
74-year-old male with type 2 diabetes, CAD s/p stent 6 years prior, hypertension and hypercholesterolemia, fell at home and presents to the ER.
A CXR performed 4 years before, showed no acute cardiopulmonary disease. Healed right sided rib fractures and healed right clavicular fracture were of incidental note

A CXR performed 4 years before, shows no acute cardiopulmonary disease. Healed right sided rib fractures and healed right clavicular fracture were of incidental note
Ashley Davidoff MD
In the ER a non-displaced right hip fracture was identified and uncomplicated hemiarthroplasty was performed.
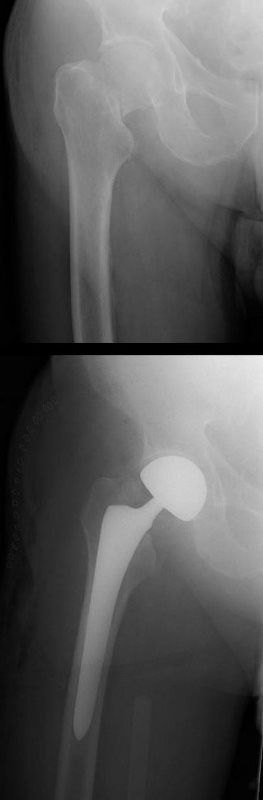
In the ER a non-displaced right hip fracture was identified and uncomplicated hemiarthroplasty was performed.
Ashley Davidoff MD
CXR at the time showed no acute disease

CXR at the time shows no acute disease
Ashley Davidoff MD
He was discharged and in the interim prior to readmission 2 weeks later his wife fell and had to be admitted to the hospital.
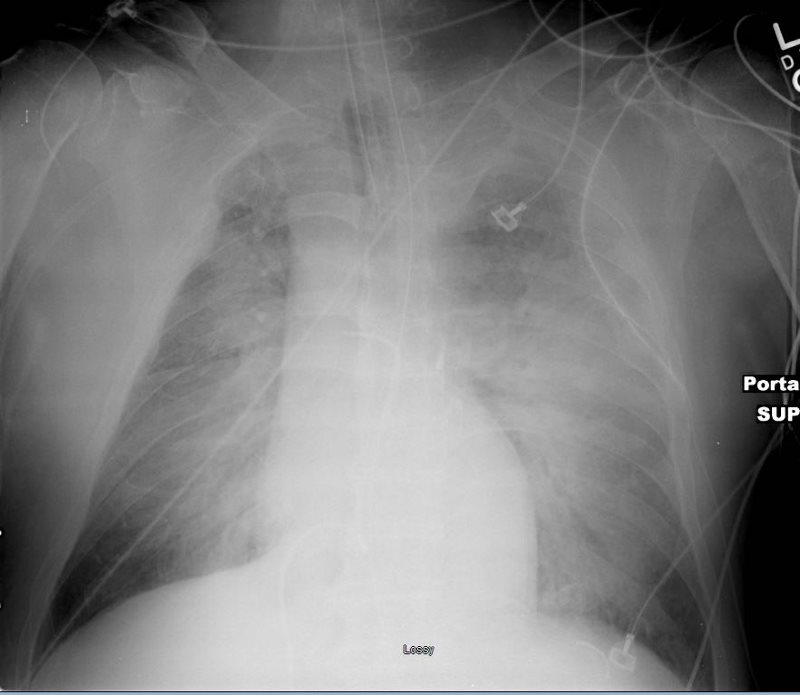
At the time of his next readmission he presented in shock. (NYHA Class IV and ASA Class 4)
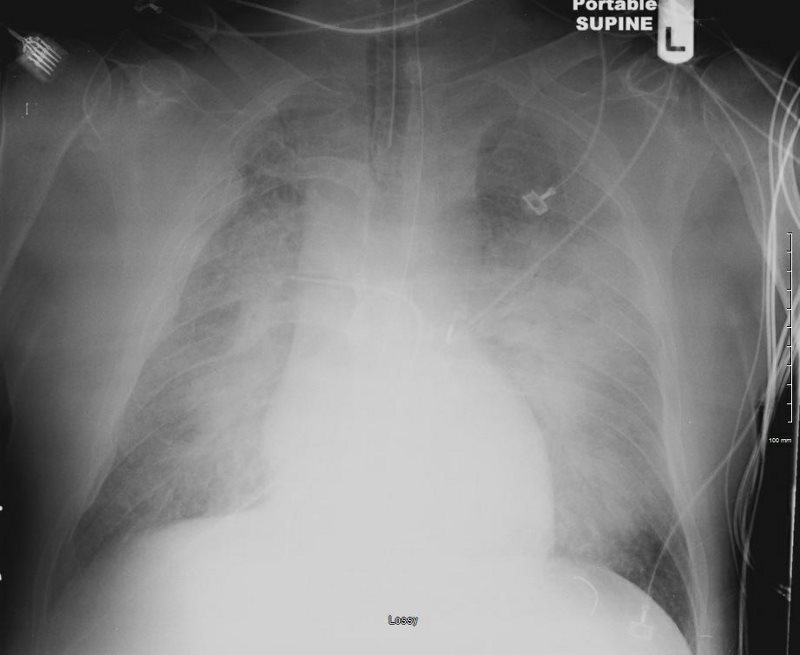
CXR showed pulmonary edema.

At the time of his next readmission he presented in shock. (NYHA Class IV and ASA Class 4)
CXR showed pulmonary edema.
EKG showed new LBB
Ashley Davidoff MD
EKG showed new LBB
Echo at the bedside in the ICU showed an ejection fraction of 15%, with global hypokinesis sparing the base of the heart. There was moderate MR, PAP 44-65mm Hg, RV was normal.
Preliminary diagnosis of an acute MI was made with acute systolic heart failure and cardiogenic shock
He was transferred to the Cath Lab
Prior to gaining access to the arterial system the patient went into PEA requiring sustained CPR requiring both epinephrine, atropine and urgent intubation
Emergent cardiac catheterization showed an LV pressure of 64/17 and wedge pressure of 41 mmHg. Temporary pacemaker was placed as well as an IABP. No significant CAD was identified.

Ashley Davidoff MD
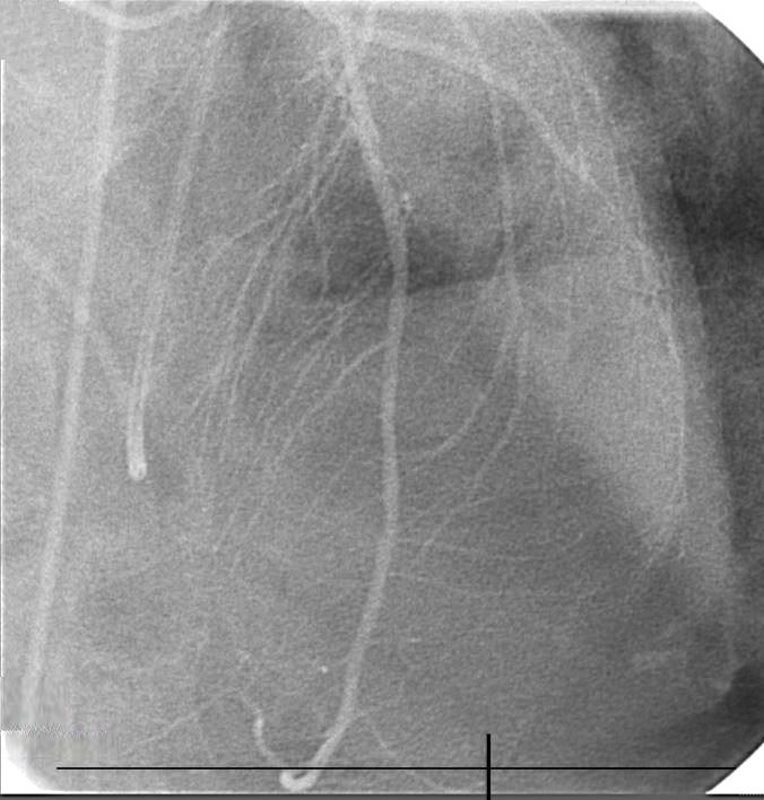
No significant CAD was identified. Ashley Davidoff MD

Ashley Davidoff MD
IABP placed

Ashley Davidoff MD
LV gram showed ballooning of the apex of the heart consistent with Takotsubo cardiomyopathy with an estimated ejection fraction of 10%

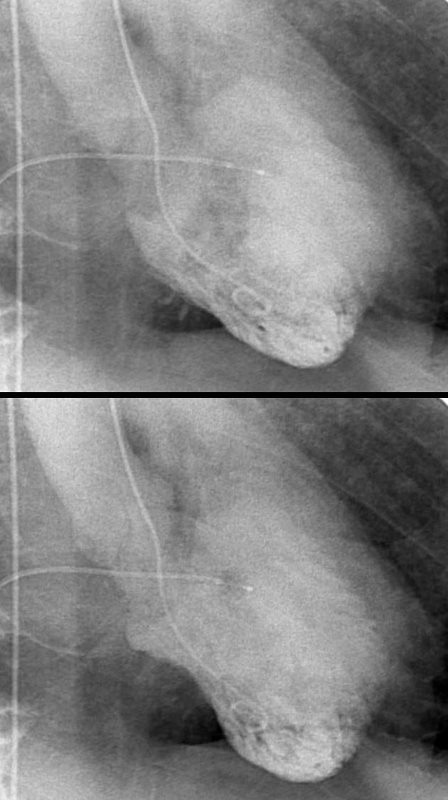
LV gram showed ballooning of the apex of the heart consistent with Takotsubo cardiomyopathy with an estimated ejection fraction of 10%
Ashley Davidoff MD
Serial CXR showed ongoing perihilar infiltrates with air bronchograms consistent with cardiogenic and alveolar edema.

TAKOTSUBO CARDIOMYOPATHY Ashley Davidoff MD
TAKOTSUBO CARDIOMYOPATHY
Ashley Davidoff MD
TAKOTSUBO CARDIOMYOPATHY
Ashley Davidoff MD
He passed away 2 days later – Broken Hearted
- Points of Interest
- Acute presentation and Death from Takotsubo
-
References and Links