
Copyright 2020
Introduction
Corona = Crown or wreath from mid 17th century (in the sense ‘resembling a crown’): from Latin coronarius, from corona ‘wreath, crown’.

Corona = Crown or wreath from mid 17th century (in the sense ‘resembling a crown’): from Latin coronarius, from corona ‘wreath, crown’.
Courtesy Ashley Davidoff MD
3D
Scaffolding of the Heart
Basic Structure – a Cross Made of Two Intersecting Circles

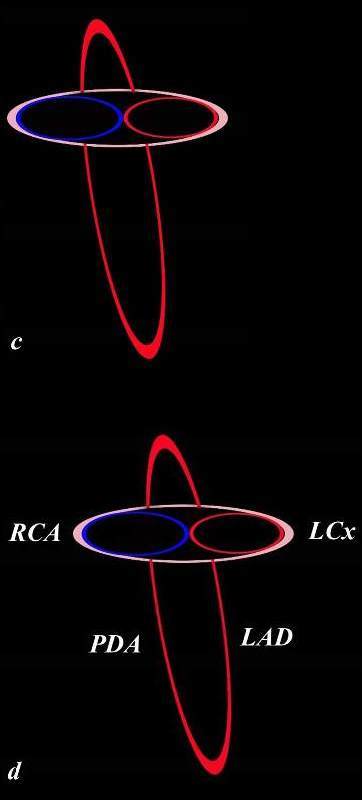
The Cross in 3 Dimensions
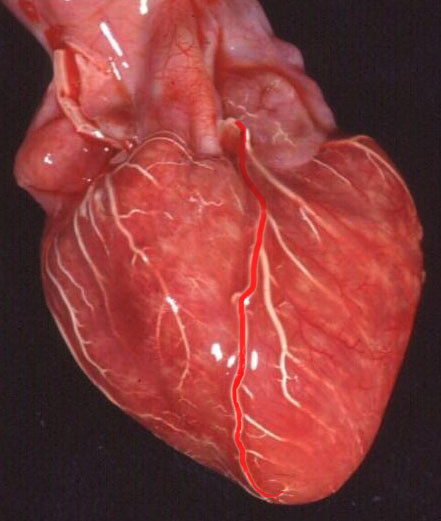
The infrastructure of the heart as a cross has horizontal and vertical components that have 3 dimensions (b). The tricuspid valve and annulus (blue ring) and mitral valve and annulus (red horizontal ring) are aligned in the horizontal plane (c). The right coronary artery (RCA) and circumflex (LCx) supply the right and left side while the left anterior descending (LAD) and posterior descending artery (PDA) align along the the vertical limb.
Ashley Davidoff MD
Horizontal circle consists of the mitral and tricuspid annuli and the Circumflex and RCA run in their respective A-V grooves. The LAD and PDA run anteriorly and posteriorly in their respective interventricular grooves
The Cross in 3 Dimensions
The infrastructure of the heart as a cross has horizontal and vertical components that have 3 dimensions.
The tricuspid valve and annulus (blue ring) and mitral valve and annulus (red horizontal ring) are aligned in the horizontal plane (c). The right coronary artery (RCA) and circumflex (LCx) supply the right and left side while the left anterior descending (LAD) and posterior descending artery (PDA) align along the the vertical limb.
Ashley Davidoff MD
CORONARY CIRCULATION IN 3D – ANATOMICAL SPECIMEN INJECTED WITH BARIUM
Anatomical Specimen injected with Barium
The Left Side Anterior
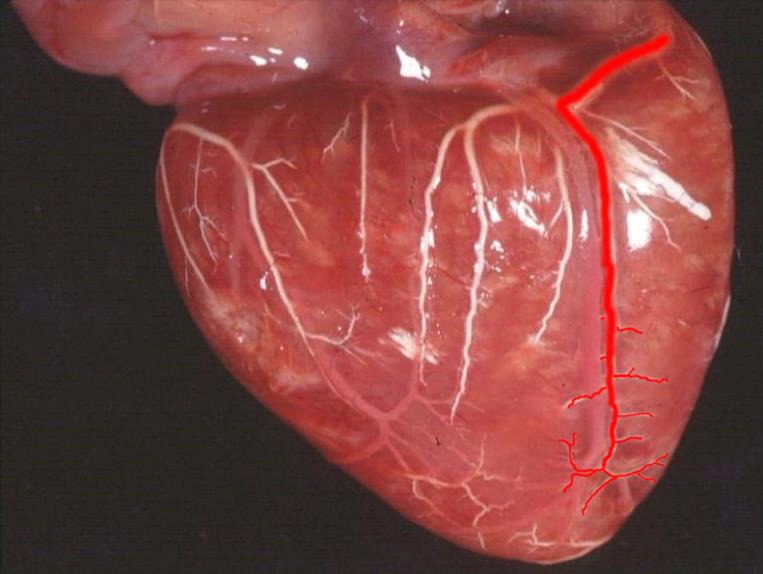
LAD Coursing in the Interventricular Groove
Ashley Davidoff MD
Branches
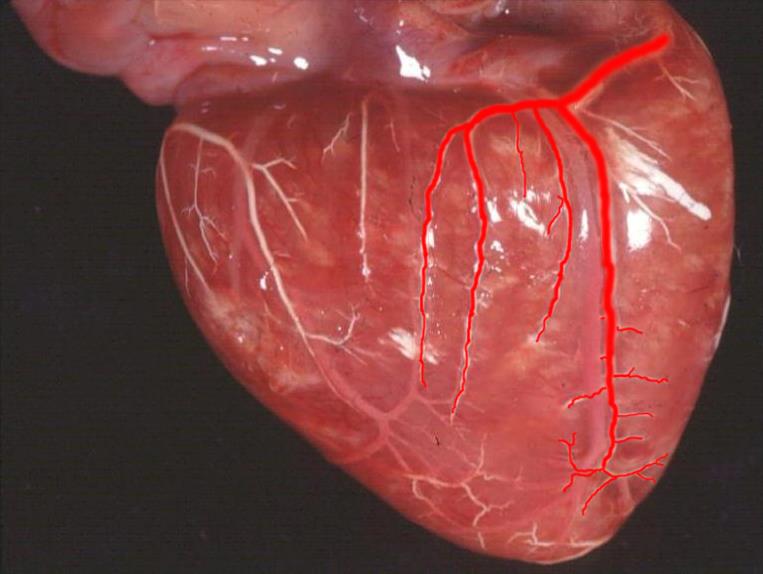
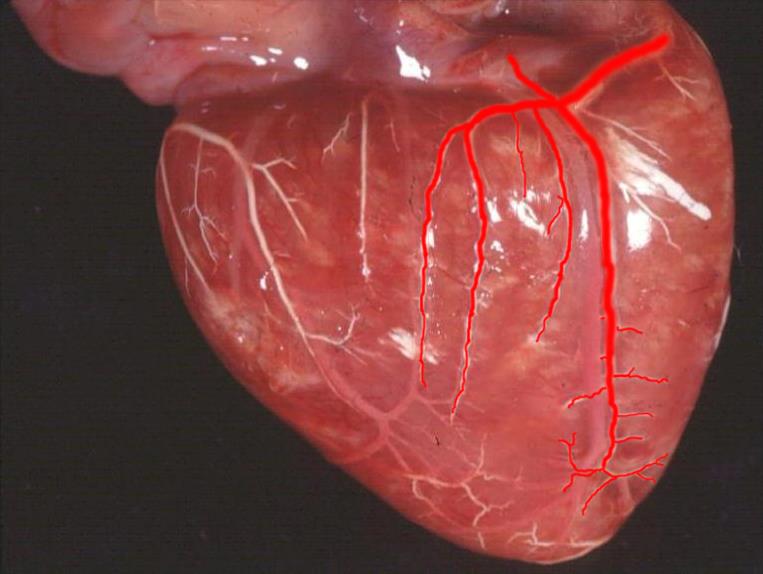
3-5 Diagonals supplying the anterior portion of the LV
Ashley Davidoff MD
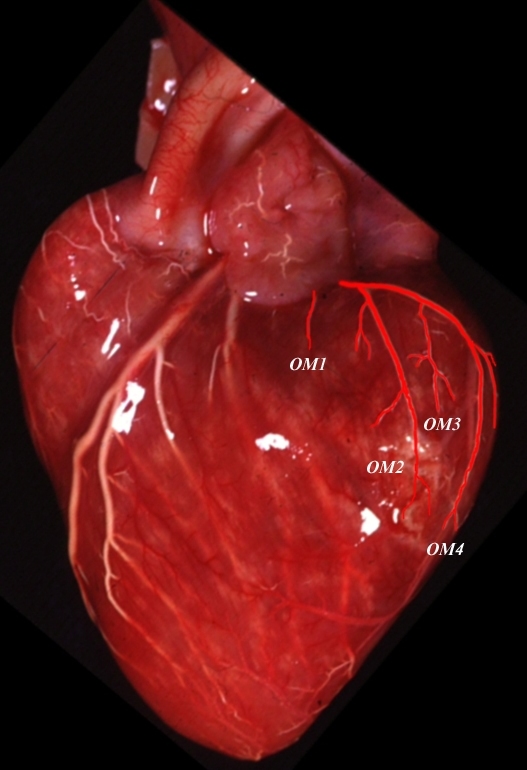
OBTUSE MARGINALS OFF THE CIRCUMFLEX (3-4 vessels)
supplying the lateral and posterior portion of the LV
Ashley Davidoff MD
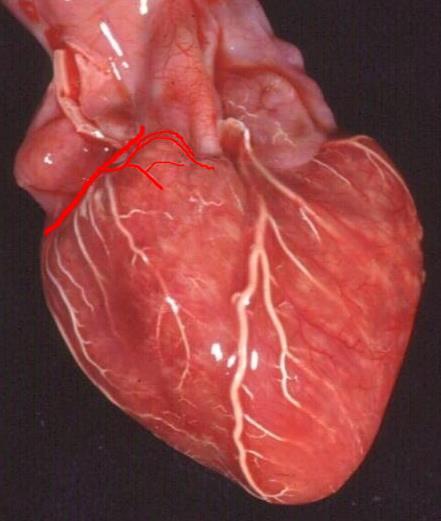
INFUNDIBULAR BRANCH SUPPLYING THE ARC OF VIEUSSENS
Important collateral from proximal LAD to proximal RCA

Ashley Davidoff MD
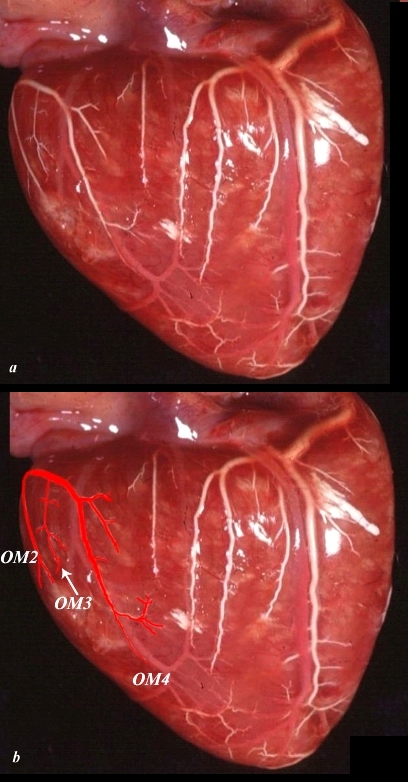
CIRCUMFLEX AND OBTUSE MARGINALS
in lateral projection supplying the lateral and posterior portions of the LV
Ashley DAvidoff MD
OBTUSE MARGINALS OFF THE CIRCUMFLEX POSTERIOR VIEW in a right dominant system. In this case only about 50% of the inferior portion of the LV is supplied by the LCA
Ashley Davidoff MD
RIGHT SIDE – DOMINANT
MAIN RCA IN ANTERIOR A-V GROOVE

Ashley Davidoff MD
INFUNDIBULAR BRANCH SUPPLYING THE ARC OF VIEUSSENS
Ashley Davidoff MD
ANTERIOR RV BRANCHES AND ACUTE MARGINAL ARTERY (arrow)

Ashley Davidoff MD
RIGHT SIDE POSTERIOR VIEW – CONTINUATION OF THE RCA
CONTINUATION OF THE RCA
Ashley Davidoff MD
PDA
Note it runs side by side with the middle cardiac vein
Ashley Davidoff MD
POSTERIOR LV BRANCHES
Ashley Davidoff MD
A-V NODAL ARTERY
Ashley Davidoff MD
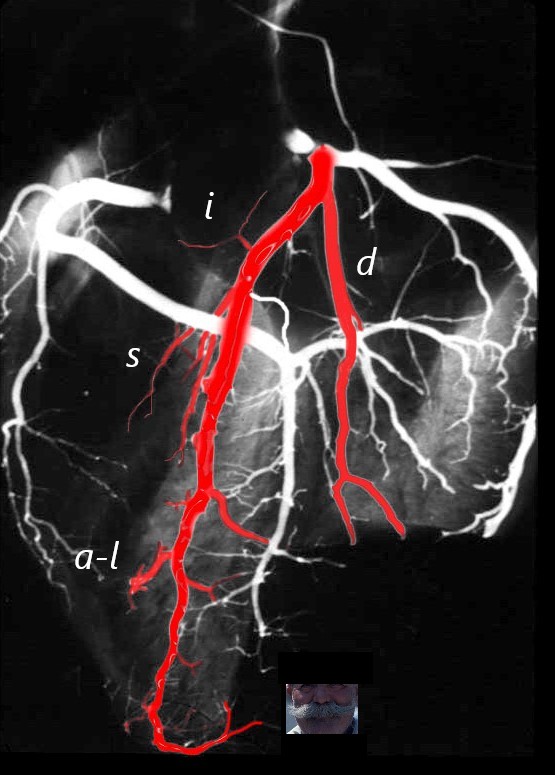
The anatomical specimen has been injected with barium and shows LAD arising from the left main coronary artery. The diagonal arteries (d) course toward the patients left to supply the anterior and anterolateral part of the LV. The infundibular artery (I, aka arc of Vieussen’s) courses over the RVOT to join its partner arising from the RCA. The septal arteries have a vertical course toward the diaphragm, and the branch to the anterolateral papillary muscle of the RV (a-l) courses toward the right of the patient. The LAD often terminates with a bifurcation reminiscent of a moustache.
Ashley Davidoff MD
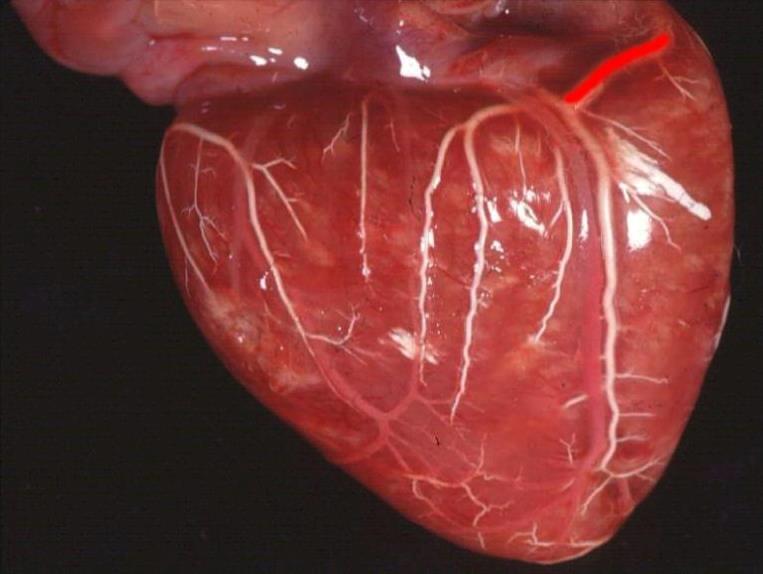
CIRCUMFLEX CORONARY ARTERY –
Note The distal circumflex is usually very small and sometimes not even visible but is recognised by its relationship to the A_V groove and coronary sinus
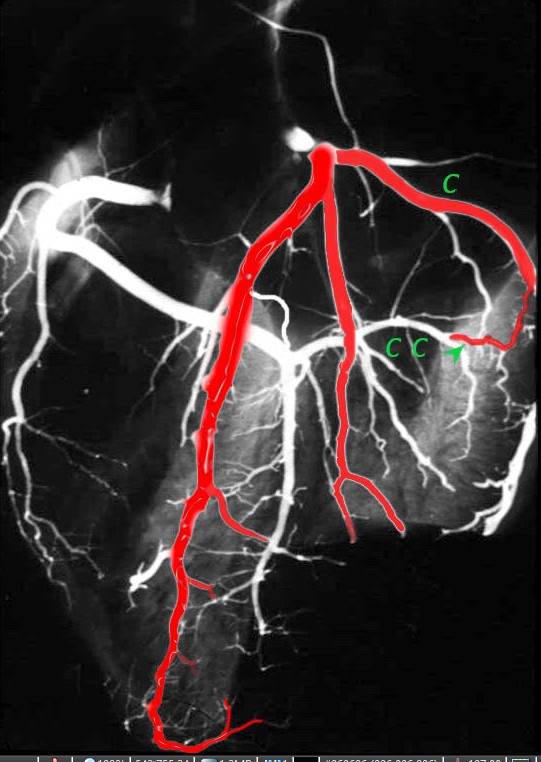
The anatomical specimen has been injected with barium and shows the circumflex (c) arising from the left main coronary artery. The obtuse marginal arteries are large vessels so the distal circumflex continuation (c c green arrow) is a small vessel that runs in the posterior A-V groove with the coronary sinus
Ashley Davidoff MD
BRANCHES OF THE CIRCUMFLEX CORONARY ARTERY
Note the SA nodal artery arises from the circumflex about 40% of the time and from the RCA 60% of the time
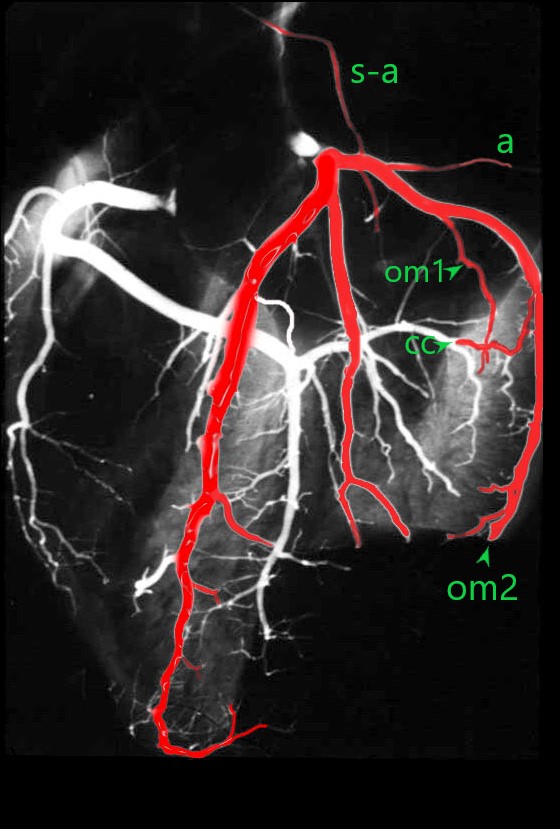
The anatomical specimen has been injected with barium and shows the circumflex (c) arising from the left main coronary artery. The obtuse marginal arteries are large vessels so the distal circumflex continuation (c c green arrow) is a small vessel that runs in the posterior A-V groove with the coronary sinus
The S-A nodal artery (s-a) sometimes arises from the circumflex as the first branch. Atrial branches (a) also arise from the proximal circumflex artery.
A number of obtuse marginal arteries (OM1 and OM2 ) supply the posterior and posterolateral parts of the LV and are almost always larger than the distal circumflex itself (c c).
Ashley Davidoff MD
RCA
Note the septal perforators supply about 1/3 of the septum and are important collateral pathway when the LAD is occluded

The coronary arteries have been injected with barium and shows left (bright red overlay) and right (maroon) coronary circulation The proximal RCA (p) courses anteriorly in the A-V groove arising from the right coronary ostium. The acute marginal (am) courses along the right margin of the heart, and the RCA continues posteriorly (p) to the crux of the heart where it gives off 3 branches. The posterior descending artery (PDA), A-V nodal artery (a-v) and posterior left ventricular artery (plv). The PDA supplies the inferior 1/3 of the interventricular septum with perforating septal arteries (s)
This is a dominant RCA
Ashley Davidoff MD
SELECTIVE ANGIOGRAPHY
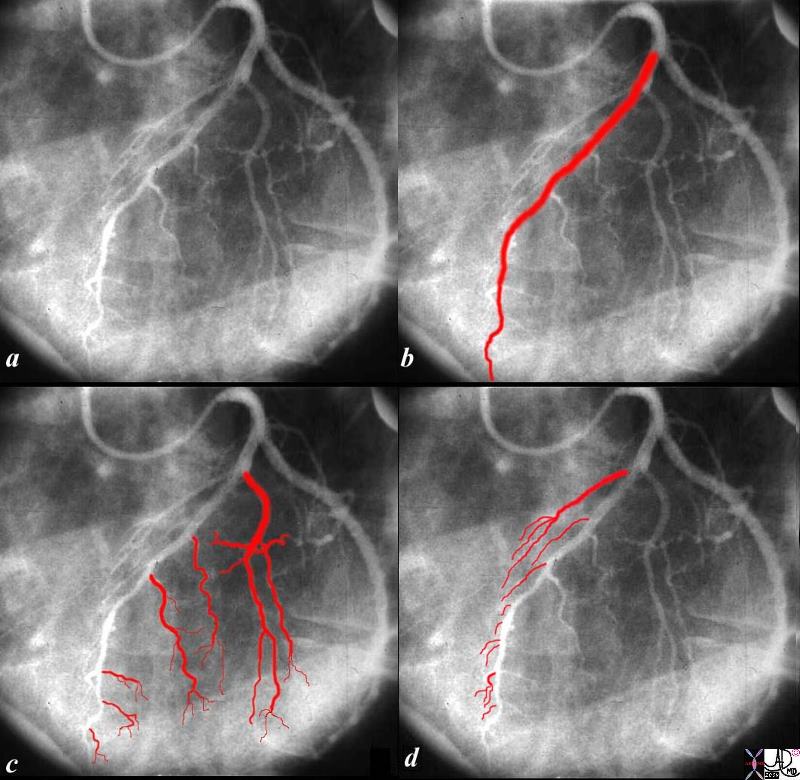
The angiogram of the left coronary artery in the LAO projection shows the LAD in b, diagonals in c and septal arteries coursing toward the diaphragm in d.
Ashley Davidoff MD
Dominant LCA 15-20%
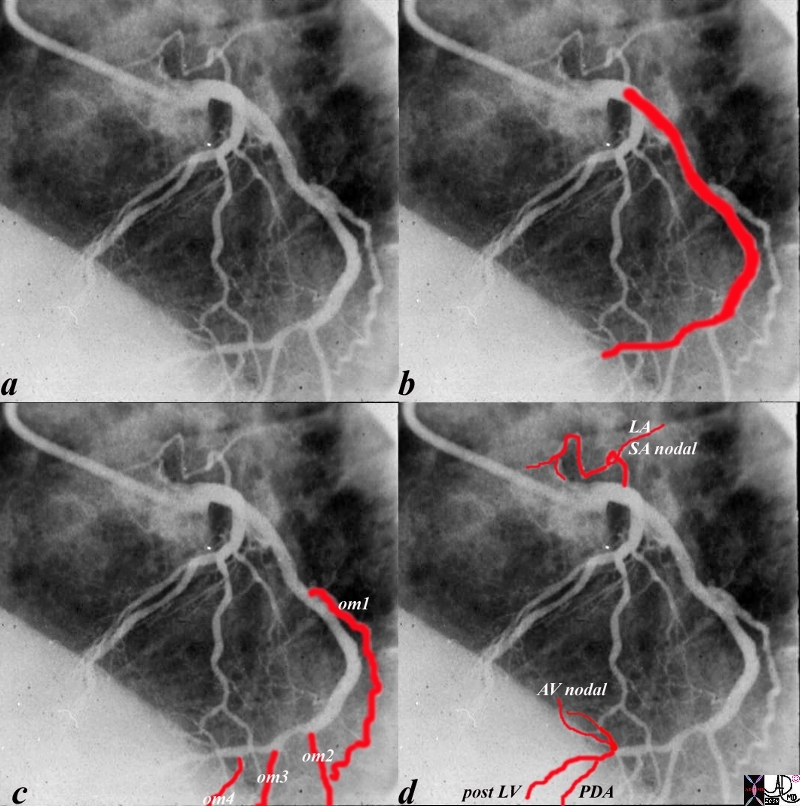
The angiogram of the LCA (a) shows the circumflex (b) arising from the left main coronary artery. In this left dominant system, there are 4 obtuse marginal arteries (c). Distally the circumflex continues and gives rise to the PDA, (d) AV nodal artery and posterior LV branches
Ashley Davidoff MD
RCA Dominant 80-85%
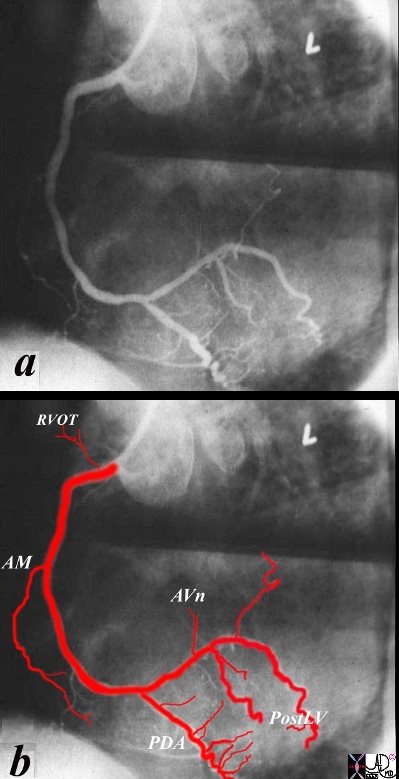
The angiogram of a dominant RCA shows the infundibular artery coursing to the RVOT, the acute marginal artery (AM), at the right margin of the heart, PDA and septal perforators,, A-V nodal (AVn) and posterior left ventricular branches (Post LV)
Ashley Davidoff MD
The coronary arterial tree is divided into three segments; two (the left anterior descending artery and the circumflex artery) arise from a common stem of the left main coronary. The third segment is the right coronary artery. The dominance of the coronary circulation (right versus left) refers to the artery from which the posterior descending artery originates and supplies the Atrio-ventricular node (AV node), and not the absolute mass of myocardium perfused by either. Right dominance occurs in 85% to 90% of normal individuals.
The arteries that supply blood to the heart are the right and left coronary arteries, which extend from the aorta. The right coronary artery originates from the right anterior aortic sinus and extends to the diaphragmatic surface. It is continued to the apex of the heart as the posterior descending branch. The marginal branch of the right coronary artery, which follows the acute margin of the heart, supplies branches to both surfaces of the right ventricle. The marginal branch also supplies oxygenated blood to the right atrium and to the part of the left ventricle. The left coronary artery, which is larger than the right, originates from the left anterior aortic sinus and divides into an anterior descending and a circumflex branch. The anterior descending branch passes behind and then in front of the pulmonary artery and then descends along the left ventricle towards the apex of the heart. The circumflex branch follows the left part of the coronary sulcus, reaching nearly as far as the posterior longitudinal sulcus, and supplying the left atrium and ventricle.

RCA
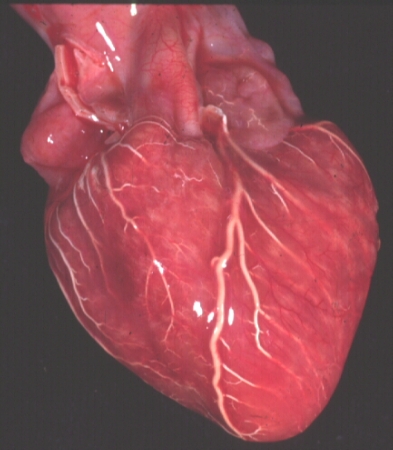
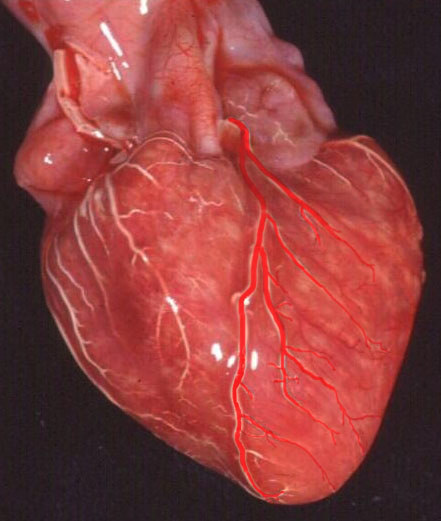
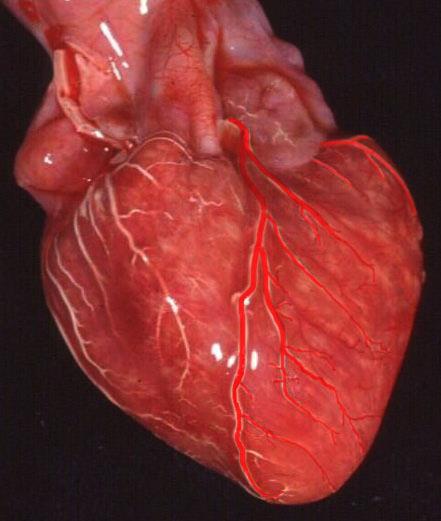
32134 |
| This is an anterior view of the heart showing the long LAD travelling within the expected course of the interventricular septum. Can you identify the LAD? Courtesy of Ashley Davidoff M.D. 32134 code cardiac heart coronary artery LAD diagonal conal infundibulum RVOT anatomy normal |

The Tipped Cross |
| The heart has a left and right arterial system. The vessels are formed around the cross of the heart, “vertically” along the interventricular septum and interatrial septum, and “horizontally” in the atrioventricular (A-V) grooves. The left coronary artery arises from the left coronary ostium and supplies one branch, the left anterior descending artery, that travels anteriorly on the anterior aspect of the interventricular septum, and one branch that travels in the atrioventricular groove(left circumflex). The right coronary artery has a branch that courses along the right atrioventricular groove and usually continues as the posterior descending artery on the posterior aspect of the interventricular groove, and commonly gives rise to the A-V nodal branch at the back of the crux of the heart.
Davidoff art drawing Copyright 2009 all rights reserved 06570corb01.8.8s |
Coronary arteries supply blood to the heart muscle. They are the first arteries to arise from the aorta and include the right and left coronary arteries which arise from the respective aortic sinuses, that lie behind the right and left aortic cusps. The orifice of the left coronary artery is superior and posterior to that of the right coronary artery due to the oblique plane of the aortic valve. These major coronary arteries and their branches normally flow epicardially and terminate at the capillary level which lies in the myocardium.
Left Main Coronary artery(LM): The left main coronary artery after arising from the left aortic sinus courses a short variable distance forward between the pulmonary artery and left auricle and then divides into its two principal branches – the left anterior descending artery and the left circumflex artery. A third branch vessel, the Ramus Intermedius (RI) , an artery that arises from the left main between the LAD and LCX, may be found in 37 % of the population. It supplies the free lateral wall of the left ventricle. The LM varies in length from 1 to 25 mms and has a diameter of 5-10 mm .
Variations in LM anatomy :
In few cases, the LCA may be very short and bifurcates almost immediately.
In 0.41% of the cases, the LCA is not developed and there are two orifices in the left coronary sinus giving origin to the LAD and LCX.
In the majority of cases, the LM divides beneath the left atrial appendage, into the left anterior descending (LAD) and the circumflex arteries(LCX).
Left anterior descending: (coronary artery of Vieussens) The LAD courses in the anterior interventricular groove towards the apex of the heart . a direct continuation of the LM stem from the bifurcation nourishes the anterior and lateral wall of the left ventricle by coursing anteriorly and inferiorly towards the apex.
Course : The LAD a direct continuation of the LM from the bifurcation, adopts a S shaped course by passing to the left of the pulmonary trunk and then running anteriorly and inferiorly in the anterior interventricular groove towards the apex which it wraps around in as many as 80% of the cases to reach the inferior wall. It occasionally continues through the posterior interventricular groove, where it is known as Mouchet’s posterior recurrent interventricular artery. The left anterior descending artery (LAD) has the most constant origin, course and distribution and is usually divided into proximal, middle and distal segments.
Branches of LAD: The LAD gives rise to two main groups of branches. (1) The septal branches, which supply the anterior two-thirds of the septum, and (2) The diagonal branches, which lie on the lateral aspect of the left ventricle. A third set of branches are the right free wall branches.
The septal branches vary in size, number (4 to 6 or more) and distribution and arise from the LAD at a 90 degree angles, which serves as a useful marker for identification of the left anterior descending artery on coronary angiograms . The septal branches of the LAD anastomose with the septal branches of the posterior descending, thereby making the interventricular septum the most densely vascularized portion of the myocardium . The LAD is divided into 3 segments proximal (origin to first septal), middle (first septal to third septal) and distal (third septal to apex) by the septal branches. A fourth segment is that which lies distal to the cardiac apex. The first septal perforator is the largest and usually arises just distal to the take off ,of the first diagonal branch.
The diagonal branches of the LAD arise at an acute angle (run diagonally away from the LAD- towards the left ventricular wall) to it and extend over surface of heart between interventricular and A-V groove. They vary in size and number(2-5) and supply the anterolateral wall of the left ventricle and the anterior left ventricular papillary muscle. Most frequently there is atleast one diagonal branch. Failure to visualize any diagonal artery denotes occlusion.
Supply : The LAD is the largest epicardial coronary artery and supplies 40 – 60% of the left ventricular myocardium . It supplies adjacent areas of the left and right ventricular myocardium while in the anterior AV septum, AV bundle of conducting tissue and most of the LV myocardium including anterior papillary muscle and apex. Right bundle is supplied by the septal perforators of the LAD.
Anomalies of the LAD : A rare anomaly is the early bifurcation of the anterior interventricular artery, which gives rise to two arteries which are defined as long or short anterior interventricular arteries depending on their length. The one too short to reach the apex is the “short LAD” and stays in the anterior interventricular sulcus (AIVS). The other, the “long LAD,” travels to the apex, first along the AIVS, then leaving it, and then reentering the distal AIVS. Must be differentiated from a parallel diagonal.
Left Circumflex coronary artery: Is a smaller branch of the LM compared to LAD and is otherwise called the posterior division of the left coronary artery.
Course : It originates from the LM at a right angle to the LAD and travels a variable distance posteriorly, along the left atrioventricular groove beneath the left atrial appendage and parallel to the coronary sinus vein. In 85–95 percent of patients, it terminates in the coronary groove in the posterior surface of the heart before reaching the crux , however in the remaining 10–15 percent of patients, it continues around the atrioventricular groove to the crux of the heart to give rise to the posterior descending artery(Left dominant system) .
Branches : The principal branches are the anterior and posterior marginal arteries , obtuse marginal arteries and the left atrial branch . The marginal arteries are variable in number but usually three in the absence of the obtuse marginal ,and are the longest branches off of the circumflex artery supplying the lateral wall of the left ventricle. A large branching artery that dominates the lateral left ventricular wall and is composed of anterior and posterior branches that share a common trunk is called the obtuse marginal artery.
Supply : The left circumflex supplies the left atrium and the lateral and posterior walls of the left ventricle. A branch from the LCX supplies the SA node in 45 % of the population and the AV node in 10%.
Anomalies of the left circumflex coronary artery: Anomalous origin of the left circumflex artery from the
right sinus of Valsalva or the RCA is one of the most common congenital coronary anomalies. They can be identified on coronary angiography by the aortic root sign(profile view of the artery behind the aortic root during left ventriculography ) and the sign of non perfused myocardium (absent arterial inflow to a significant area of the posterior lateral left ventricle during selective injections of the main left coronary artery).
Right Coronary Artery: The right coronary artery (RCA) originates from the right coronary sinus of Valsalva at a slightly lower level than the origin of the left main coronary artery.
Course : It courses anteriorly between the right auricle and the pulmonary trunk to reach the atrioventricular sulcus. It then passes beneath the right atrial appendage within the right atrioventricular groove continuing around the margin of the heart towards the crux. In 85–90 percent of the population, the right coronary artery crosses the crux, and terminates as several parallel trunks descending in or near the posterior interventricular sulcus towards the terminal branches of the left anterior descending artery at the apex.
Right coronary artery segments : Proximal R1(Extends from the ostium of the right coronary artery to the first of the longest acute marginal branches) , Middle R2(Extends from the origin of the first acute marginal branch to the origin of the third acute marginal branch) and distal R3 (Extends from the origin of the third acute marginal branch to the origin of the posterior descending artery). Right posterolateral artery forms R4 and represents the distal continuation of the right coronary artery after the origin of the posterior descending artery.
Branches :
The first branch of the RCA is the conus branch or infundibular branch which in as many as 50 % of individuals may take off from a separate ostiumin the right sinus and supply the right ventricular infundibulum. An anatomic connection between the right and left coronary arterial systems via the conus branch of the right coronary system and one or more vessels of the LAD that cross the anterior right ventricular outflow tract exists and provides collateral circulation. This has been called the Vieussen’s ring after Raymond de Vieussens who described it.
The sinus node artery arises as the second branch in 60 % of the individuals , with a dual blood supply from the LCX and RCA in 2- 7 %. In another 45 % the SA node is supplied by the LCX.
The vertical portion of the RCA gives origin at the acute margin of the heart to the longest 3 arteries arising from the right coronary artery to supply the free anterior right ventricular wall called the acute marginal artery (A1,A2,A3).
In the right dominant circulation the RCA terminates by bifurcating into the posterior descending and right posterior lateral segment artery .
The posterior descending artery travels in the posterior interventricular septum towards the apex where it anastomoses with the LAD. During it course in the interventricular septum it gives rise to septal branches at a vertical offshoot which helps in its identification during angiography.
The right posterior lateral segmental artery proceeds as a continuation of the RCA and ends by anastomosing with the LCX. It gives rise to the right posterior and right inferior arteries in large right-dominant anatomy, to just the right inferior branch in small right-dominant anatomy, and it is not present in left-dominant or balanced dominant systems. It has a characteristic inverted U-shape – TheU turn of James , which helps in its identification on coronary angiography. The atrioventricular nodal branch originates from this artery.
Right inferior artery (RI): Arises from the fourth segment of the right coronary artery and supplies the inferior wall.
Right posterior artery (RP): Distal most branch to arise from the right coronary artery , in a large right dominant circulation. It supplies the inferior wall of the heart .
RCA supply territory :
RCA supplies the SA node, AV node , right atrium , free anterior wall of the RV, posterior part of the interventricular septum, inferior wall of the LV and RV, and apex.
Anomalies of the RCA : The major variation seen in the RCA circulation is the length of the RCA resulting in a short non dominant , large right dominant or small right dominant circulation.
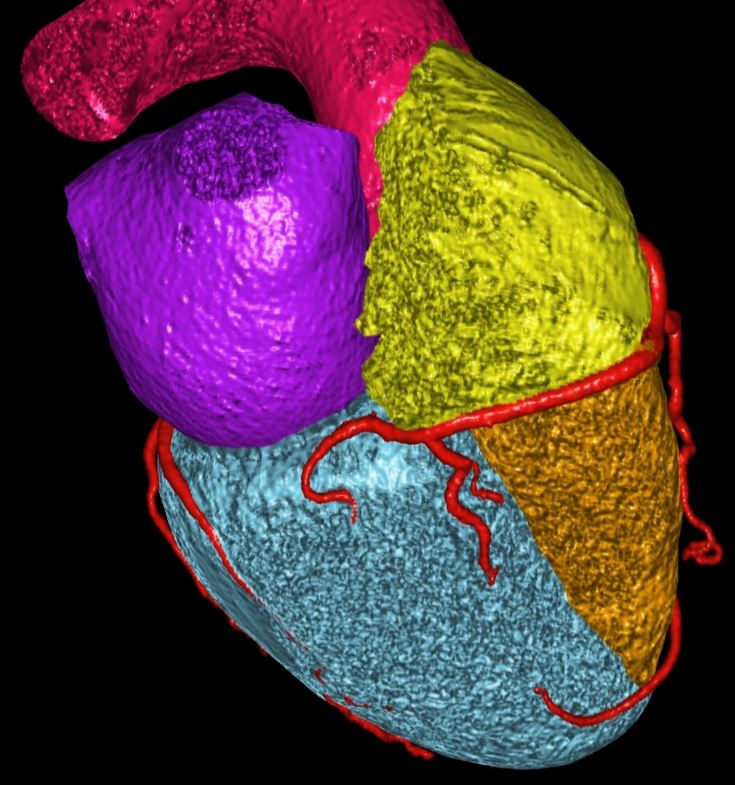
CTA of the Coronary Arteries
LAD
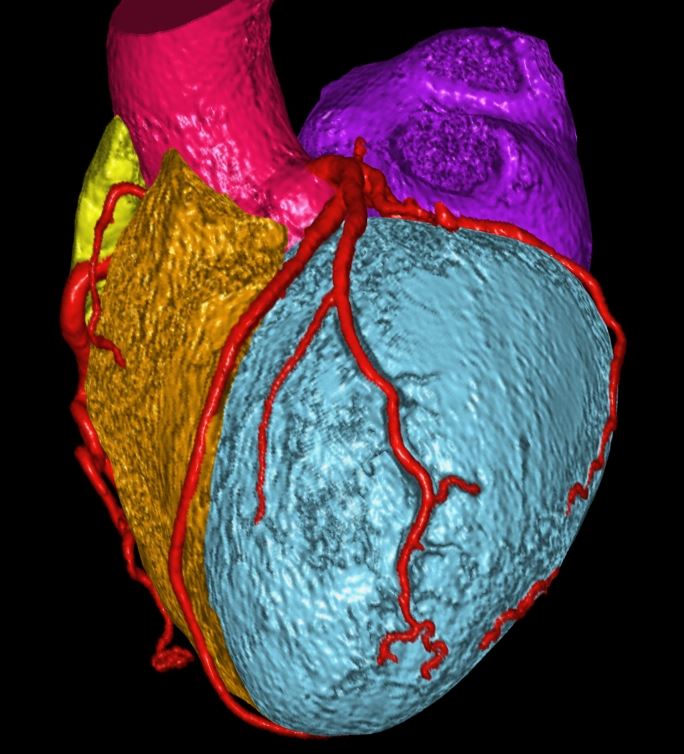
Circumflex
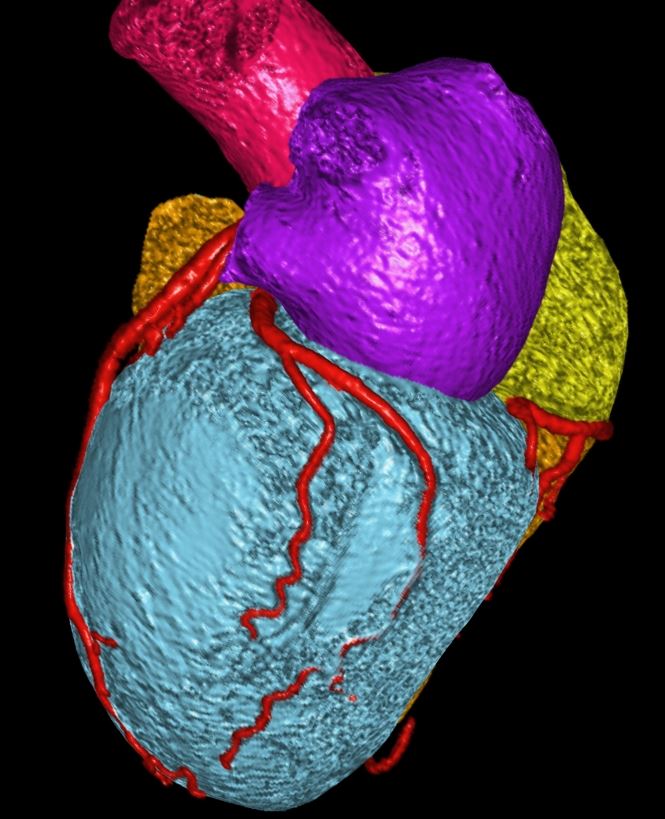
RCA
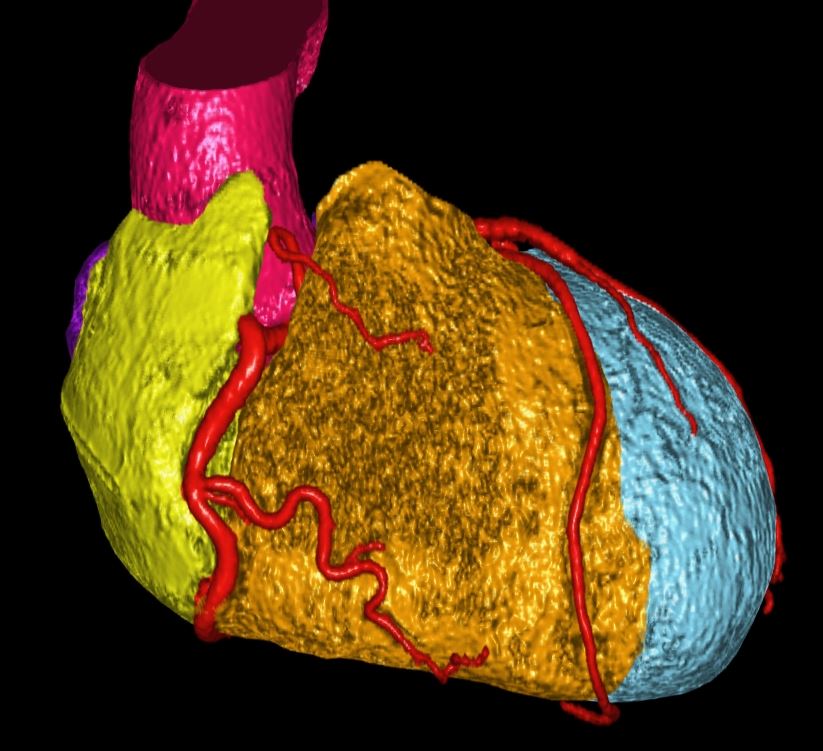
RCA
References
Peter Lanzer, Eric J. Topol Pan vascular medicine: integrated clinical management
Page HL, Enjel HJ, Campbell WB, Thomas CS. Anomalous Origin of the Left Circumflex Coronary Artery Recognition, Angiographic Demonstration and Clinical Significance . Circulation. 1974;50:768.