Abnormal myocardial perfusion SPECT scan, with reversible ischemia
of the anterior septal wall and at the apical cap.
2. Global left ventricular systolic function was abnormal with global
hypokinesis and with post-stress LVEF of 28%.
3. Regional left ventricular systolic function was abnormal with
septal and inferior wall hypokinesis.
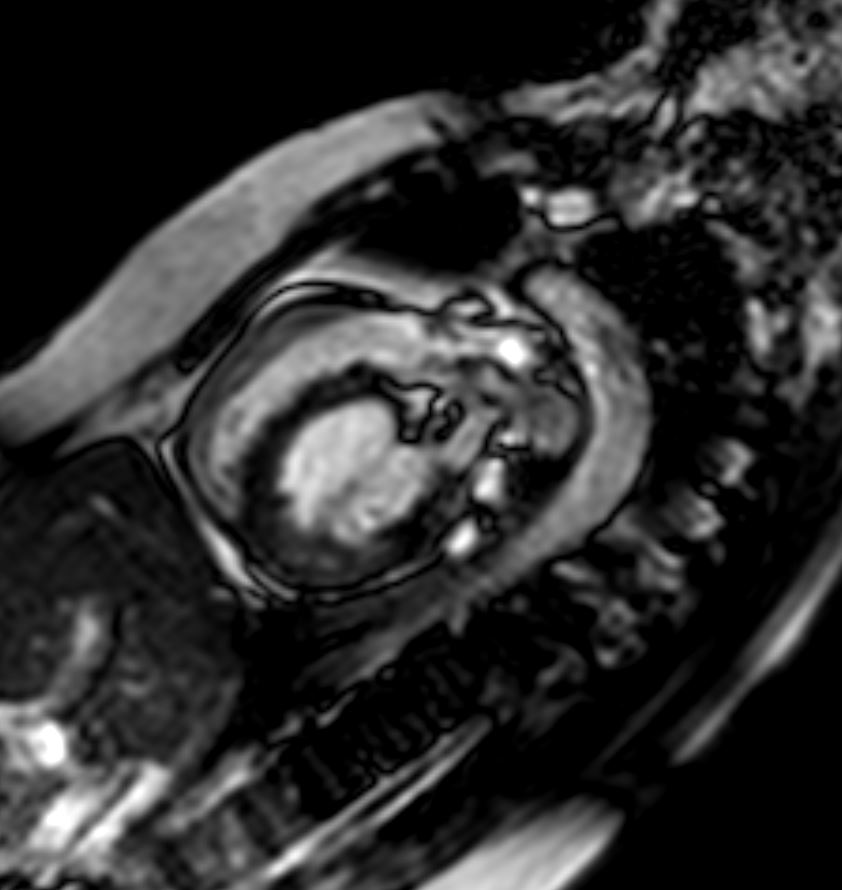
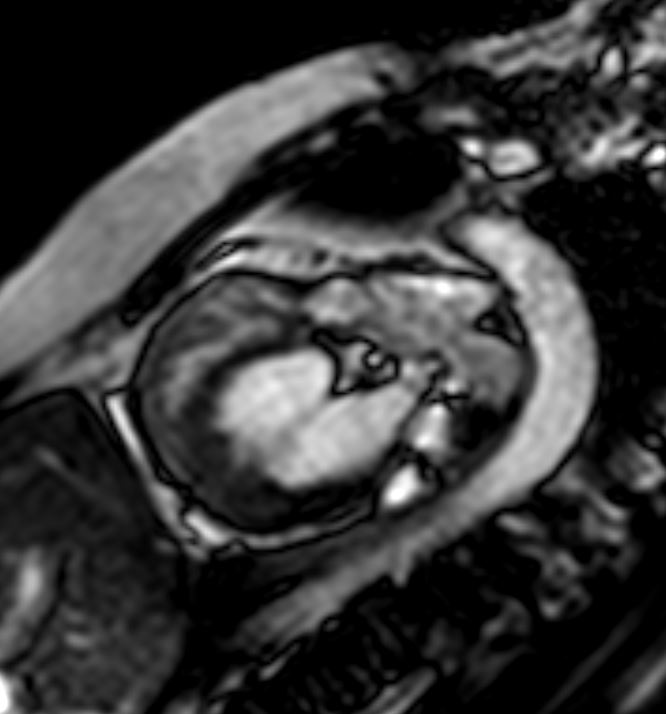
MRI
1. The LV is moderately enlarged with moderately depressed systolic
function, LVEF: 37 %.
2. The RV is normal in size with normal systolic function, RVEF: 62 %.
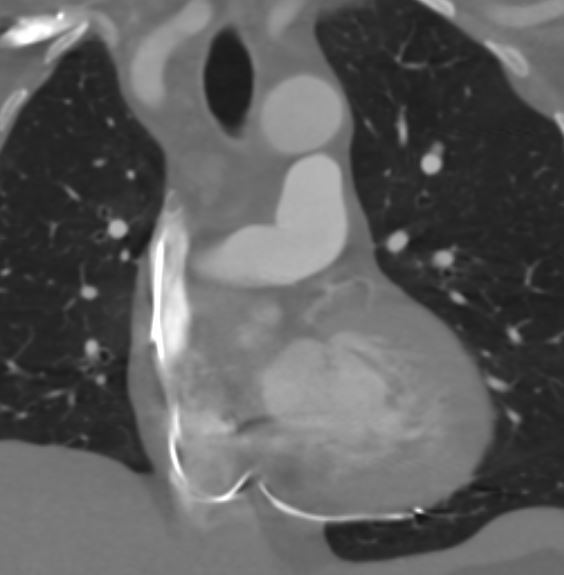
3. No anatomic obstruction or flow acceleration was seen in the RVOT
or proximal PA (right PA was well seen, but left PA was not well
seen).
4. Flow acceleration and turbulence were seen at the level of the
pulmonic valve, suggesting that there is valvular pulmonic stenosis.
Non ischemic cardiomyopathy
EF 20-25% ( 2/2023)
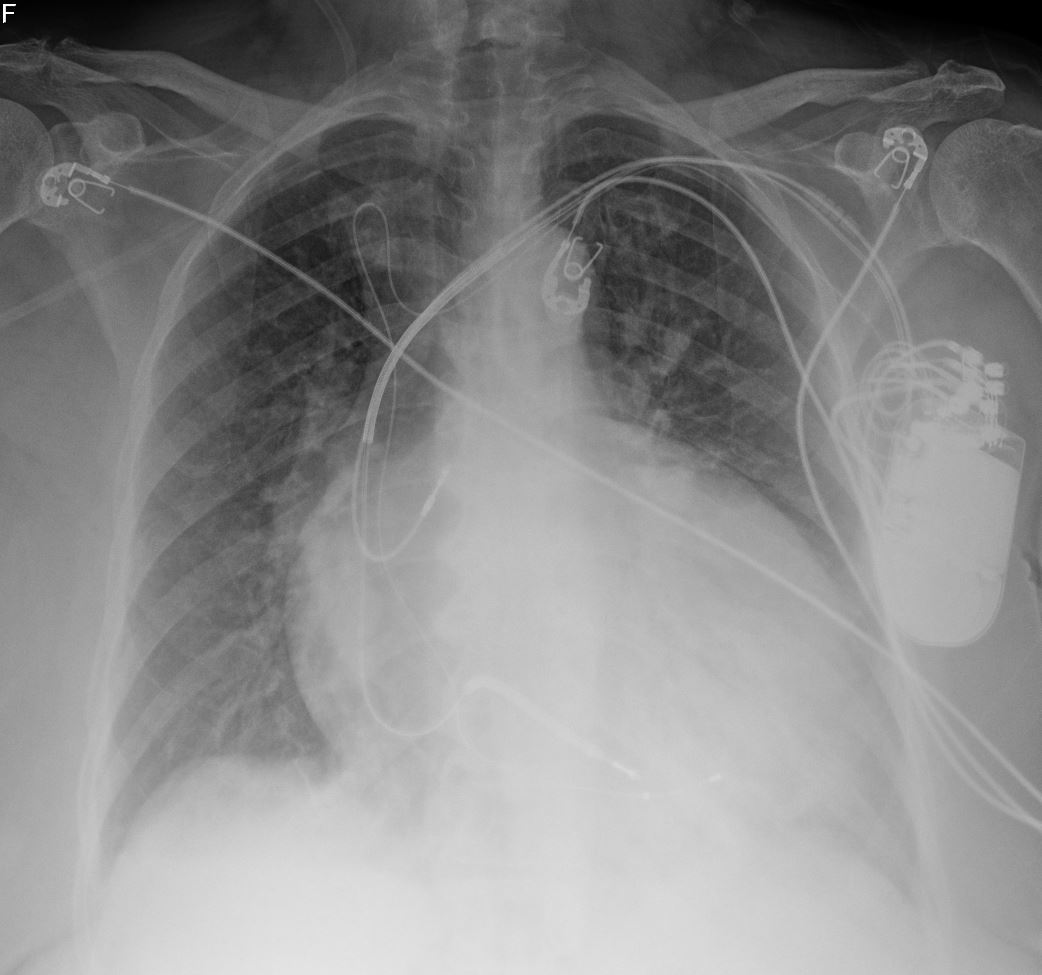
s/p CRTD placement,
Cath from 3 years ago
Normal coronary arteries
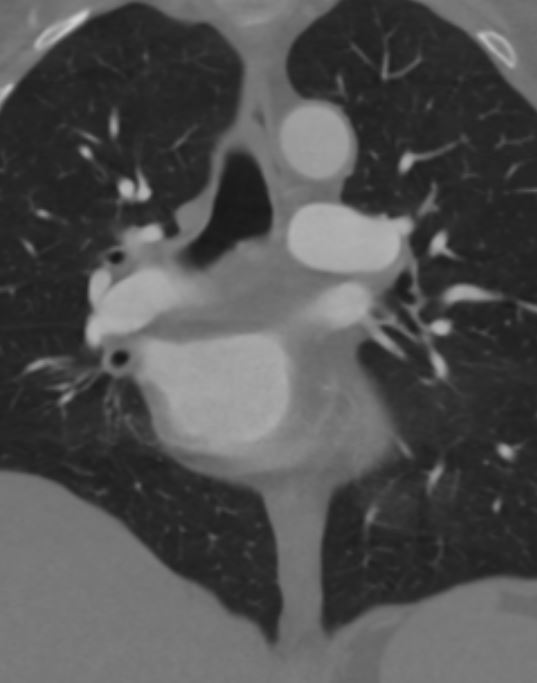
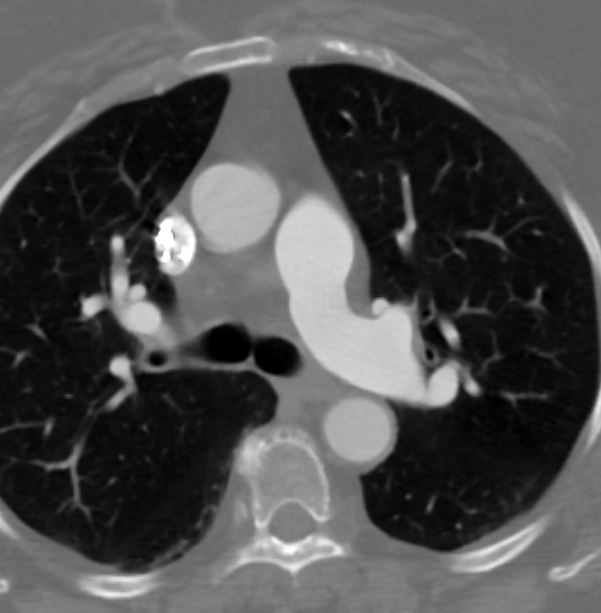
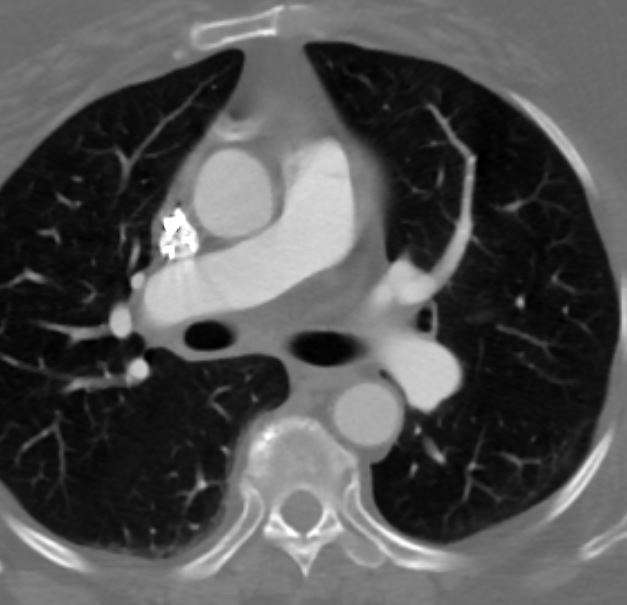
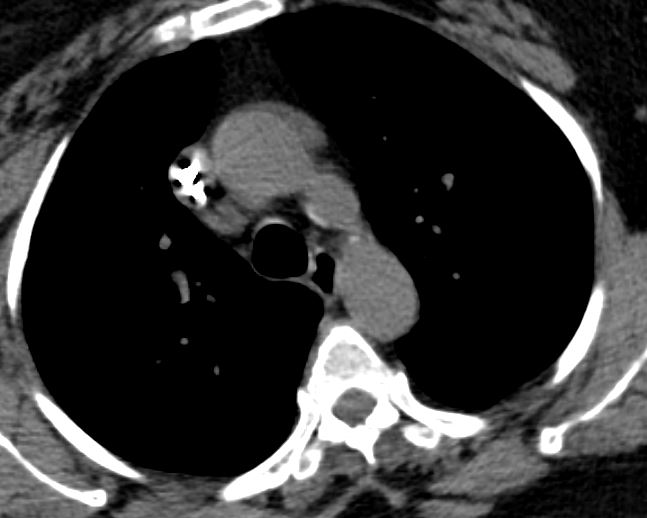
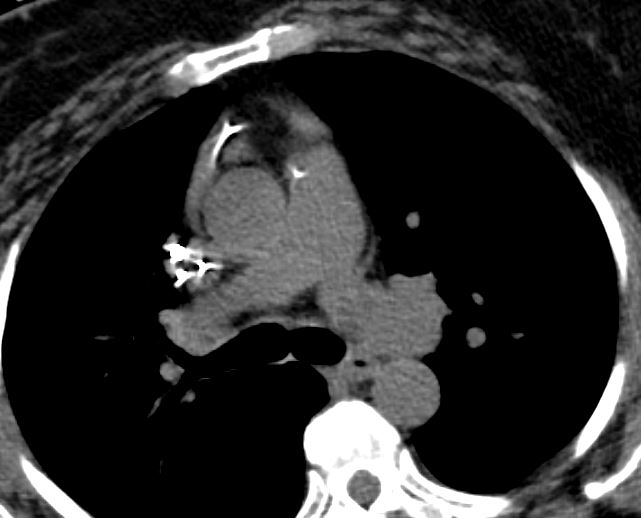
Congenital heart disease: Mild supravalvular stenosis (peak to peak
< 20 mm Hg)
Hemodynamics – PCWP & LVEDP Top-Normal