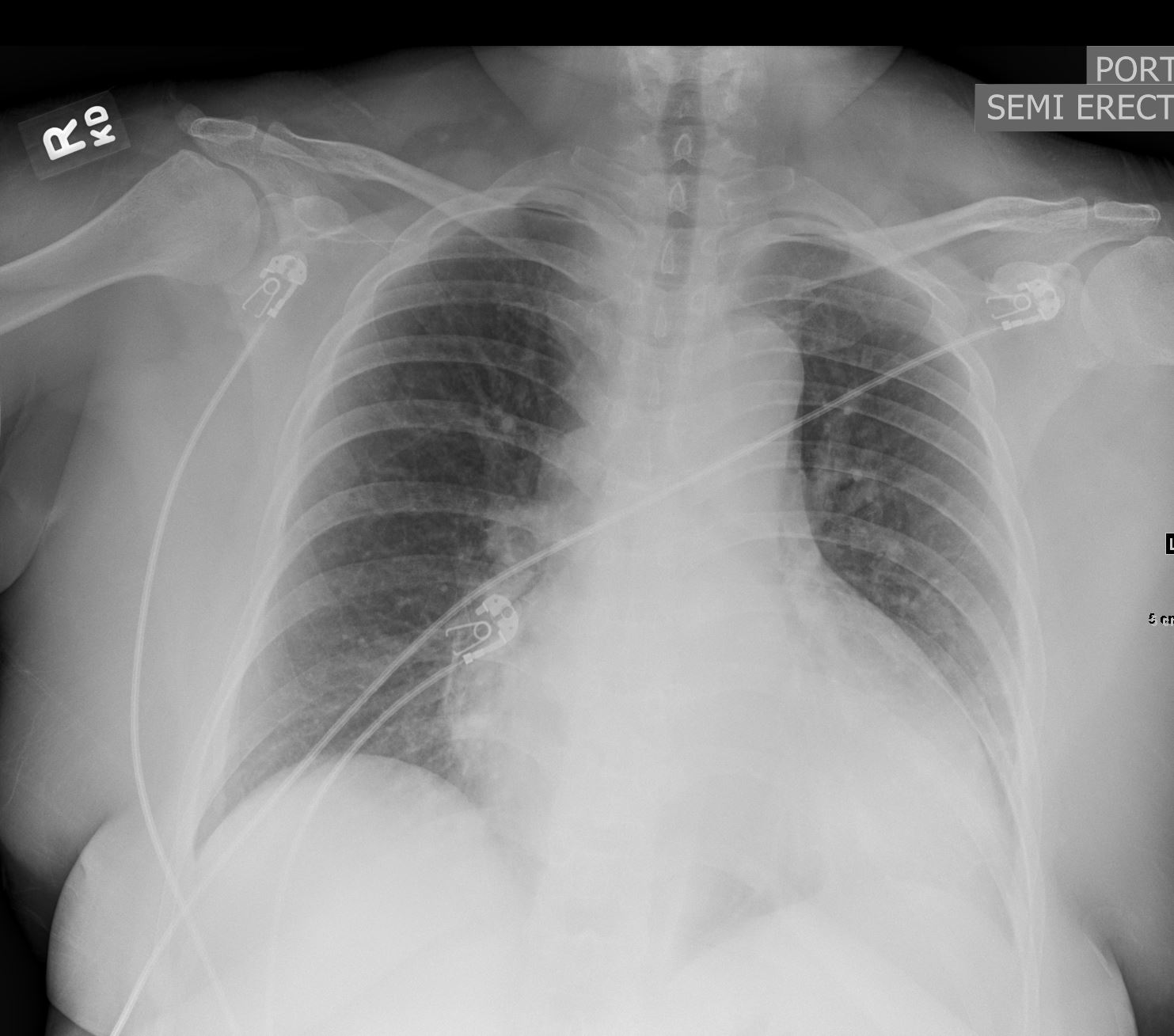
- 40 y.o. female
- 10/10 chest pain
- substernal tightness n/v diaphoresis
- ST elevation in the inferior leads
- progressing to
- new ST depressions
- ST elevations
- in II, III, aVF, new TWI in I and aVL
- code STEMIPMHx significant for HTN, ESRD on HD, and obesity.
- ascending aortic dissection s/p emergent repair
- Cardiac cath showed suspected aortic dissection.
-
- INDICATIONS:
STEMICORONARY CIRCULATION:
Right Dominant
Left Main: Normal
LAD:
Left Anterior Descending: Normal
LCX:
Left Circ: Normal
RCA:
RCA: Occluded by dissection flap
- INDICATIONS:
- CTA confirmed an aortic dissection and patient was taken to the operating room emergently.
-
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net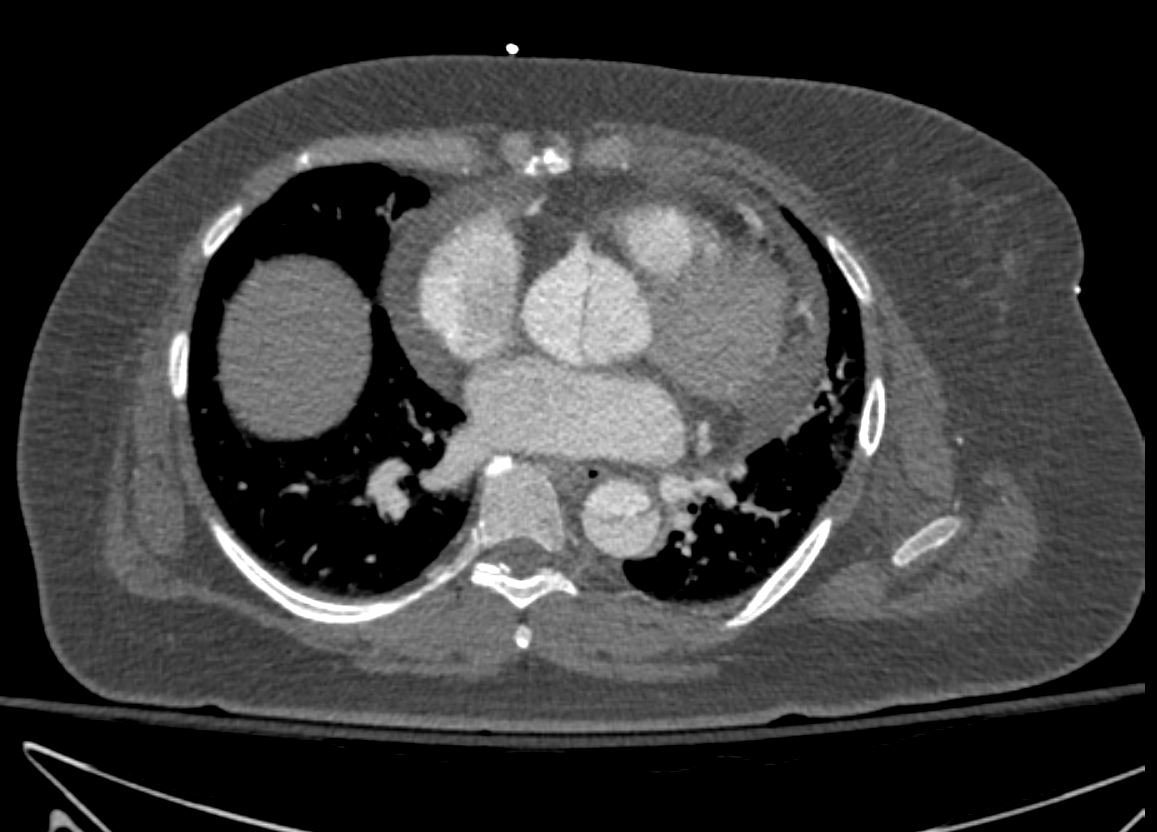
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net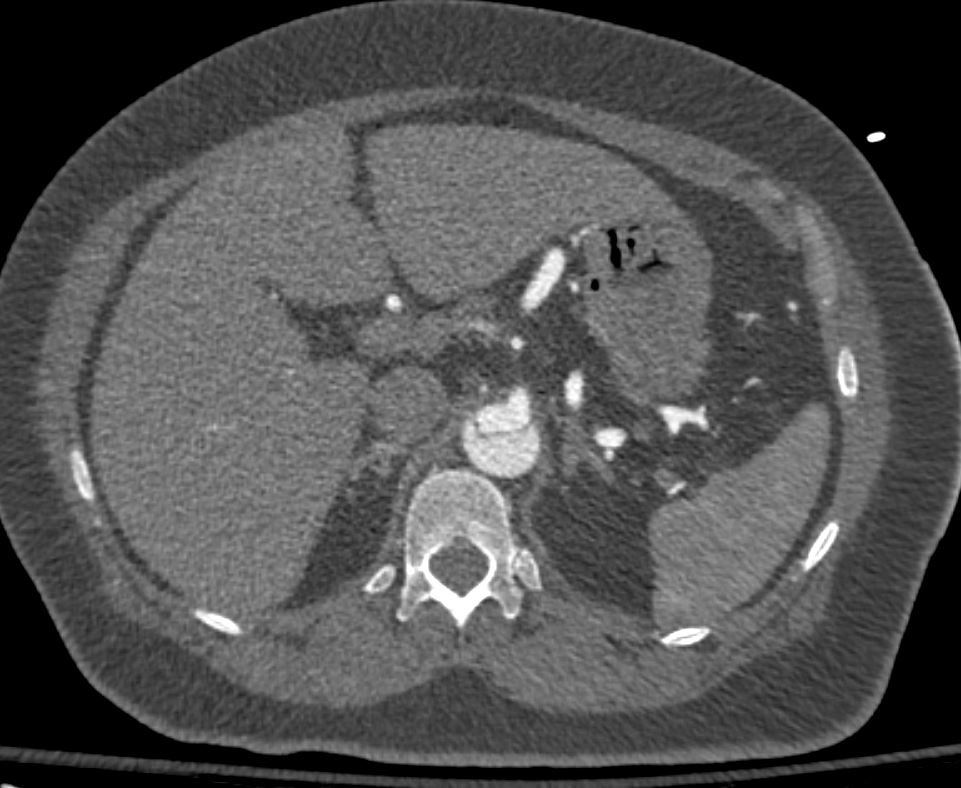
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net
40 year old female Type A dissection with RCA and left renal artery dissection
Ashley Davidoff
thecommonvein.net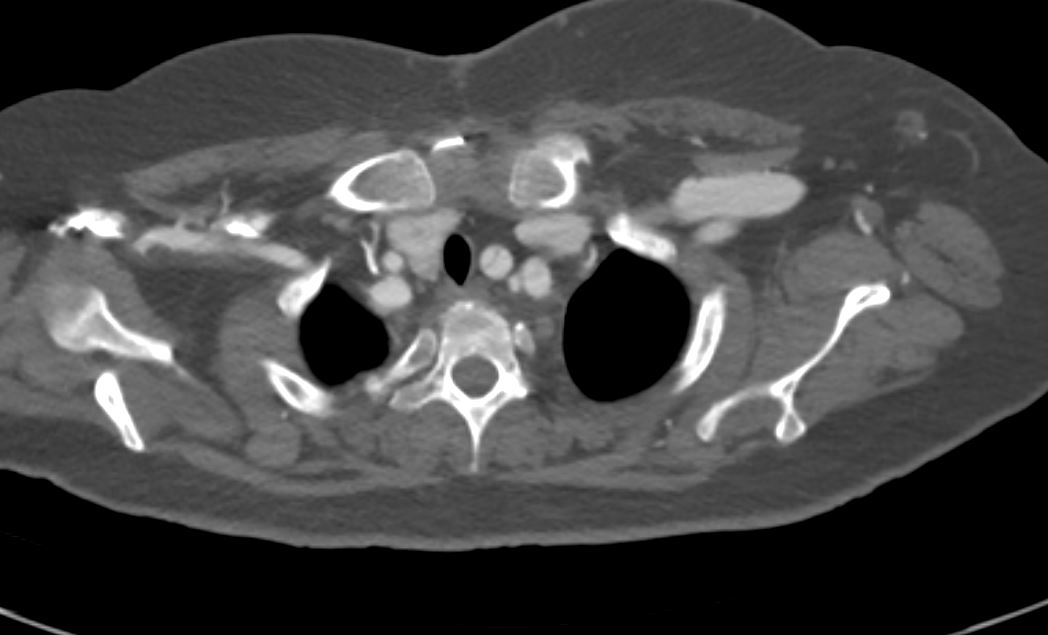
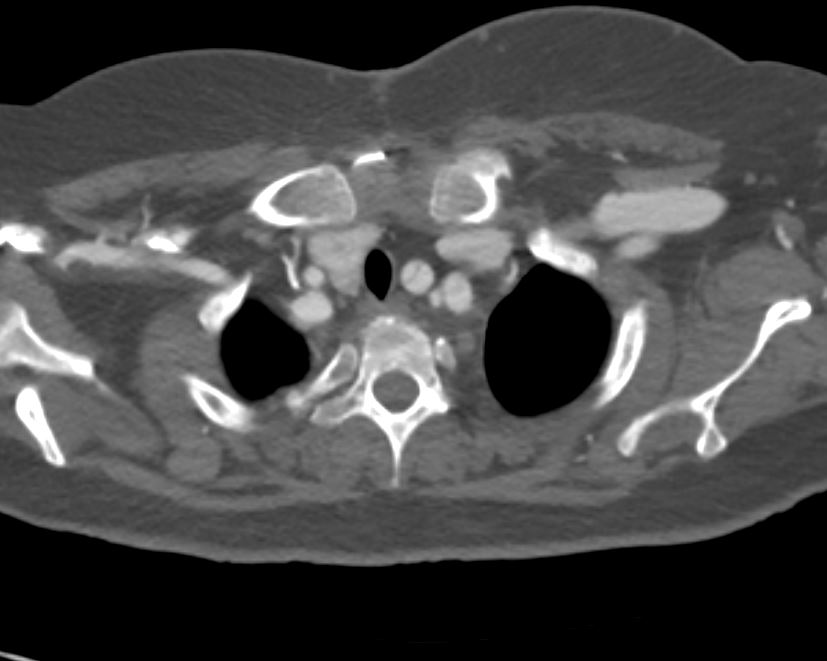
40 year old female Type A dissection with left common carotid and left subclavian artery dissection
Ashley Davidoff
thecommonvein.net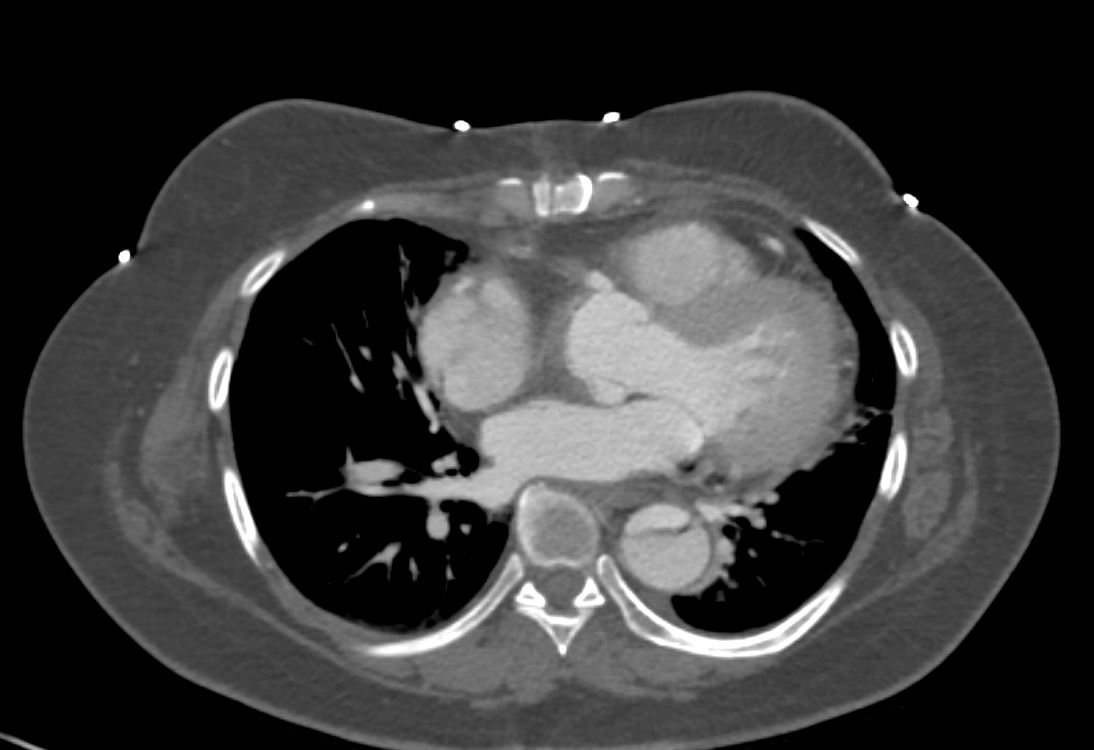
40 year old female Type A dissection post op reimplantation of RCA
Ashley Davidoff
thecommonvein.net - OR
- emergent repair of Type A Aortic Dissection,
- hemi arch repair,
- post op
- bilateral foot, R lower leg, right thigh and RUE purpuric non blanching painful lesions and bilateral foot and hand burning pain right after the surgery with concerns for atheroembolism vs reperfusion injury. Per Vascular surgery and vascular medicine, they are most likely due to reperfusion injury vs atheroemboli. ABI showed no evidence of malperfusion. DP intact b/l, sensation is intact on b/i lower extremities/feet and imaging are stable, they recommend supportive management, and discussed that we would expect resolution over the next few weeks.
-
- rheumatology clinic for initial evaluation for possible
- cryoglobulinemic vasculitis in setting of
- retiform purpura of BLE
