
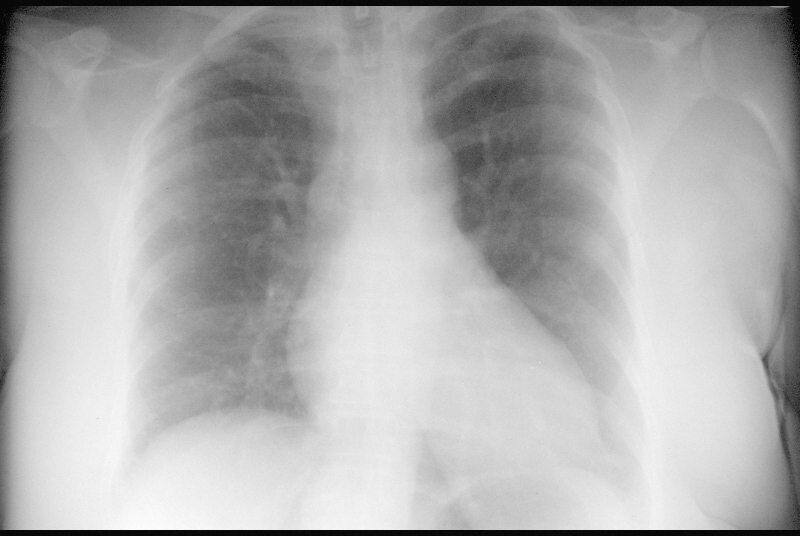
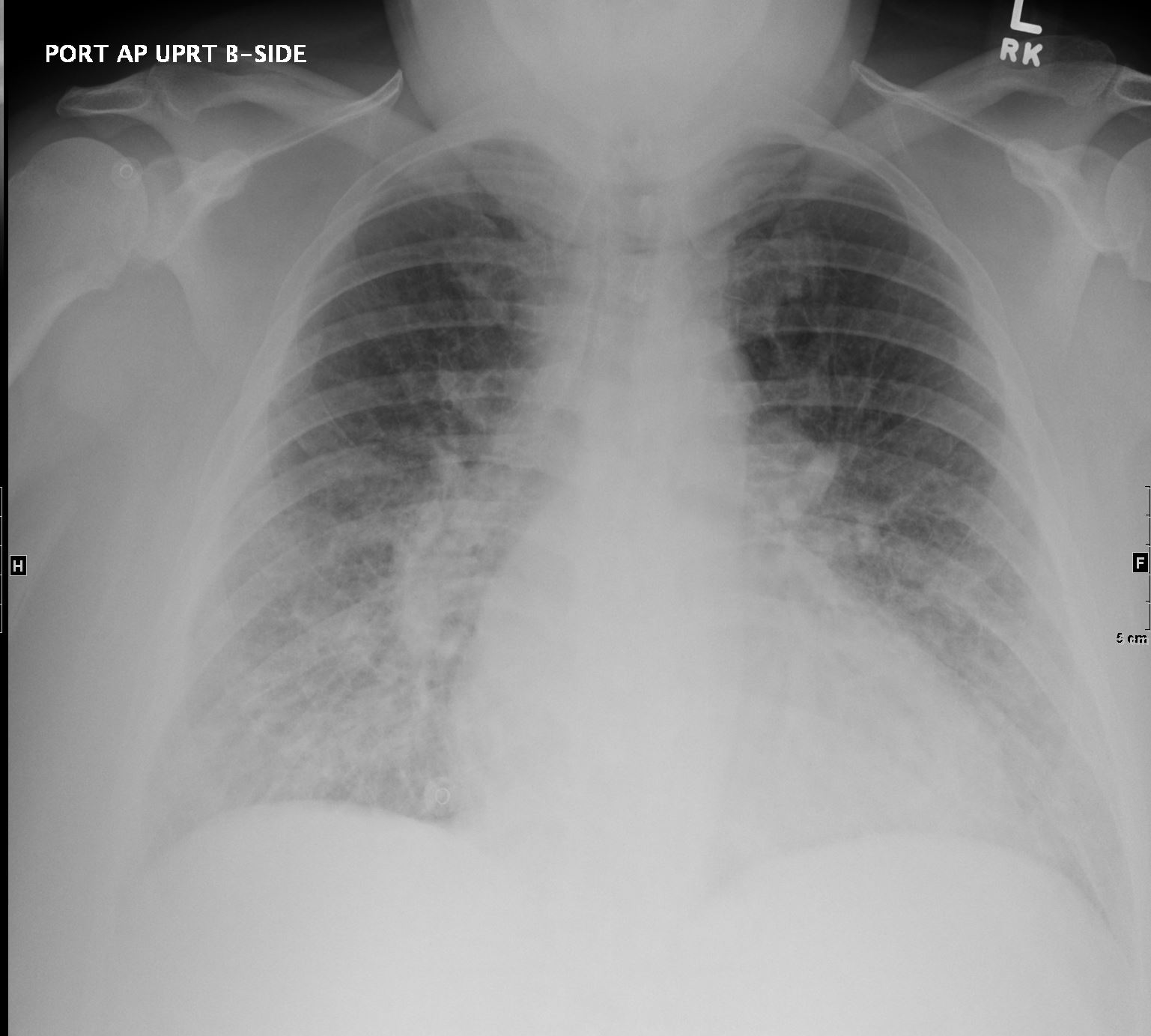
56-year-old female presents with with dyspnea. PA CXR shows possible left atrial enlargement equalization of the pulmonary vessels and suggestion of left ventricular (LV) enlargement reflecting an approximate end diastolic pressure of between 10 and 20 mmHg
indicating early mild heart failure. The azygous vein is enlarged suggesting right heart failure as well.
Ashley Davidoff TheCommonVein.net 16515
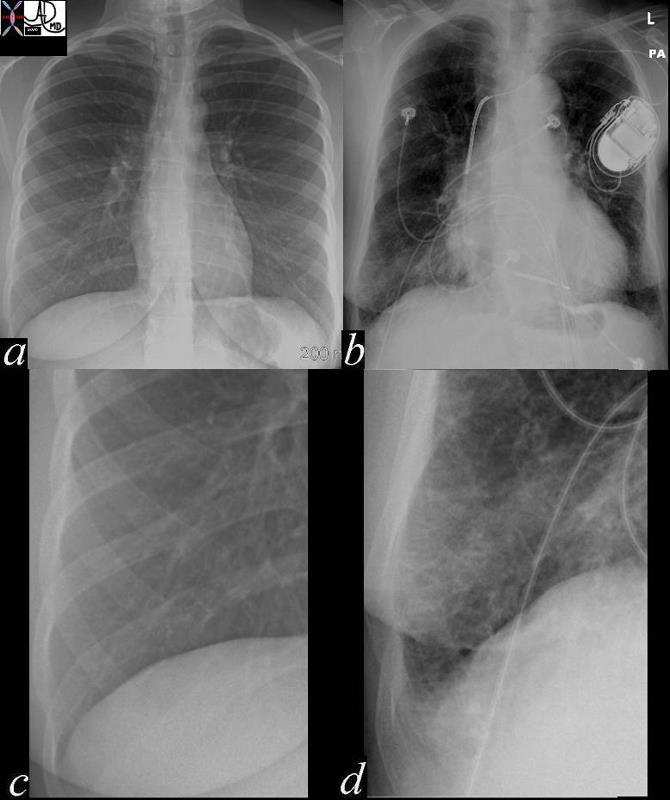
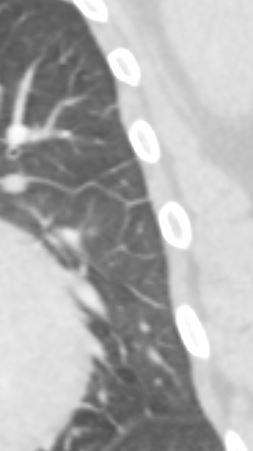
In these images. and c are normal and b and d represent thickened interlobular septa in a patient with congestive heart failure. These are the well known Kerley lines, often spoken about but rarely seen. They are identified as thin horizontal lines usually seen in the costophrenic angles, not being longer than 2 cms in length and touching the pleural surface.
42545c01.800 Ashley Davidoff MD
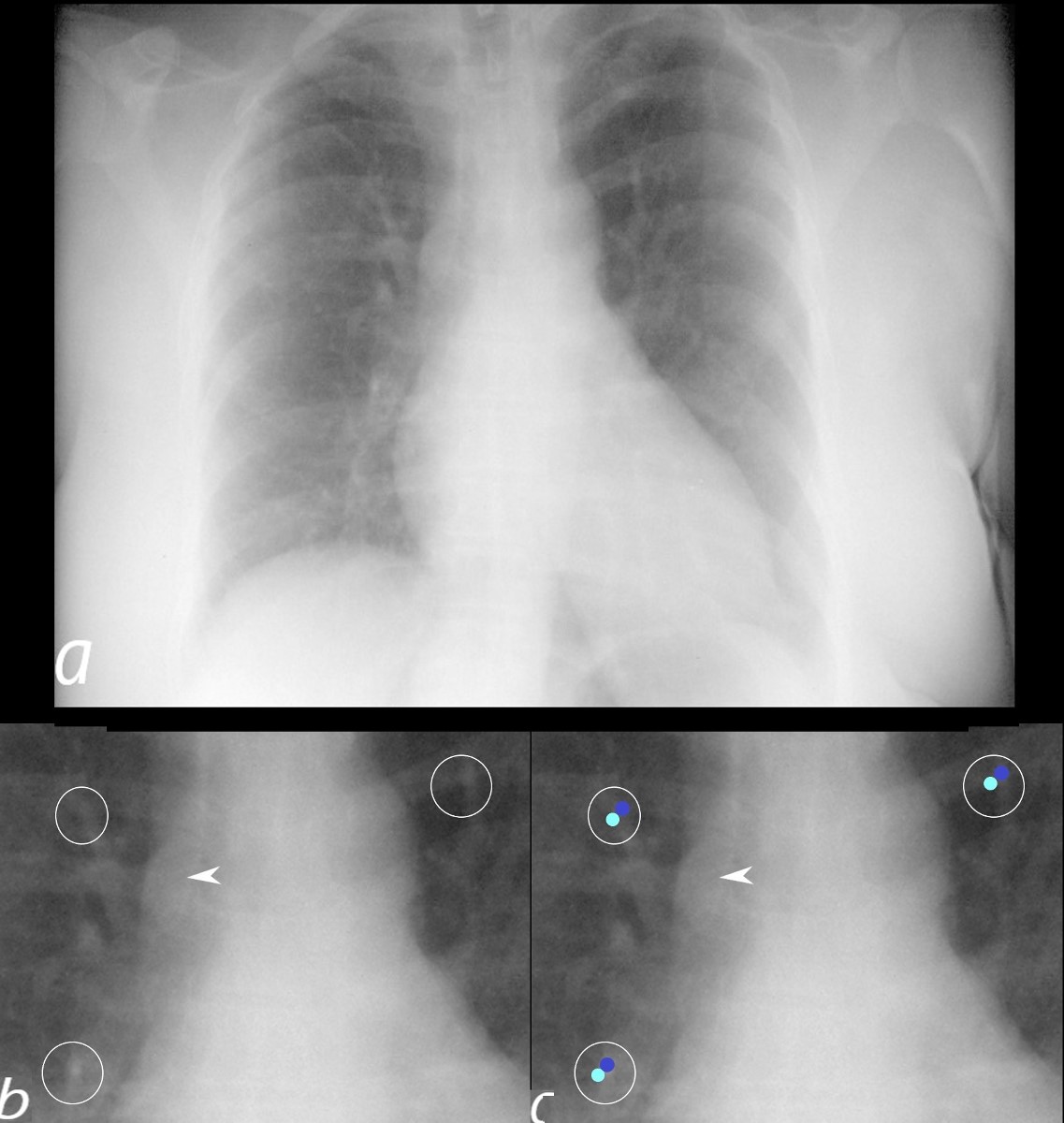
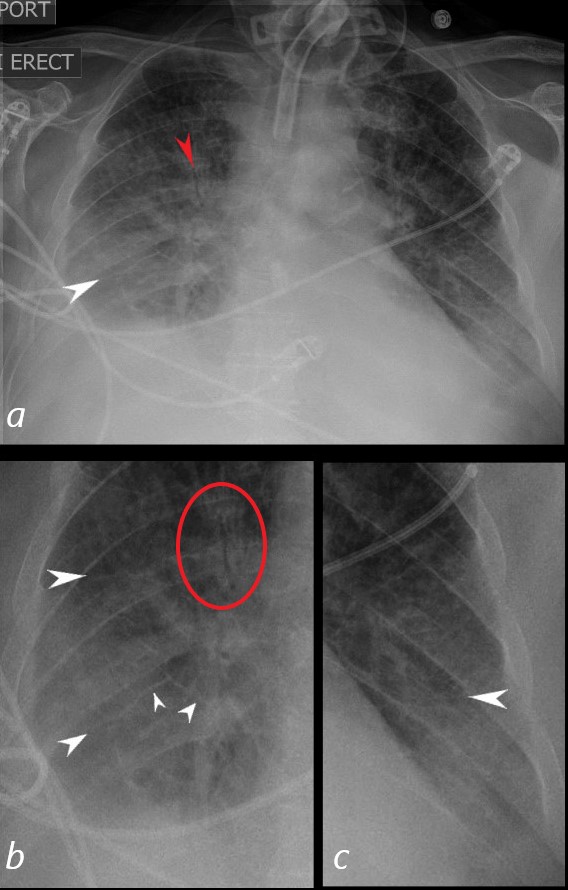
56-year-old female presents with with dyspnea. PA CXR shows possible left atrial enlargement equalization of the pulmonary vessels (ringed in b and c with airways overlaid in teal and arteries overlaid in darker blue in c) and suggestion of left ventricular (LV) enlargement reflecting an approximate end diastolic pressure of between 10 and 20 mmHg
indicating early mild heart failure. The azygous vein is enlarged (white arrowhead b and c) suggesting right heart failure as well.
Ashley Davidoff TheCommonVein.net 16515cL
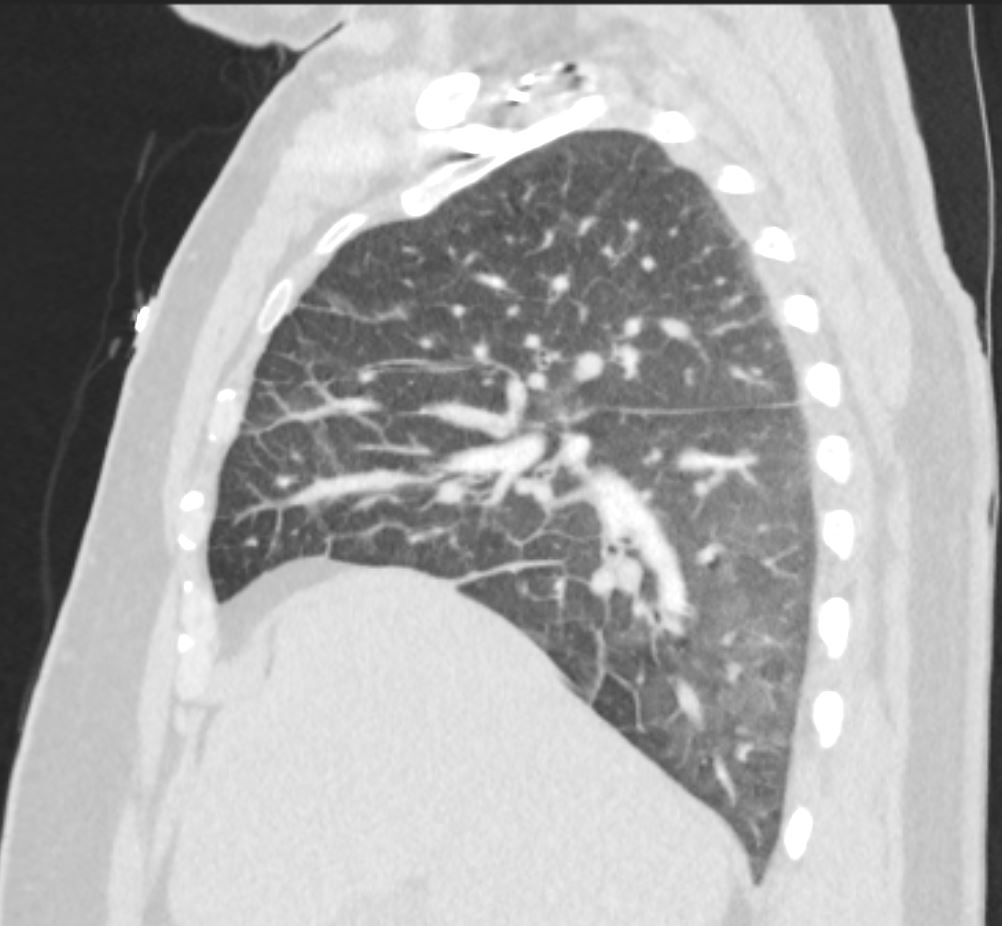

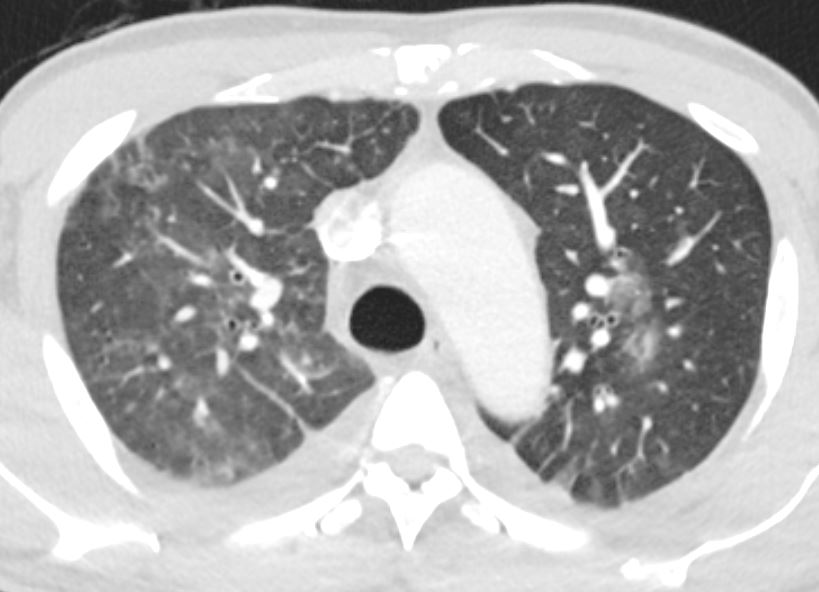
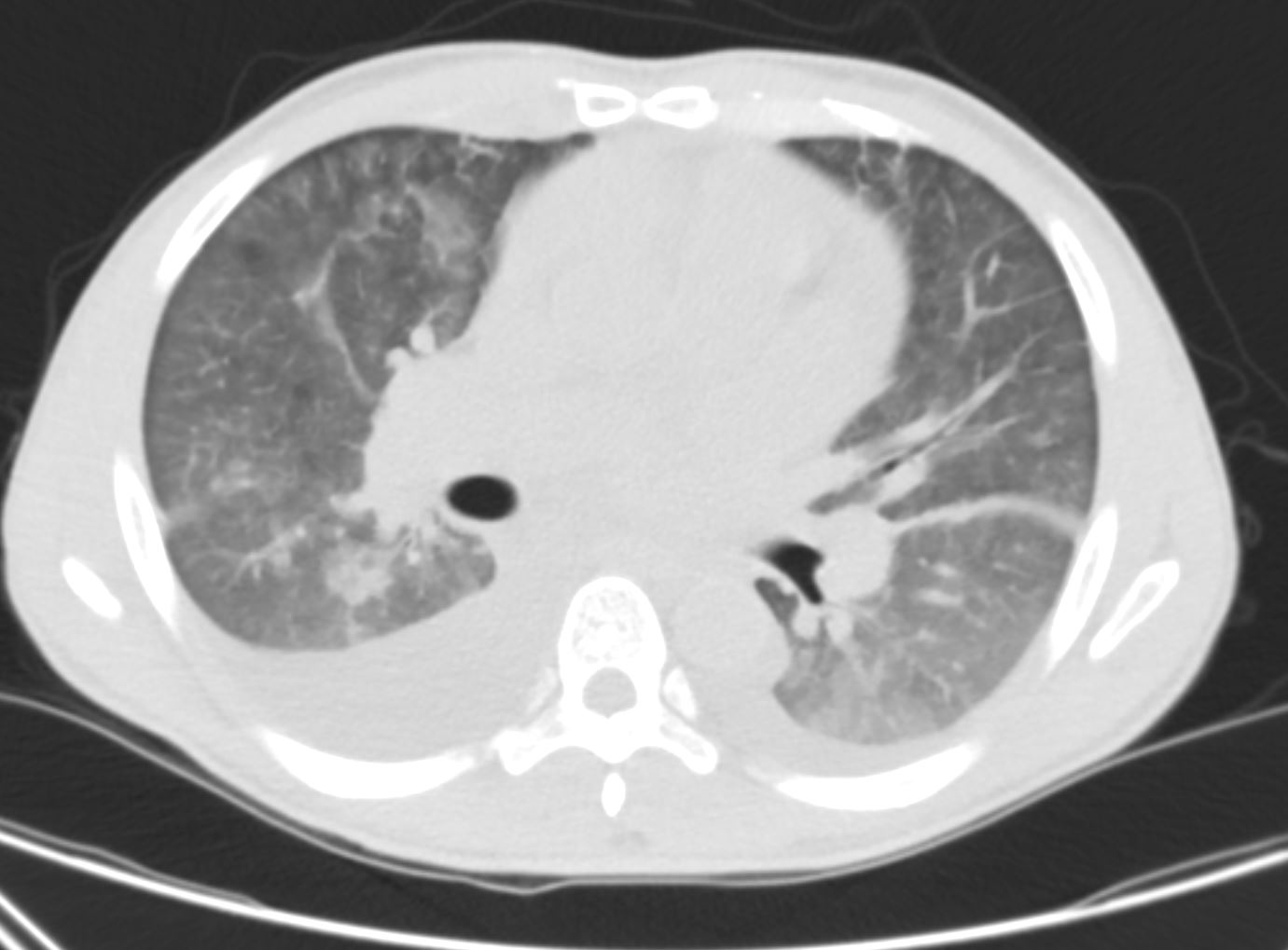
Ground Glass Changes and Bilateral Pleural Effusions
Ashley Davidoff MD TheCommonVein.net CAD-PCI-001a-CT
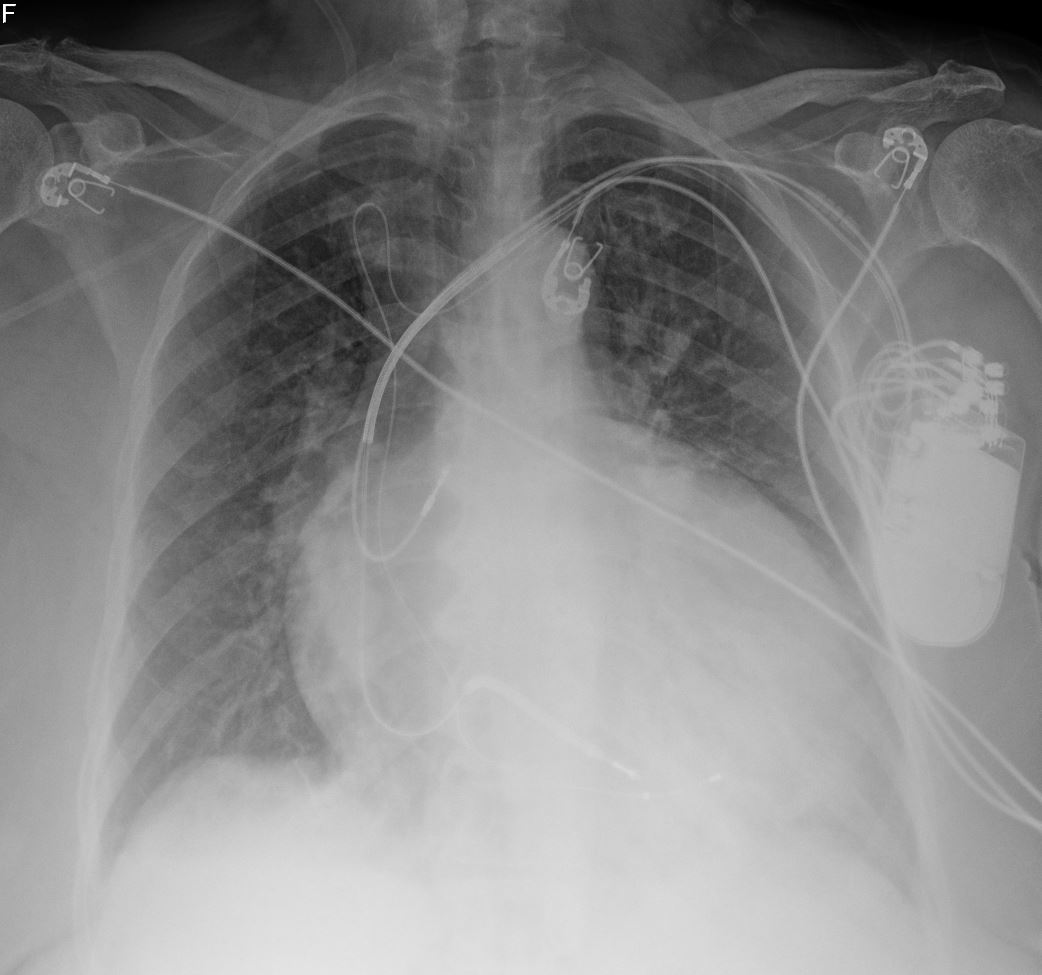
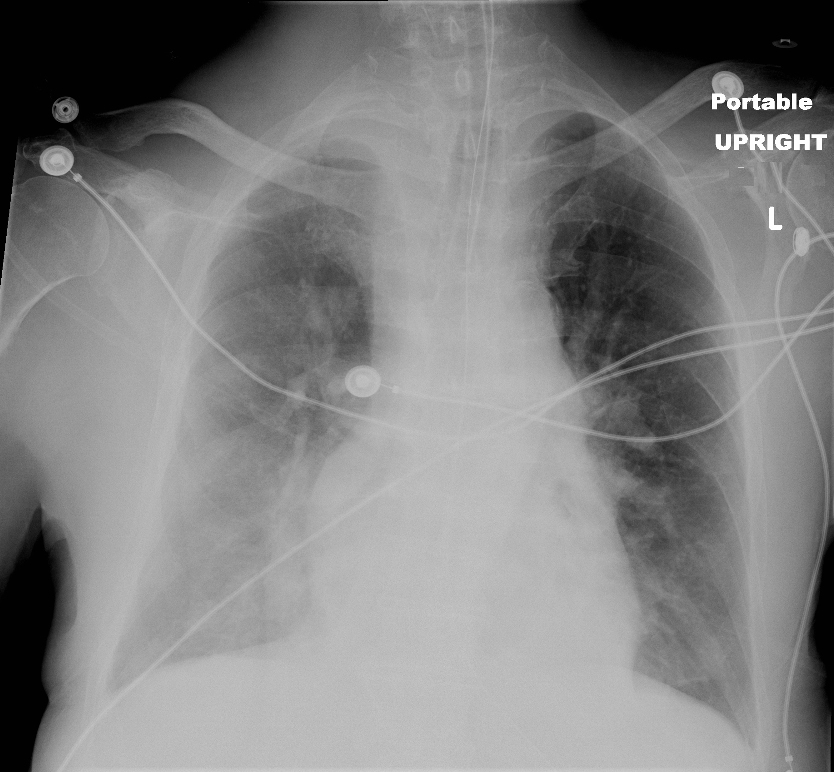
Portable CXR shows cardiomegaly with interstitial edema indicating moderate CHF
Ashley Davidoff
TheCommonVein.net



62-year-old male in the ICU with a tracheostomy and in acute respiratory distress.
CXR shows acute alveolar edema with an air bronchogram in the right upper lobe (red arrow, a), and red circle, b) with peribronchial cuffing around bilateral mid lung bronchi (teal arrows)
Ashley Davidoff MD
62-year-old male in the ICU with a tracheostomy with acute respiratory distress.
CXR shows acute alveolar edema with an air bronchogram in the right upper lobe (red arrow, a), and red circle, b)with Kerley A lines extending from the periphery to the hila and mediastinum (white arrows)
Ashley Davidoff MD

34-year-old male has a normal appearing CXR 1 year before presentation
At the time of his first presentation with dyspnea his CXR showed perihilar infiltrates.
A CT confirmed progressive alveolar edema, with bilateral effusions (right greater than left), mild left ventricular dilatation, Kerley B lines and centrilobular densities and small pericardial effusion.
1 month after this admission a treadmill stress and rest gated SPECT study showed no evidence of ischemia with a calculated ejection fraction of 31%
A repeat CXR showed classical findings of left ventricular dilatation and left atrial enlargement but without CHF
Ct showed early coronary calcification, LAE, LVE and resolution of the pericardial effusion with pulmonary hypertension. Lungs were clear.
MRI confirmed the presence of a dilated cardiomyopathy, small pericardial effusion, without evidence of LGE, global hypokinesis and EF of about 20%
2 years later he presented with acute hemorrhagic pancreatitis that was felt to be related to his CRF
Serial CXRs over 3-4 days showed CHF with cephalization and early interstitial edema.
Echo showed improved LV function with EF of 50%, normal PAP, normal sized chambers, improved since the study performed 2 years earlier.
Repeat CT of the abdomen showed maturing pancreatic pseudocysts, mildly dilated LA, calcified medium sized vessels and calcification of the vasa deferentia
Ashley Davidoff MD
Unilateral Pulmonary Edema Scimitar PAPVR and CHF
66 year old female presents with dyspnea
Frontal CXR shows unilateral right sided pulmonary edema with cephalization of the left upper lung vessels, with evidence of left atrial enlargement, and enlaged main paulmonary artery suggesting pulmonary hypertension secondary to longstanding left to right shunt. In addition there is a curvilinear structure along the right heart border that is shaped like a sword or a scimitar and the right lung appears smaller than the left. These findings are consistent with scimitar sign and scimitar syndrome
The large shunt results in in increased flow to the right lung and therefore accounts for the unilateral edema
Courtesy Ashley Davidoff MD The CommonVein.net 127H 82595.8