
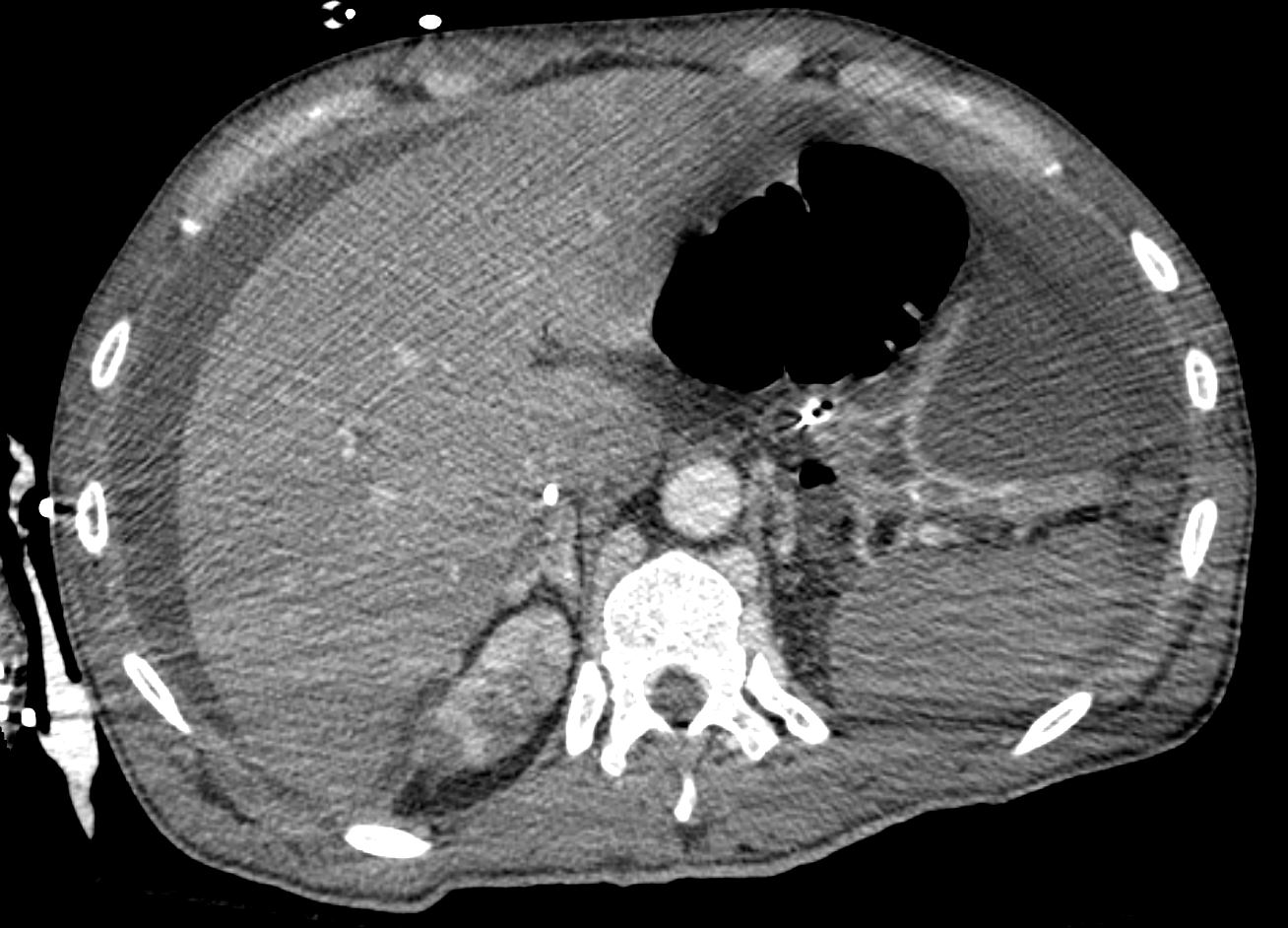
62-year-old man who was brought obtunded to the emergency room. Workup shows him to be acidotic, hypotensive, hypothermic and in septic shock. A CT scan shows a large
amount of fluid and free air.
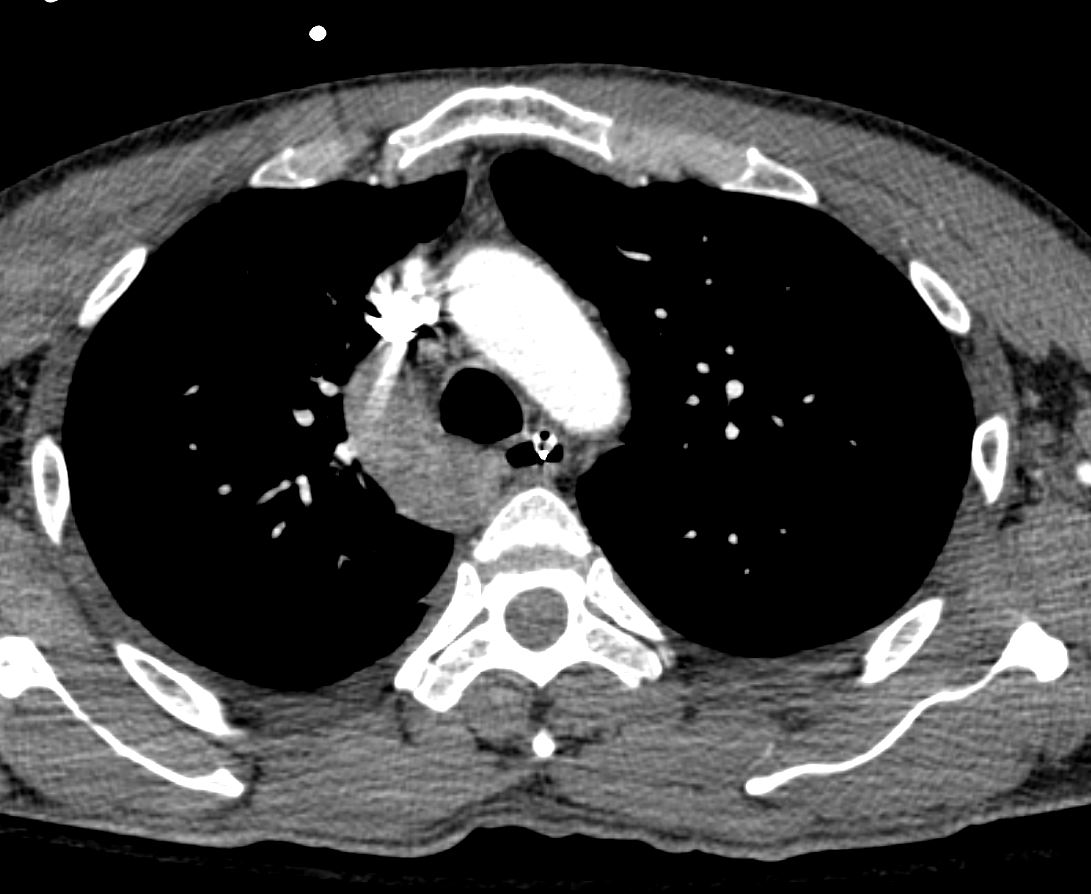
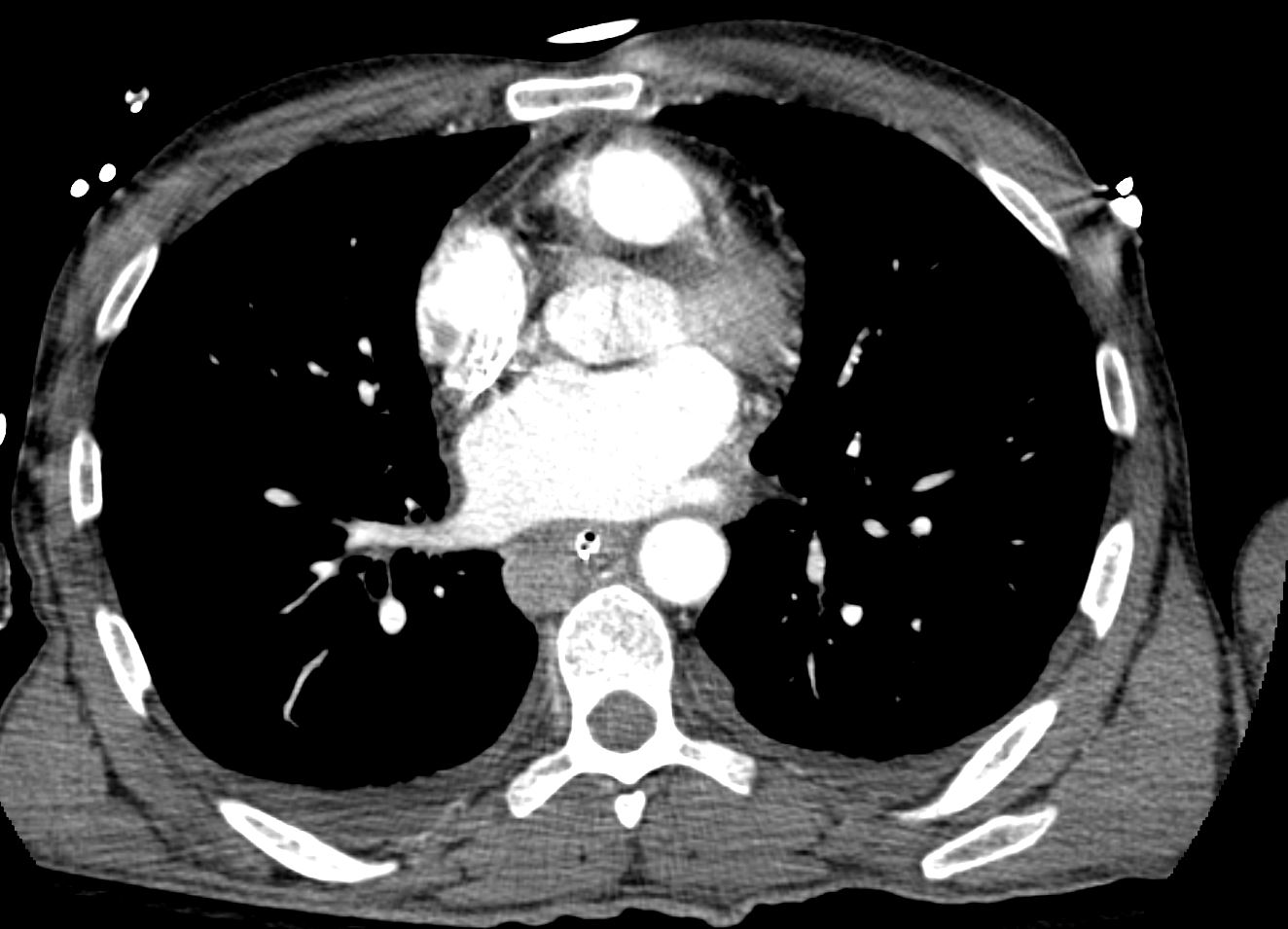
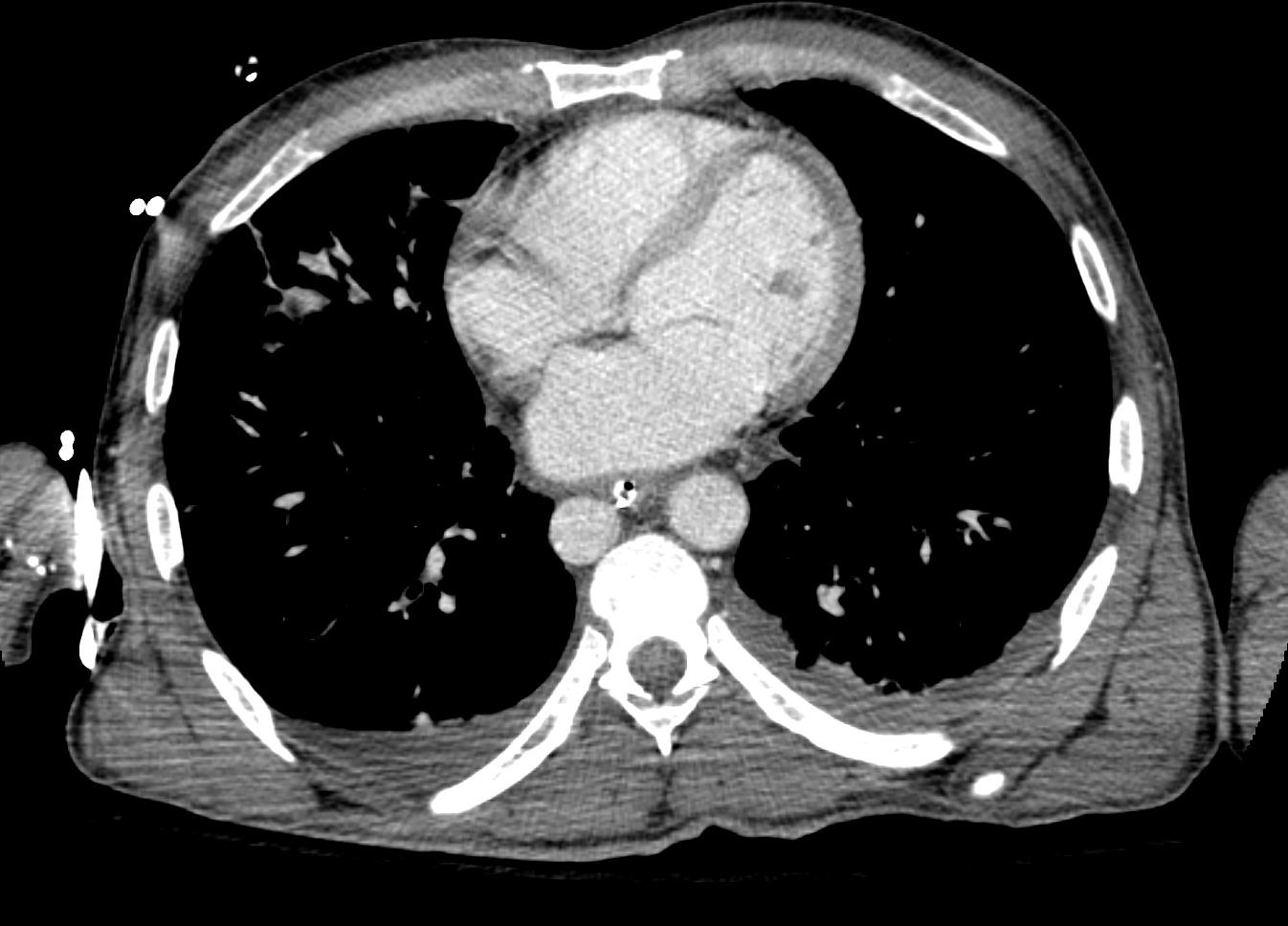
CT scan
Note distended azygous and transverse colon

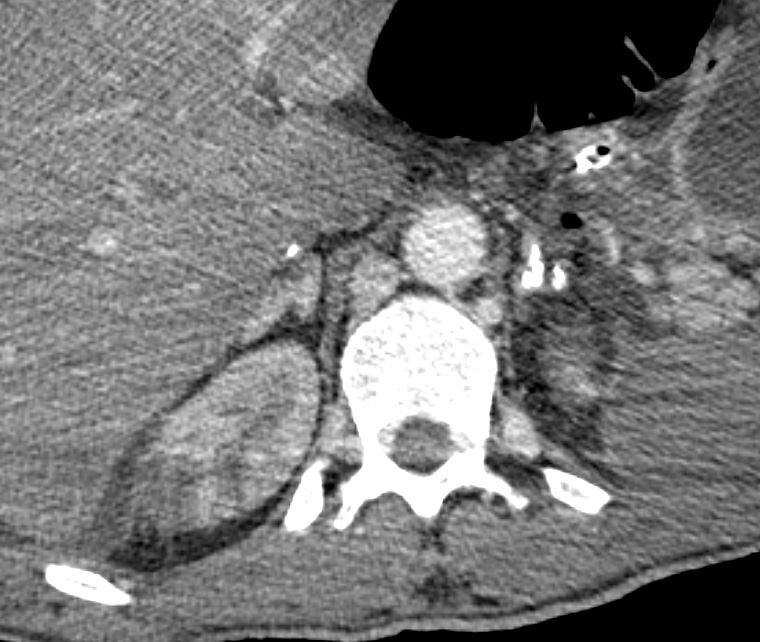
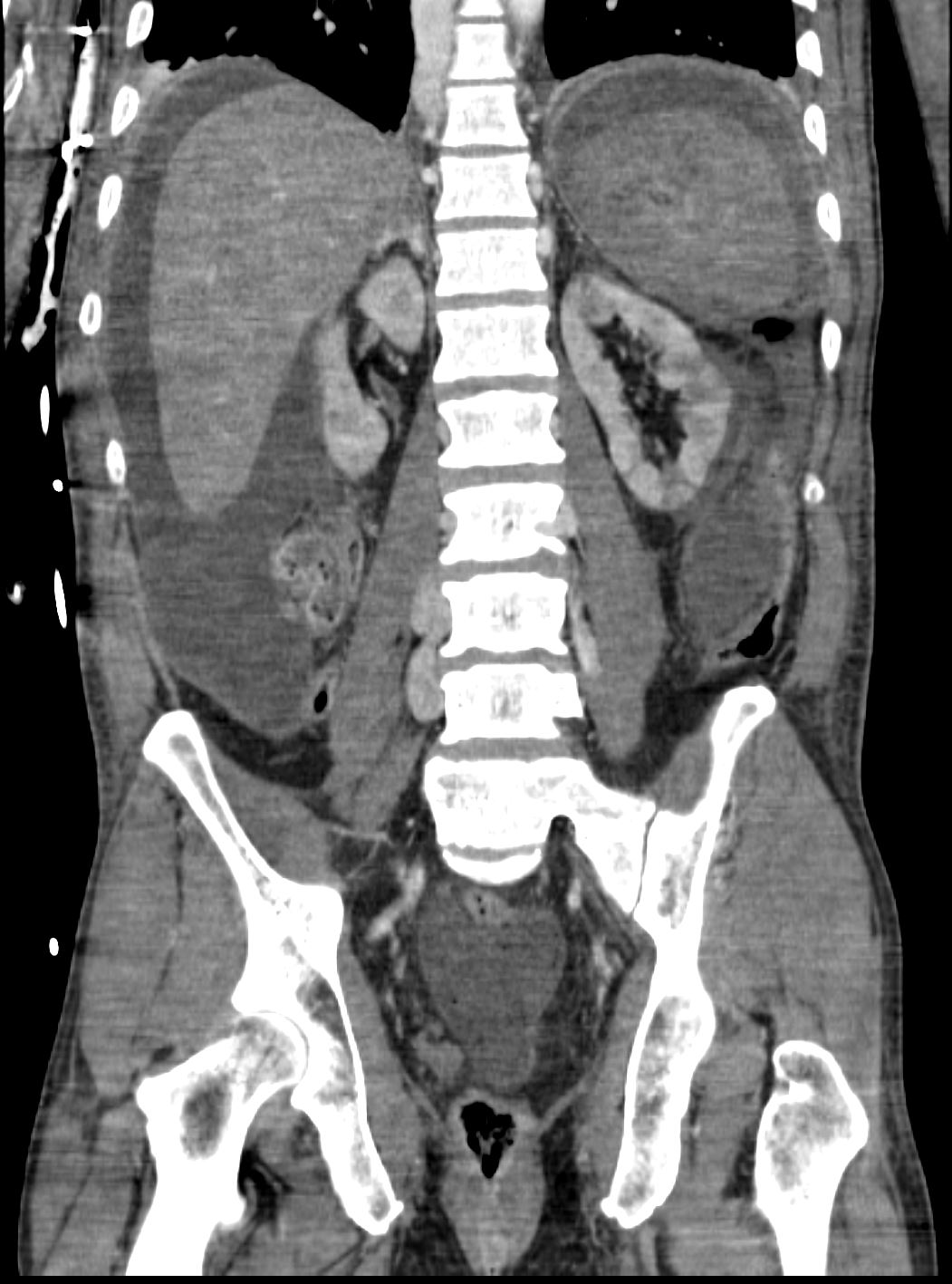
Cortical flow in the adrenal gland

Azygous Extension
Calcified infrahepatic IVC and heteroneous renal perfusion likely secondary to hypotension

Heteroneous renal perfusion likely secondary to hypotension and free air

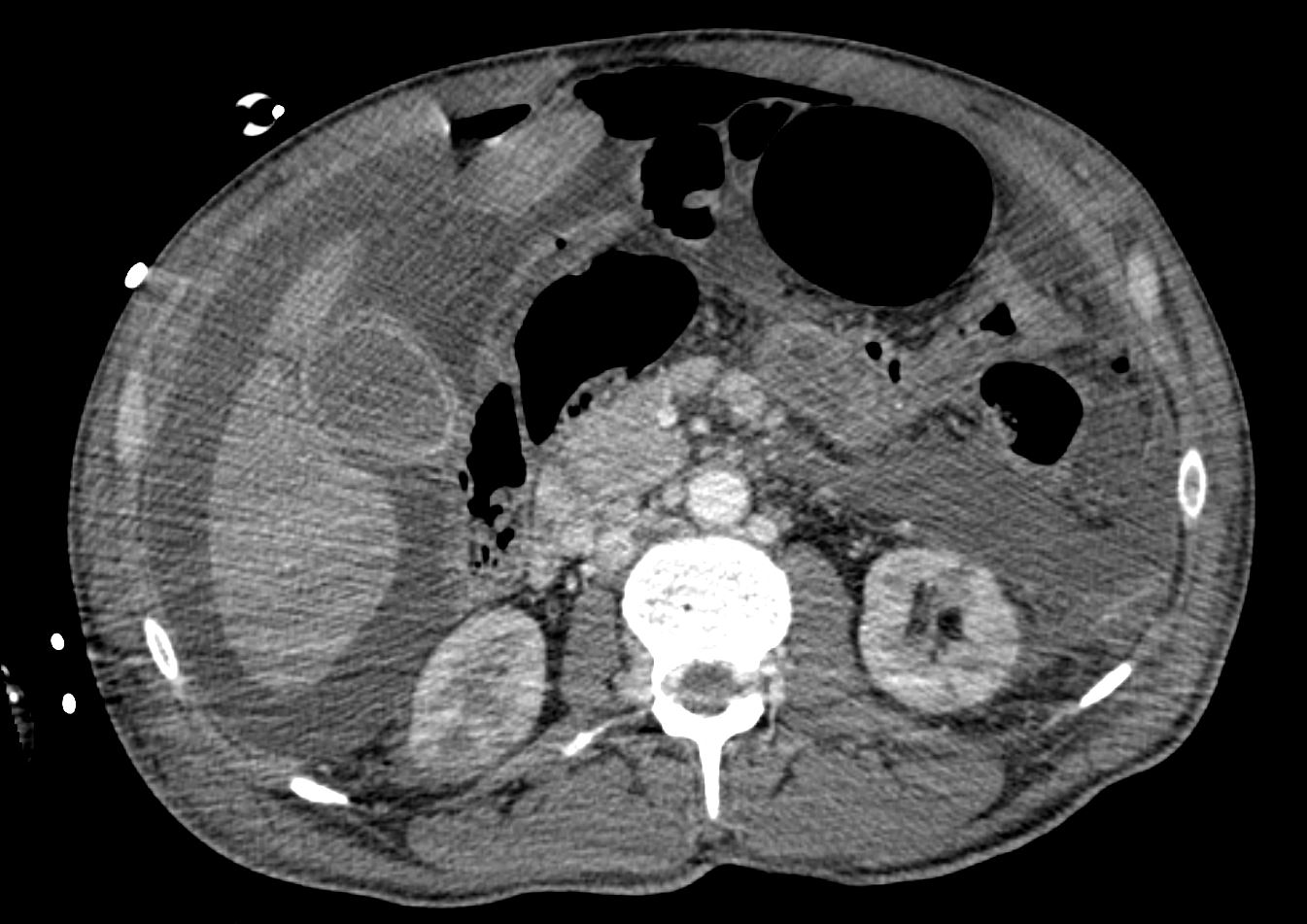
Thick walled hyperemic small bowel


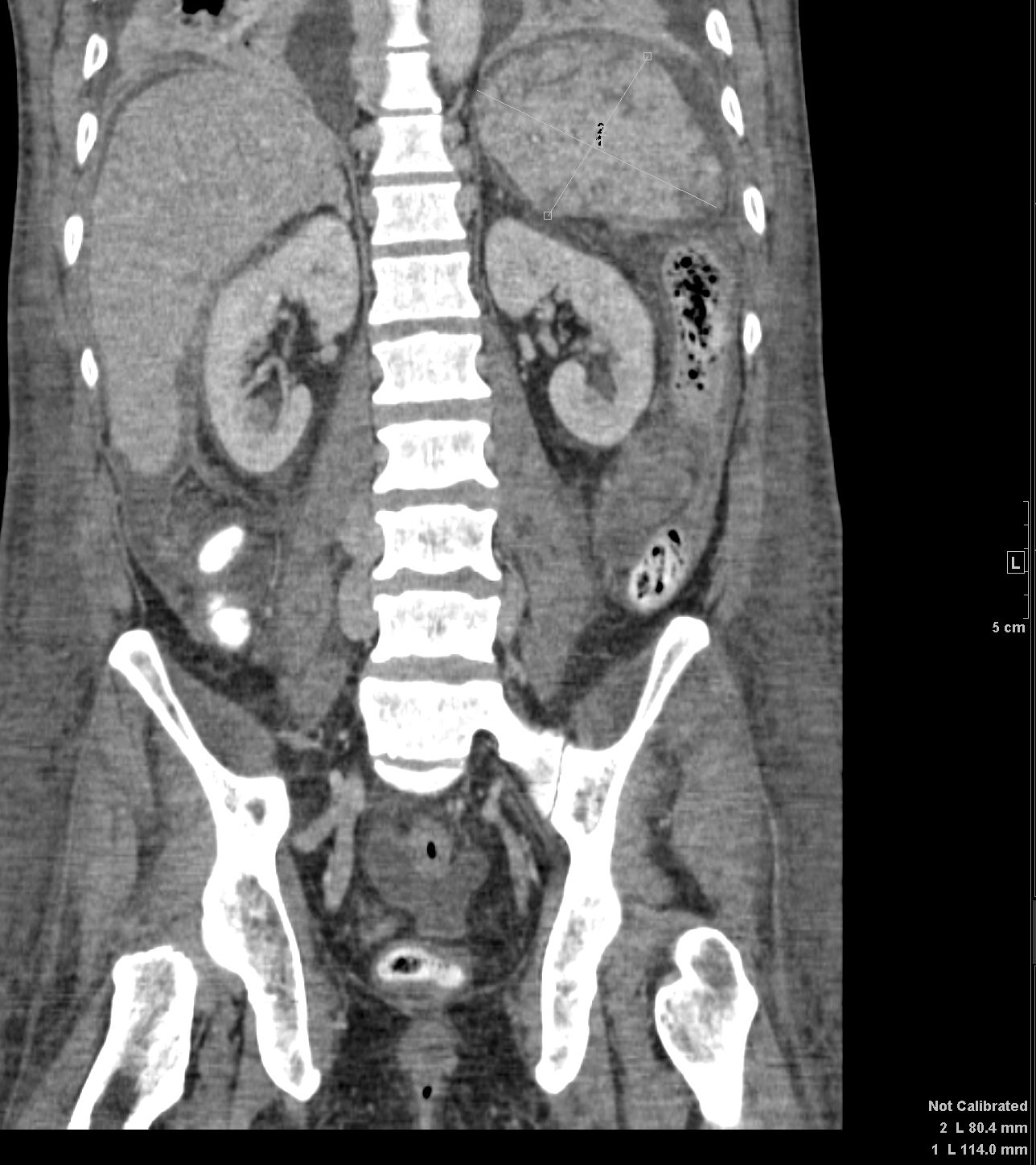
Heterogeneous flow to kidneys
Max dimension of the spleen was -9.9-x 7.3cms

Max dimension of the spleen was -11.4 x 8
1. Free intraperitoneal air with multiple foci of air adjacent to the
greater curvature of the stomach concerning for perforation.
2. Likely bilateral adrenal hemorrhage with hyperenhancing small
bowell suggestive of shock bowel.
3. Multiple hypodensities in the kidneys bilaterally given other
findings likely represents infarcts, pyelonephritis is in the
differential.
The patient was taken emergently to the operating room where he
underwent exploratory laparotomy. Upon entry into the abdomen he had a large amount of purulent, foul-smelling fluid consistent with a perforated viscus This represented well established perforation certainly greater than 24 hours. Exploration of the abdomen first did not reveal an obvious source. On further exploration it appeared that it was coming from the
stomach. The duodenum and pylorus appeared intact. The succus coming from behind the stomach and further mobilization revealed that the perforation was along the lesser curve in the prepyloric area but posterior and high inthe antrum