
- 40 y.o.fe male with PMHx of GERD, mixed hyperlipidemia (hypercholesterolemia and hypertriglyceridemia) and typical chest pain and positive family hx of CAD (father and brother) who comes for a first cardiology clinic visit.
- nuclear stress test
- showed a a small sized,
mild intensity, reversible perfusion defect in the mid to apical inferior wall - symptoms are concerning for stable angina
- optimize medications a
- close follow up in clinic to assess improvement or worsening in symptoms.#Stable angina w/ typical chest pain and abnormal NM stress test w/ reversible ischemia
#Mixed hyperlipidemia (hypercholesterolemia and hypertriglyceridemia) – TGL 799 and LDL 133 on 5/2021
– Continue ASA 81 mg daily
-increased atorvastatin to 80 mg daily on 11/23 (from 40 mg daily)
-started imdur 30 mg daily on 11/23
-increased metop XL to 37.5 mg daily on 11/23 from 25 mg daily
-c/w nitroglycerin SL PRN >> instructed to come to the ED in case increase in nitroglycerin use and refractory chest pain after 3 doses
-ordered fu w/ Cardiology NP in 2wks to assess symptoms and in case of no improvement will place a referral for a cardiac catheterization for further ischemic evaluation
- close follow up in clinic to assess improvement or worsening in symptoms.#Stable angina w/ typical chest pain and abnormal NM stress test w/ reversible ischemia
- showed a a small sized,
- Cardiac Cath
- Coronary fistula from conus to (likely) pulmonary artery
Hemodynamics – LVEDP Normal - Normal coronary arteries

Conal artery to PA fistula
Ashley DAvidoff
TheCommonVein.net
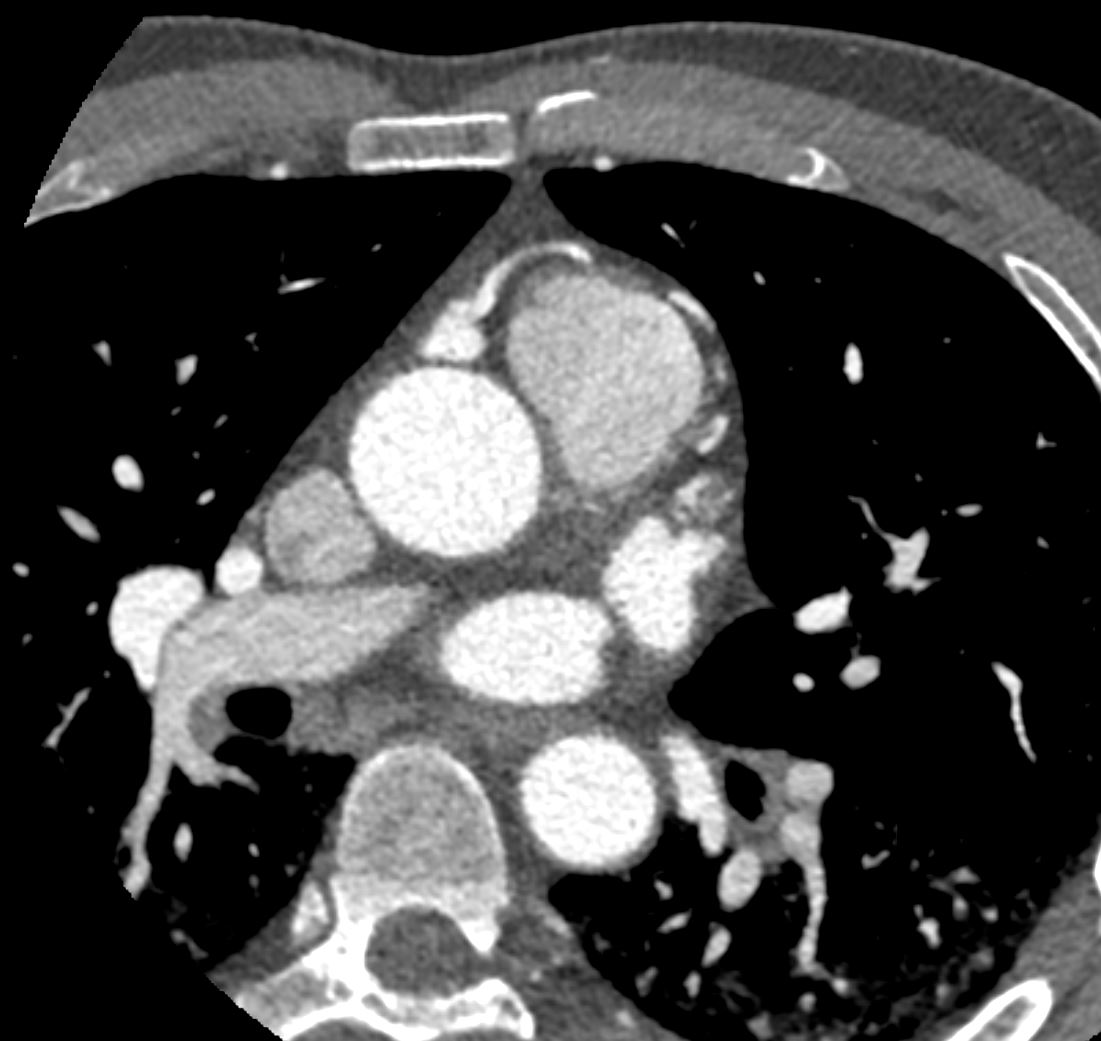
CTA coronaries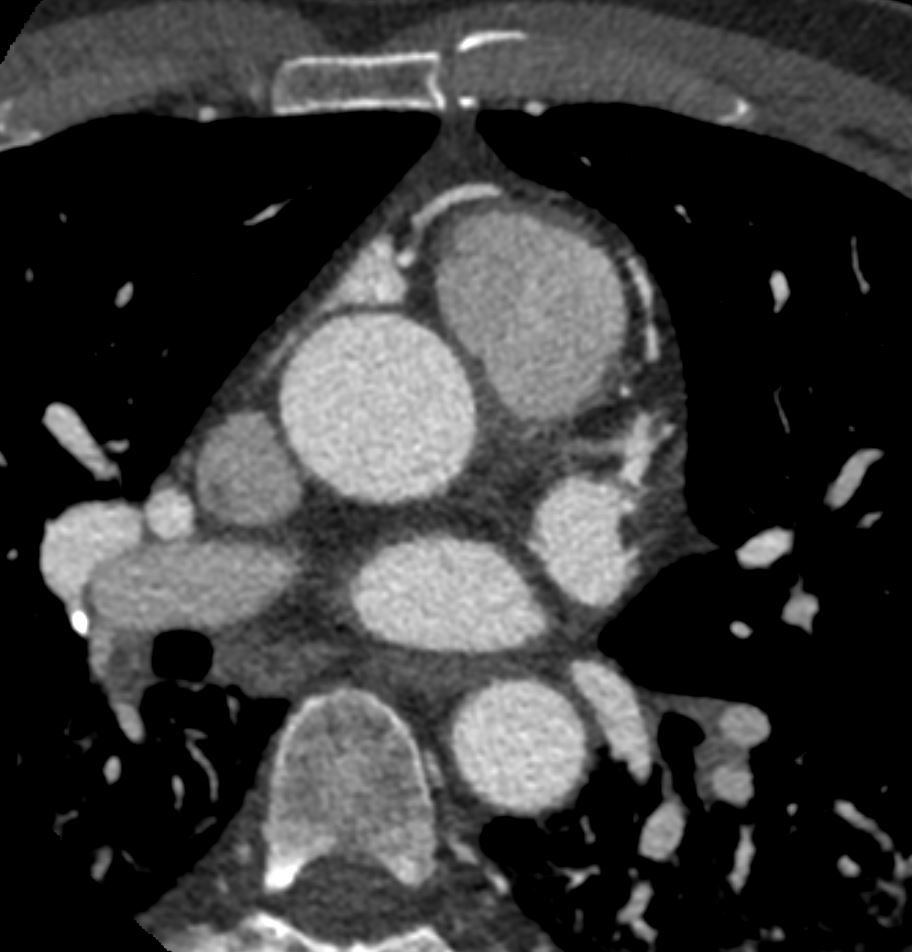

Conal artery to PA fistula
Ashley DAvidoff
TheCommonVein.net
CTA coronaries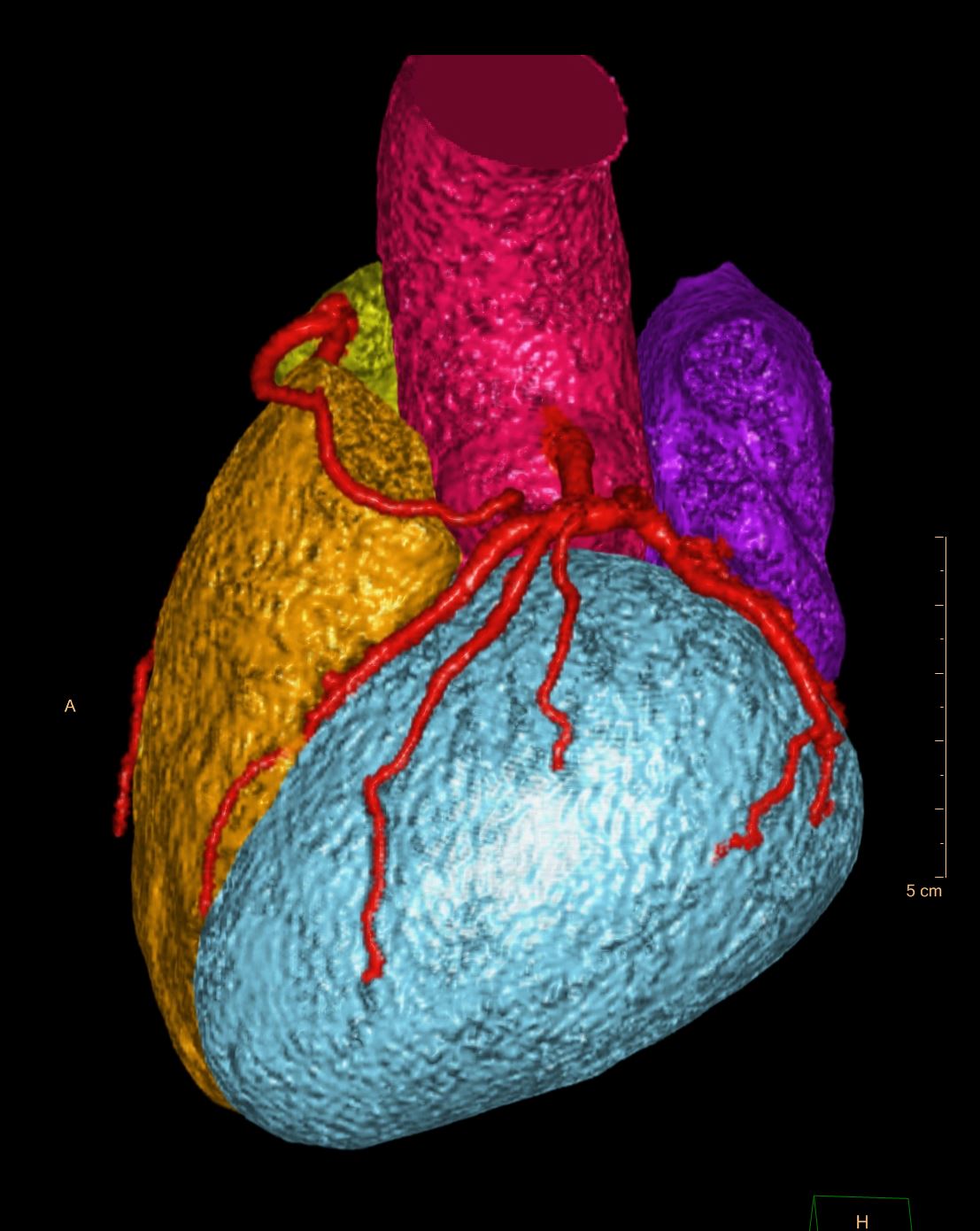
Conal artery to PA fistula
Ashley DAvidoff
TheCommonVein.net
CTA coronaries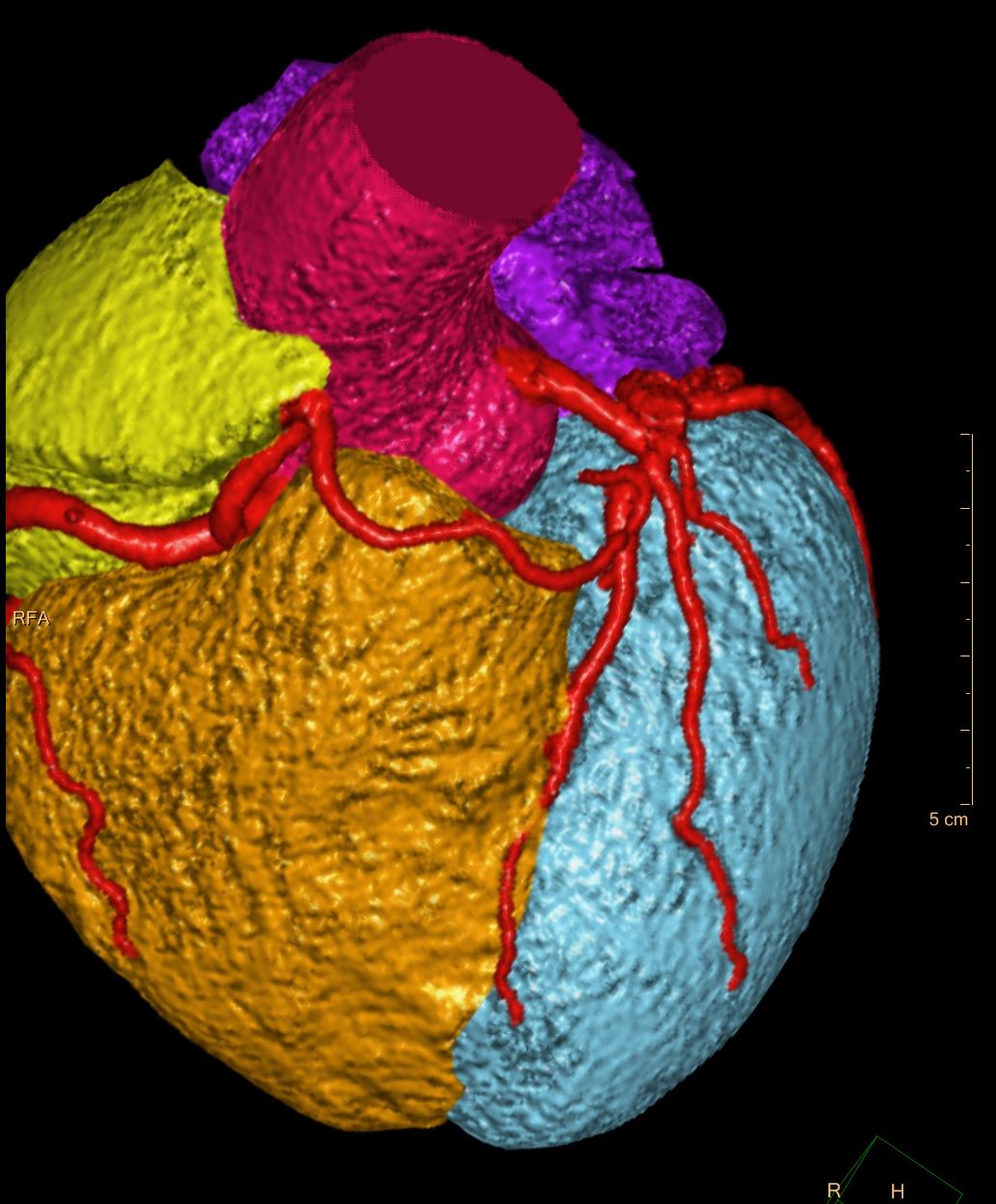
Conal artery to PA fistula
Ashley DAvidoff
TheCommonVein.net
CTA coronaries
Conal artery to PA fistula
Ashley DAvidoff
TheCommonVein.net
CTA coronaries
- Coronary fistula from conus to (likely) pulmonary artery
- CTA
- CTA of the coronary arteries confirms the presence of a large conal artery, predominantly on the right side of the artery with a suggestion of subtle increase in density overlying the left side of the main pulmonary artery and possibly a tangle of vessels in this region verifying the findings on the coronary angiogram. The distal left conal artery could not be optimally visualized but appears to be in close contact with the
proximal LAD and left main, and likely arises from one of these vessels.No evidence of atherosclerosis nor calcifications in the coronary arteriesNormal sized cardiac chambers and no evidence of pulmonary hypertension
- CTA of the coronary arteries confirms the presence of a large conal artery, predominantly on the right side of the artery with a suggestion of subtle increase in density overlying the left side of the main pulmonary artery and possibly a tangle of vessels in this region verifying the findings on the coronary angiogram. The distal left conal artery could not be optimally visualized but appears to be in close contact with the
Links and References
Lim WH et al Journal of CV US
DB126