive outpouring of catecholamines, such as aortic dissection and pulmonary embolism. Associated symptoms include shortness of breath, nausea and diaphoresis. It is usually although not necessarily precipitated by exercise or emotional stress. The episodes of angina recur usually with the same degree of excercise, and patients can predict their excercise tolerance. These episodes can also progress in frequency and can present while the patient is at rest, but do not usually wake the patuient from sleep.
An important distinction should be made between patients presenting with a single and acute episode of chest pain versus patients who chronically develop chest pain on exertion. The latter is termed stable angina and can be managed medically unless the patient is symptomatic despite optimal medical therapy.
Unstable angina on the other hand that is not responding to usual measures and is recurring at rest infers an unstable pattern of angina and is termed unstable angina. This entity is part of the acute coronary syndrome.
The diagnosis if angina is suggested by the history since it has unique and characteristic profile, but the diagnostic algorithm includes stress testing and sometimes angiography. Esophageal spasm can present with similar features of angina, and sometimes even responds to nitroglycerine, but it is not usually precipitated by excercise, nor relieved by rest.
Acute Myocardial Infarction
(b) Sudden Severe Pain Pressure Discomfort
c) Unrelieved by TNG and Rest
71197c08c.800 substernal chest pain burning esophagus heart cardiac esophagitis reflux retrosternal chest pain radiating to neck and left arm unrelieved by rest and sublingual nitroglycerine myocardial infarction time hours CTscan 3D Davidof art Courtesy Ashley Davidofff MD
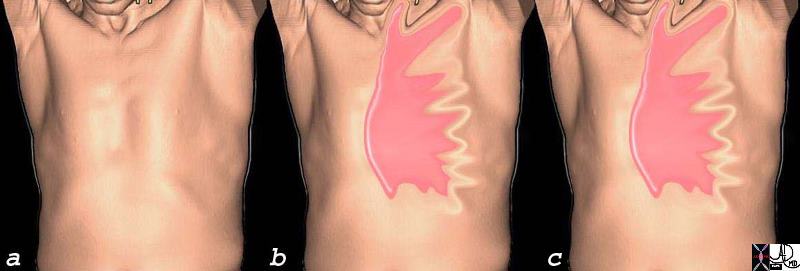
Stable Angina – Predictable Patterns a) No pain – exercise b) Pain Pressure Typical Distribution c) Relieved by Rest, TNG |
| Angina is characteristically a dull pressure like pain, that is precipitated by stress usually after a predictable distance of a walk or run for example. In a, the patient has no discomfort, develops pain after a fixed distance, and then stops. The pain is relieved
71197c07c substernal chest pain burning esophagus heart cardiac esophagitis reflux substernal chest pain radiating to neck and left arm relieved by rest and sublingual nitroglycerine angina CTscan 3D Courtesy Ashley Davidofff MD |
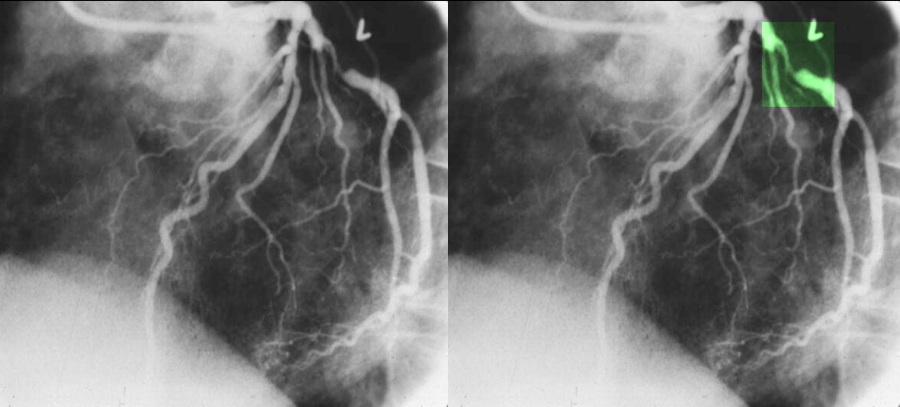
>70% Stenosis of the Left Circumflex Coronary Artery
|
| The coronary angiogram in the LAO projection shows a severe proximal stenosis (>70%) of the circumflex with some post stenotic dilatation. The second image has a green overlay indicating the region of disease with the post stenotic dilatation.
Courtesy Ashley Davidoff MD. 07023c |
Treatment is directed to preventing further progression of the disease with dietary control, weight loss, lipid management, and behavioral modification, while the finding of structural disease may require angioplasty stenting or coronary artery
bypass.
Diagnosis
Plain chest radiograph
A plain chest radiograph is usually the first imaging modality used to evaluate chest pain in the emergency department. It is an inexpensive test that may yield important information on thoracic structures such as the lung, heart and the great vessels. It is highly sensitive to non-cardiac pathologies that are in the differential diagnosis of chest pain such as pneumonia and pneumothorax. Although one cannot diagnose an acute coronary syndrome from a chest radiograph, many indirect findings such as changes in cardiac silhouette, pulmonary edema, calcification of the myocardium or coronary arteries may suggest underlying coronary artery disease.
Treadmill exercise electrocardiography (ECG)
A treadmill exercise ECG test is both safe and useful in patients thought to be at low to intermediate risk of having an acute coronary syndrome and who have a normal baseline 12 lead ECG. It is inexpensive, widely available and provides both diagnostic and prognostic information. Since prevalence of coronary artery disease in the selected population of patients is expected to be low, a negative treadmill exercise ECG has a high negative predictive value. A negative treadmill exercise ECG performed within 48 hours of presentation is associated with a 2 % cardiac event rate at 6 months, whereas that percentage rises to 15% in patients found to have a positive or equivocal treadmill exercise ECG.
Resting myocardial perfusion imaging (MPI) and transthoracic echocardiography
Both observational and prospective studies conclude that a resting myocardial perfusion imaging performed in the emergency department help reduce the rate of unnecessary hospitalizations in patients presenting with chest pain. A normal resting MPI has a negative predictive value that is equal or superior to 99% whereas a normal serum troponin level drawn at the same time has a negative predictive value of 39%. However, resting MPI is mostly useful in patients with no prior history of myocardial infarction.
A transthoracic echocardiography is most helpful during a patient’s episode of chest pain as wall motion abnormalities can be visualized within seconds of coronary artery occlusion. The echocardiography may also aid in patients in whom symptoms have resolved. Actually, a wall motion abnormality visualized with or without pain is associated with poor prognosis. The transthoracic echocardiography can help identify or rule out many causes of chest pain such as aortic dissection, pericarditis along with pericardial tamponade and pulmonary embolism. In brief, it is a highly sensitive exam for multiple pathologies and therefore not very specific.
Stress echocardiography and radionuclide scans
Stress echocardiography or radionuclide scans are preferred stress imaging modalities in patients with an abnormal baseline ECG or who have an inconclusive treadmill exercise ECG. Although these imaging modalities are more expensive and less available than a treadmill exercise ECG, they have a higher sensitivity to detect coronary artery disease. Also, they provide more information on extent and possible location of disease.
CT scanning
The role of CT and its place in algorithms are still being determined. CT scan has a promising role in patients deemed to be at low risk for an acute coronary syndrome. Coronary calcium is associated with coronary artery disease with a sensitivity ranging between 88 to 100%. A coronary artery calcium score (CAC) can be determined. A low CAC score carries a high negative predictive value for future cardiac events. CTA of the vessels has a high negative predictive value, and thus can exclude significant coronary artery disease.