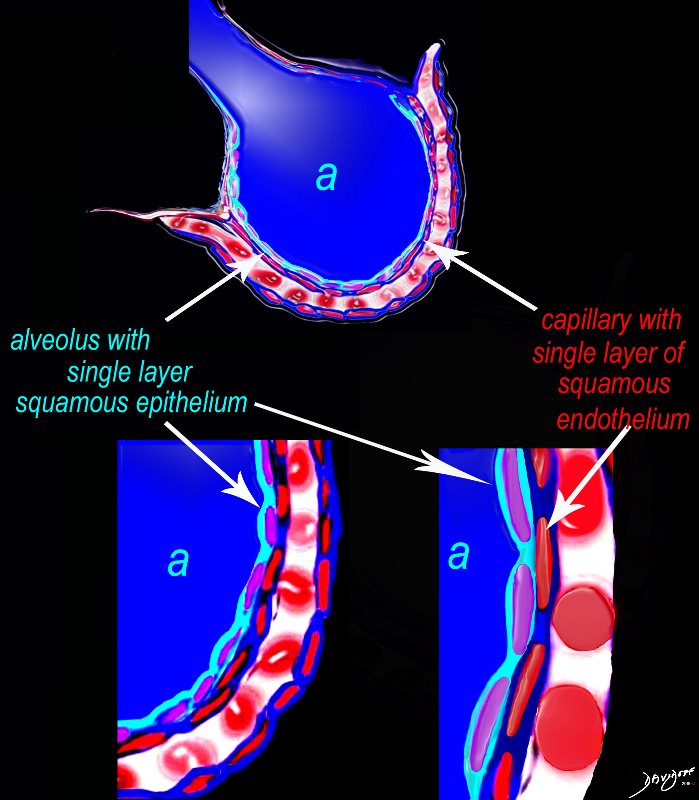
Alveolus at a Cytologic Level The diagram shows an alveolus (a) above, lined by a single layer of squamous cells, surrounded by a capillary with red cells which is also lined by a single layer of squamous endothelial cells . The images below show progressive magnification of the alveolar wall demonstrating the two thin layer of the alveolar membrane . Ashley Davidoff TheCommonVein.net lungs-0028-low res
Pulmonary edema is
caused by the
extravascular movement of fluid into the
pulmonary interstitium and
alveoli.
It is therefore not a helpful term when trying to distinguish between
moderate heart failure ie interstitial edema
severe heart failure – alveolar edema
classified into four categories based on these physiologic
hydrostatic pressure edema, ‘
left heart failure and
volume overload
permeability edema with and without diffuse alveolar damage (DAD)
DAD is acute respiratory distress syndrome,
direct injury to the
capillary endothelium and
alveolar epithelium by
many different causes including
infectious processes,
inhaled toxins,
inflammatory mediators arising from a larger systemic insult.
changes in membrane permeability without severe alveolar damage.
“crack-lung” or
opioid overdose or,
high-altitude pulmonary edema, or
cytokine administration such as IL-2.
both an increase in hydrostatic pressure and membrane permeability.
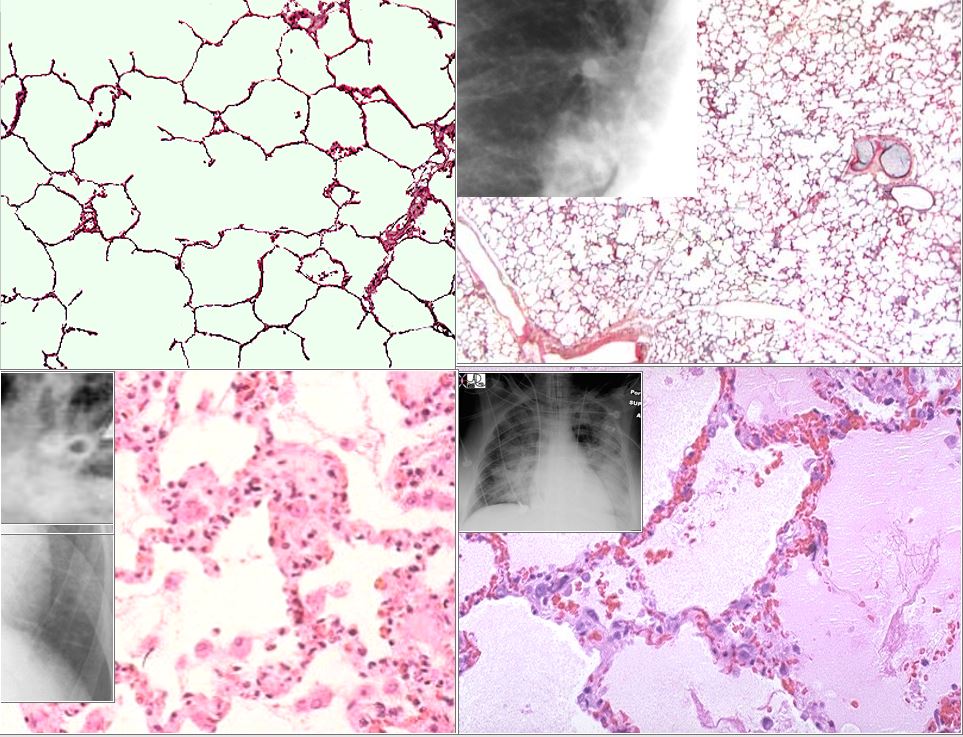
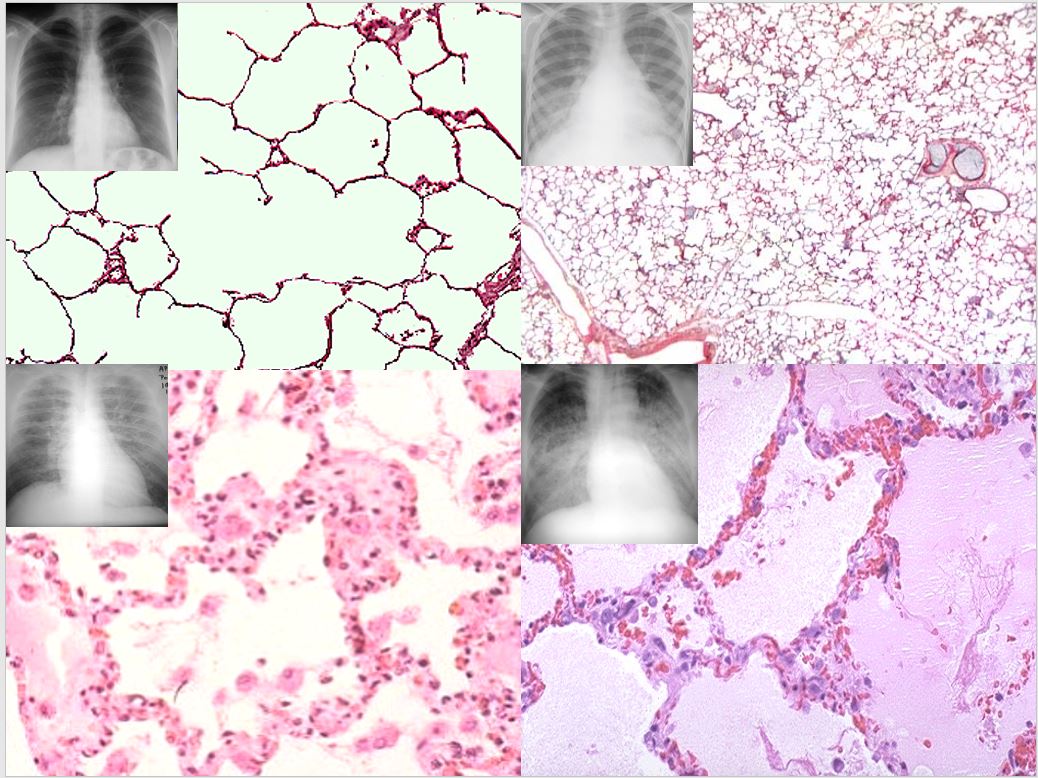
PHASES OF HEART FAILURE The top left image is the a histological section of normal alveoli and normal wall and interstitium. Heart failure occurs when the left ventricular end diastolic pressure rises. There are 3 basic phases of heart failure. in the first phase (top right) the LVEDP rises above 12 mmHg and on an upright CXR there is equalization of the size of the vessels going to the upper lobes and lower lobes. As the LVEDP goes above about 15-18 mm Hg there is cephalization of the vessels and the upper lobe vessels are larger than the lower lobe vessels. The second phase of interstitial edema (bottom left) occurs when the intravascular hydrostatic pressure exceeds the intravascular oncotic pressure and this occurs when the LVEDP goes above 25 mm Hg. Fluid accumulates in the alveolar walls and interstitium and the wall becomes thicker with fluid, and the lymphatics and interlobular septa are distended. The last phase of alveolar edema (lower right) occurs when the pressure exceeds 35 mmHg and the fluid leaks into the alveoli . Ashley Davidoff MD
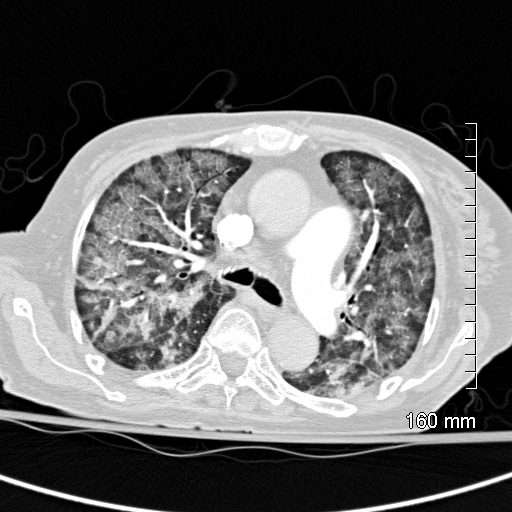
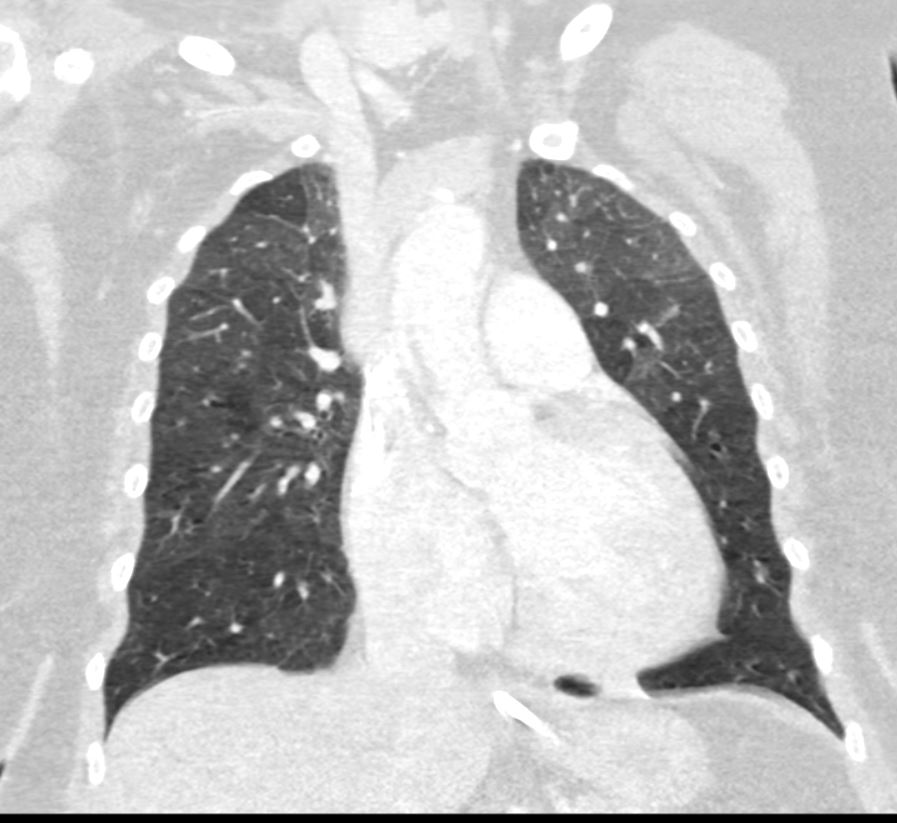
batwing alveolar edema Courtesy Start RadiologyCHF – Alveolar Edema CT scan shows Diffuse ground glass pattern with thickening of the interlobular septa and manifesting as crazy paving pattern Ashley Davidoff MD
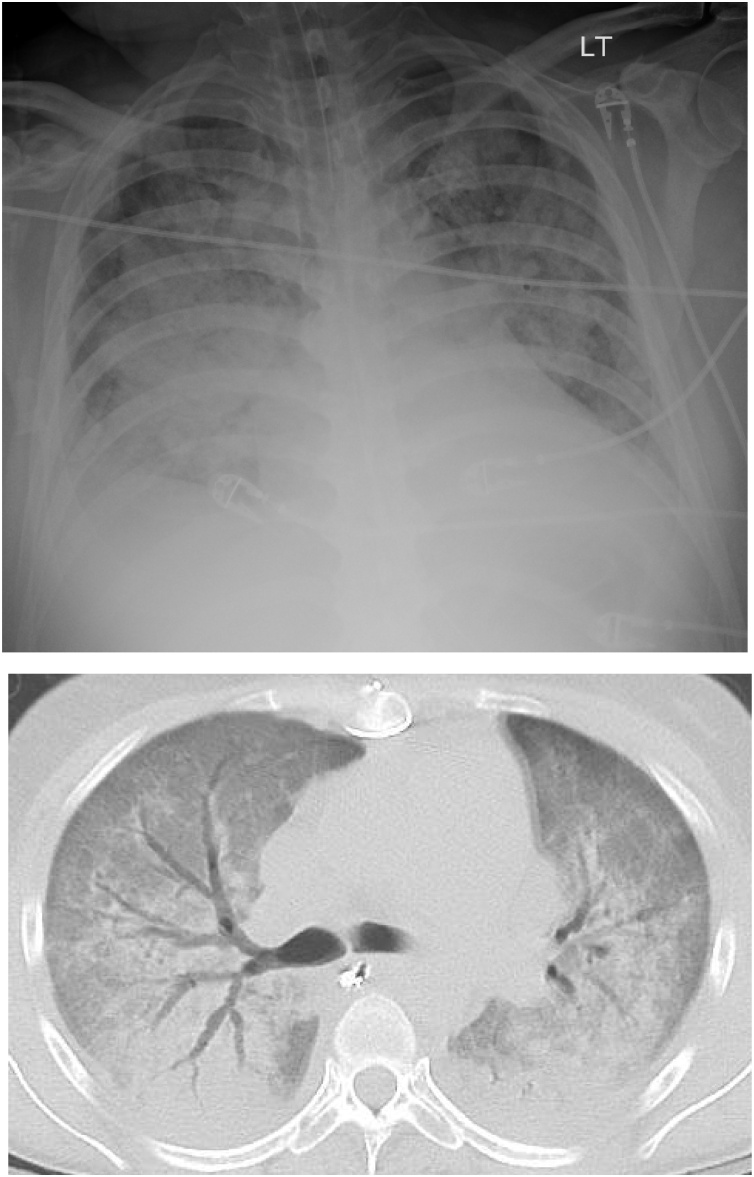
Permeability Edema with and without Diffuse Alveolar Damage (DAD)
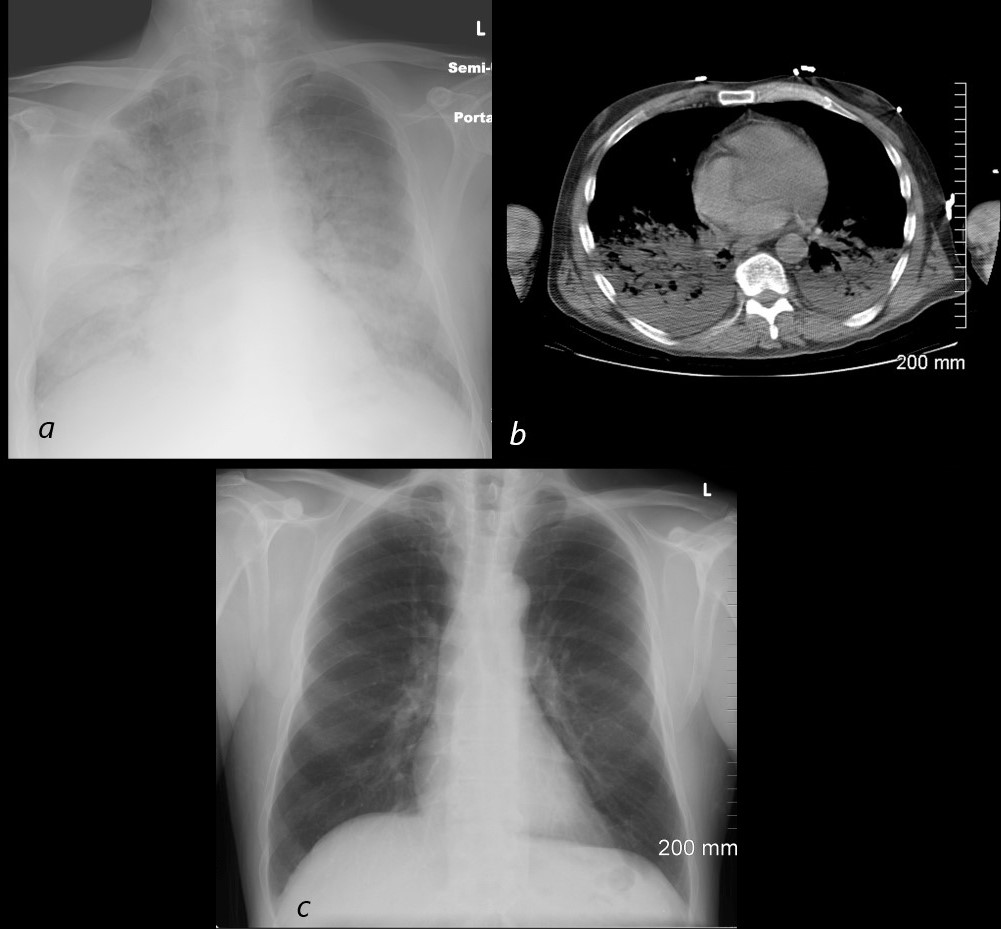
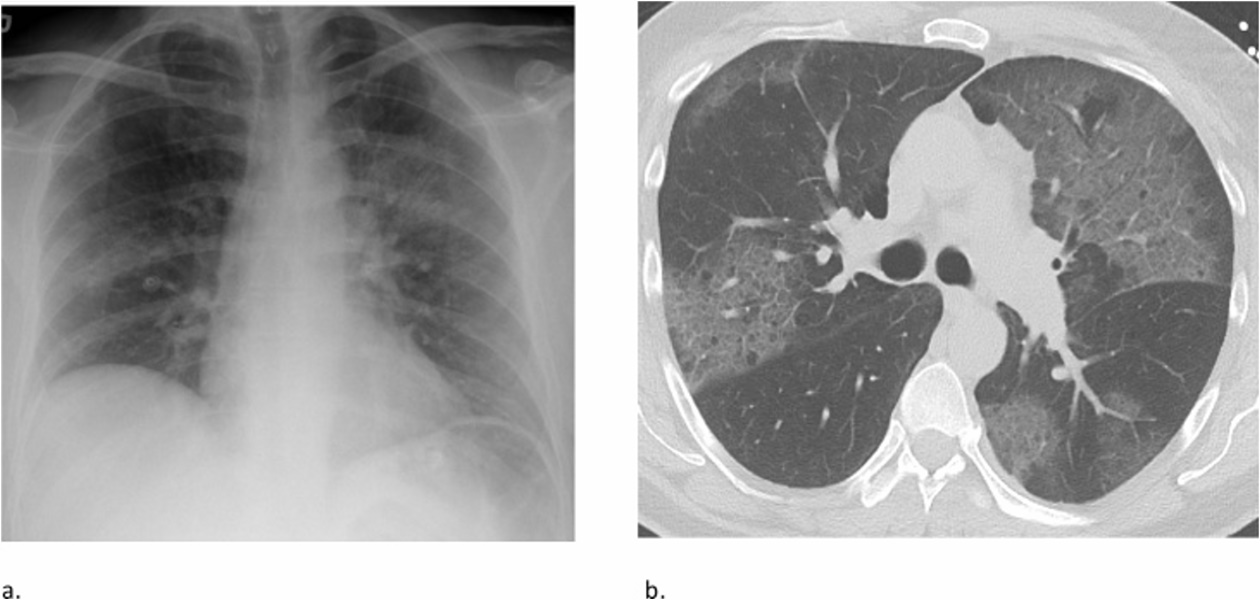
Aspiration Pneumonia Pulmonary Edema and DAD 54 year old male alcoholic with seizures presents with diffuse alveolar disease consistent with pulmonary edema (a). CT scan (b) shows bibasilar infiltrates consistent with aspiration. Follow up CXR 6 months later (c) shows resolution Ashley Davidoff MD TheCommonVein.net
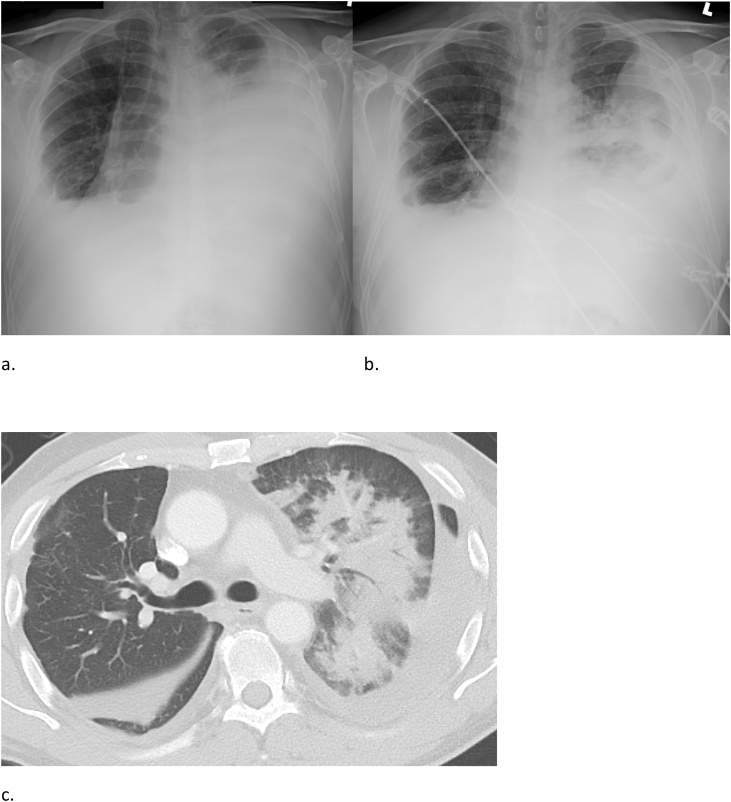
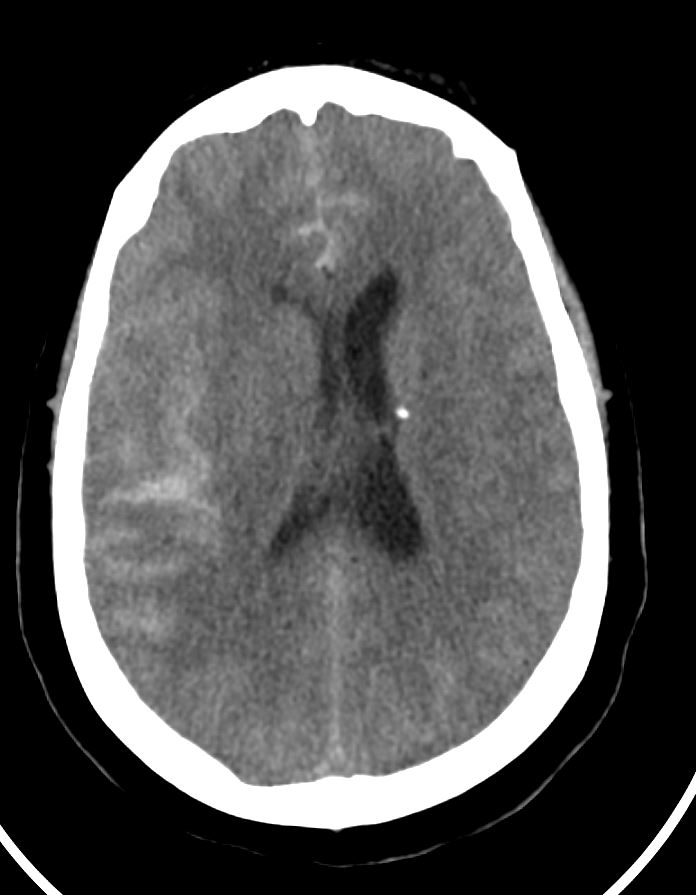
54 year old female with subarachnoid hemorrhage with mild pulmonary edema Ashley Davidoff TheCommonvein.net54 year old female with subarachnoid hemorrhage with mild pulmonary edema Ashley Davidoff TheCommonvein.net
54 year old female with subarachnoid hemorrhage with mild pulmonary edema Ashley Davidoff TheCommonvein.net