
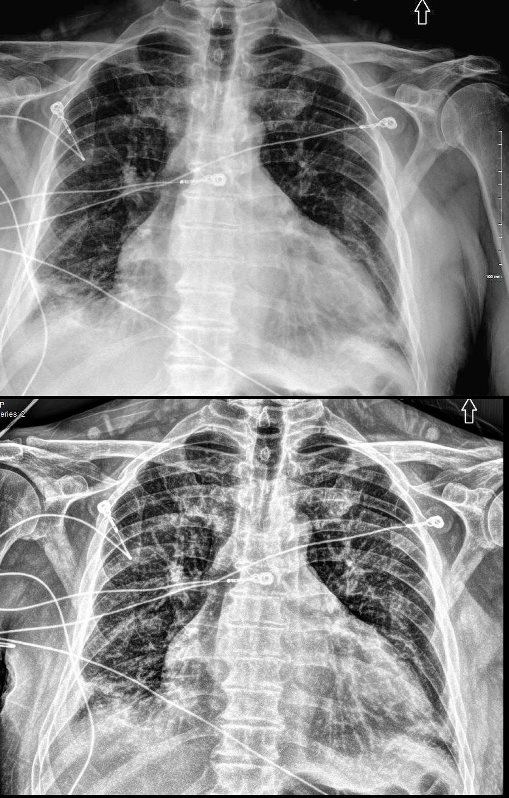
59 year old man with history of scleroderma (clinically noted to be definite), Raynaud’s phenomenon, and question RA and possibly a mixed tissue disorder, (on Plaquenil), recent admission for pneumonia presents with symptoms of heart failure with the following cardiovascular history:
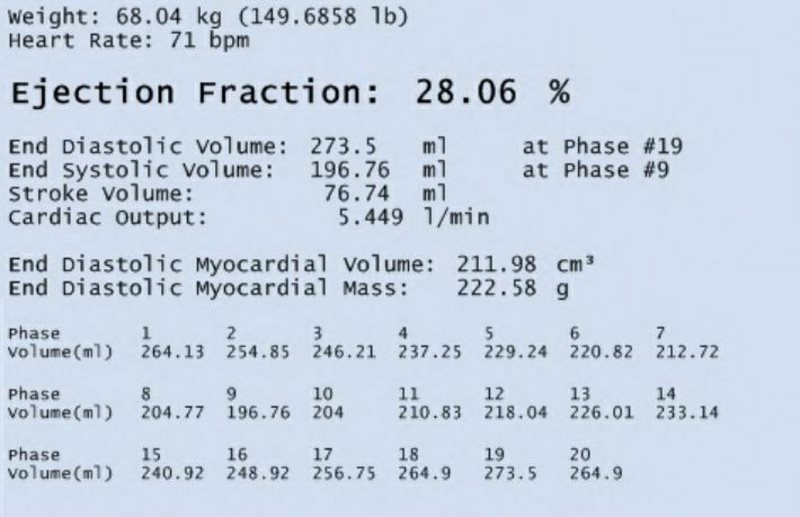
Non ischemic cardiomyopathy, with both diastolic and systolic failure, with normal coronary arteriogram, atrial fibrillation, an echo showing an EF of 20-25% with abnormal diastolic function, biatrial enlargement, mild MR normal pulmonary artery pressure, and normal RV function and size. Left ventricular hypertrophy with LV mass of 144g/sq m
Right heart catheterization for biopsy showed RA 4/3, RV 27/0 PCW of 9, PA 32/9
Anti-cyclic citrullinated peptide (anti-CCP) an antibody present in most rheumatoid arthritis was elevated and hand X-ray suggested an erosive osteoarthritis, reminiscent of RA or RA related arthropathy.
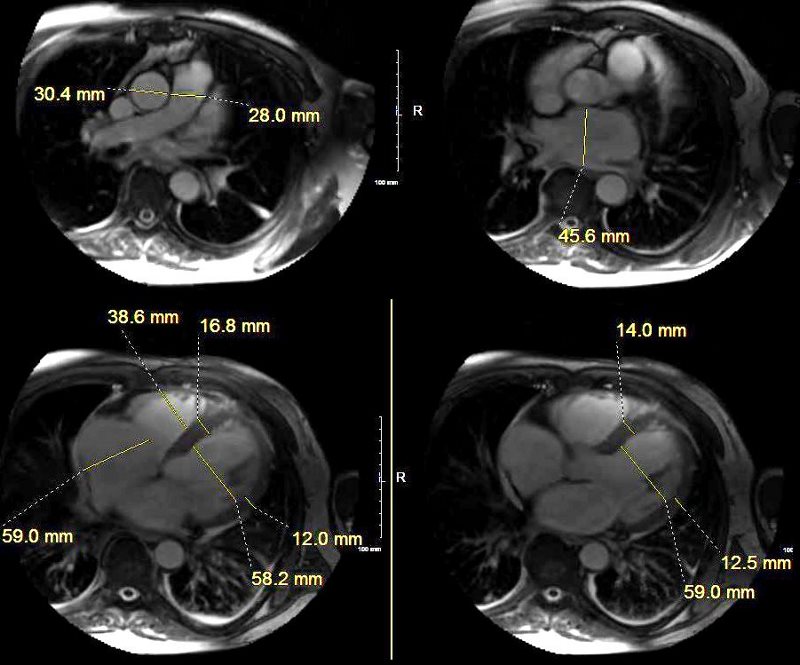
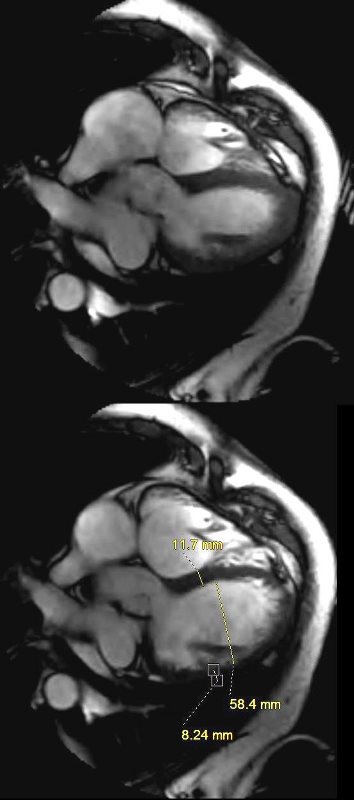
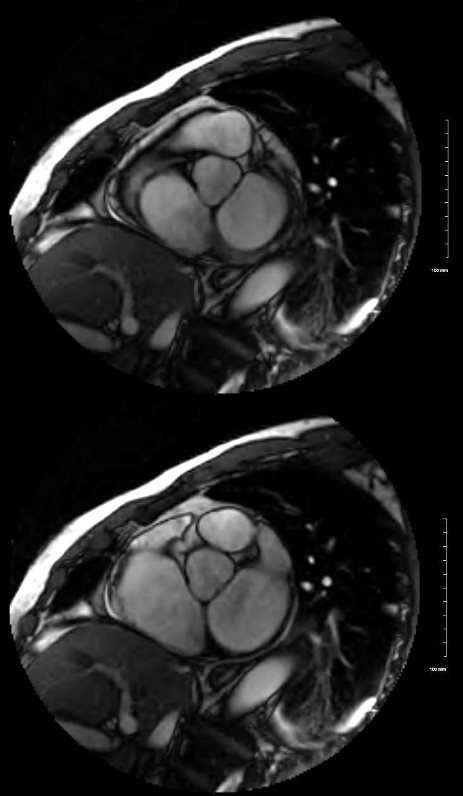
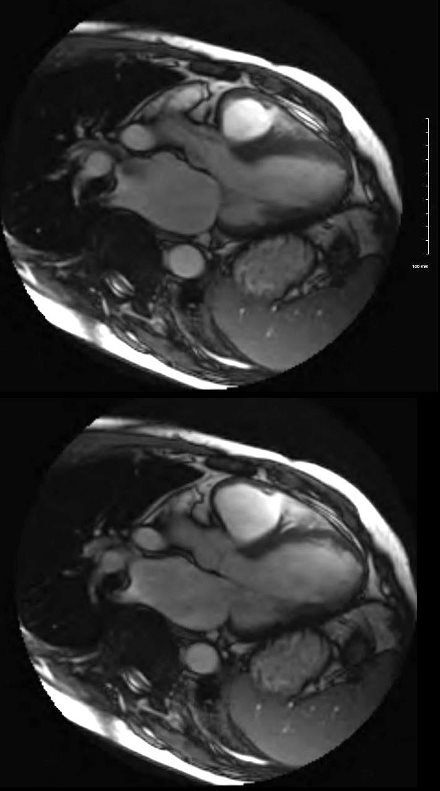
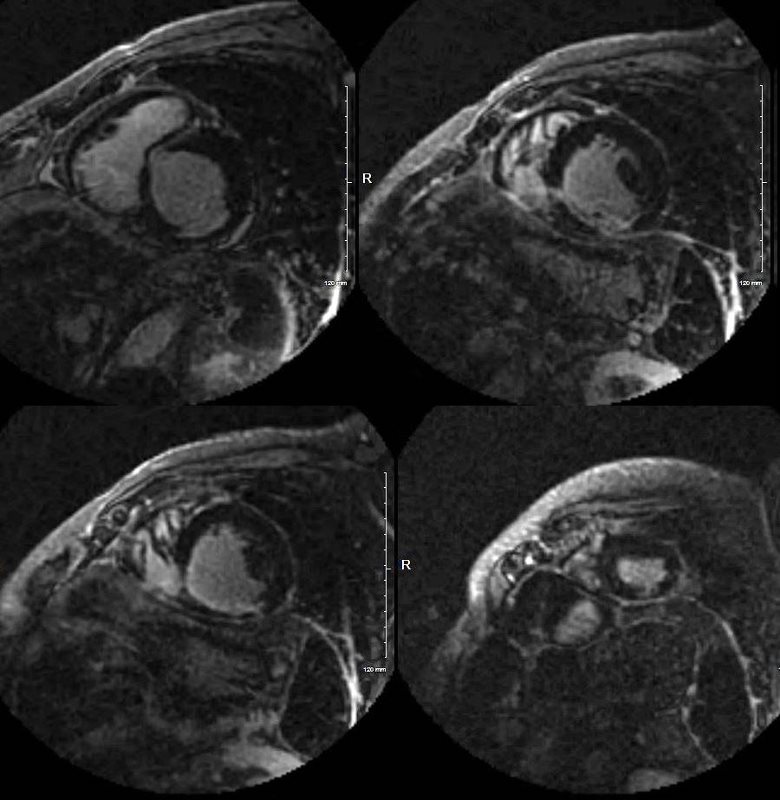
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD

Ashley Davidoff MD

Ashley Davidoff MD

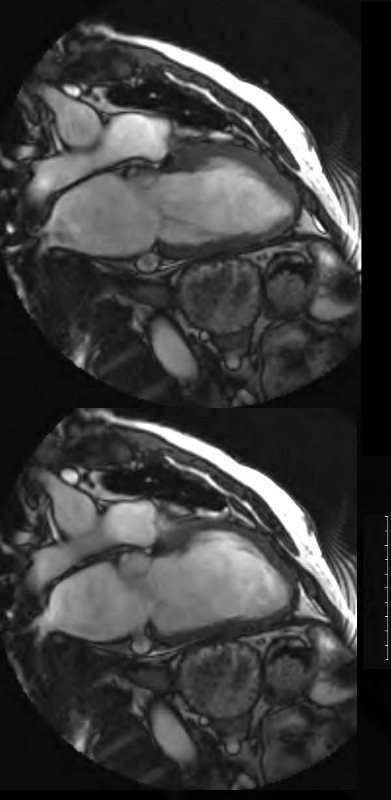
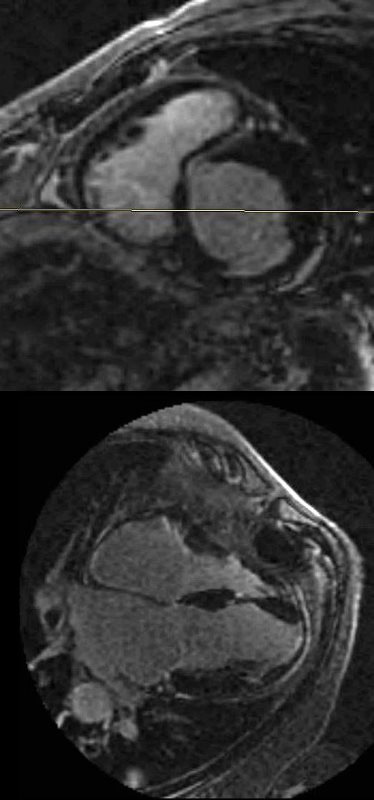
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD

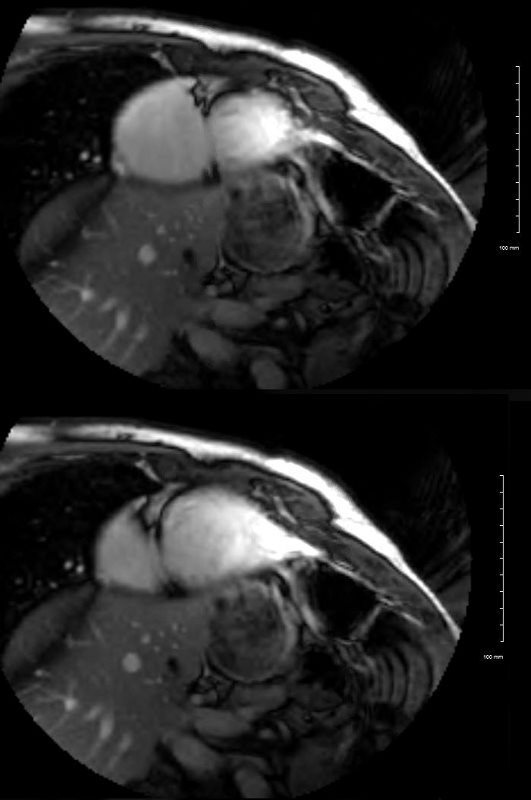
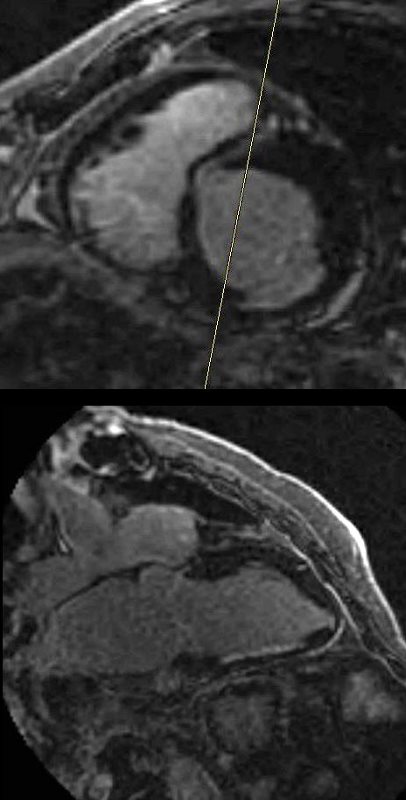
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
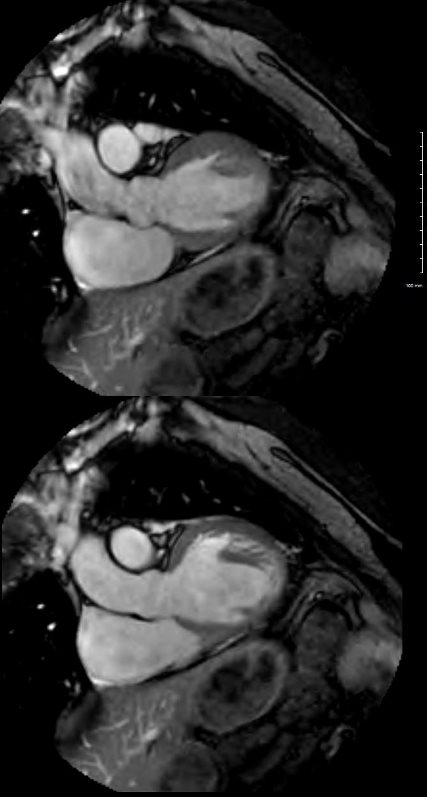
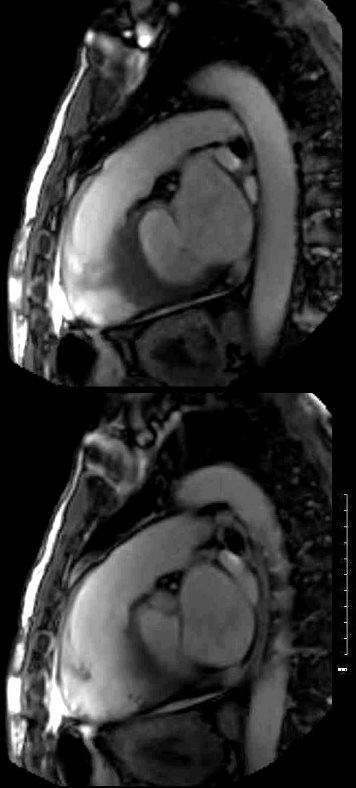
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
Right heart catheterization for biopsy showed RA 4/3, RV 27/0 PCW of 9, PA 32/9
Anti-cyclic citrullinated peptide (anti-CCP) an antibody present in most rheumatoid arthritis was elevated and hand X-ray suggested an erosive osteoarthritis, reminiscent of RA or RA related arthropathy.
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD

MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD
MRI showed LV mass of 113g/m sq and extensive subendocardial LGE involving apex, and inferior wall with minor mid myocardial nodular LGE at inferior septal region and linear in the anterior wall
Endomyocardial biopsy showed myocardial hypertrophy mild interstitial subendocardial fibrosis, no amyloid, nor inclusion bodies but with intracellular lipofuscin pigment
Ashley Davidoff MD