
35 year old male, PMH including HTN, DM, OSA and obesity who presents to the ED with leg edema. Patient has noted some SOB and for about a month and leg edema
- tachy at 106,
- BNP elevated to 398 but
- trop negative.
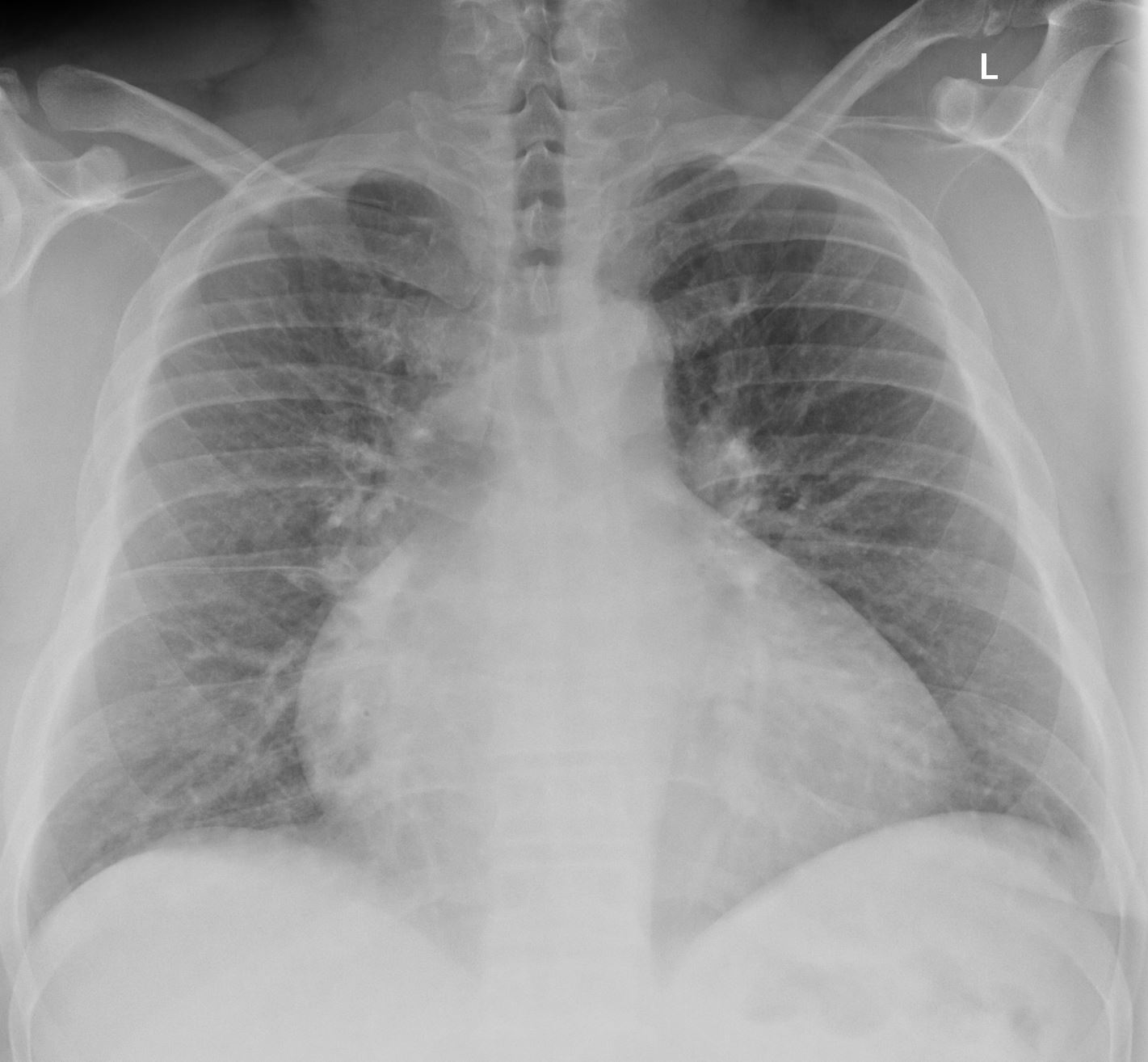
- CXR with some congestion in the hila.
-
Congestive Cardiomyopathy
CXR with mild CHF and global cardiomegaly
Ashley Davidoff
thecommonvein.net - Pt was given 20mg IV Lasix
- active smoker.
- formerly a heavy drinker
- CXR: 1. Moderate cardiomegaly with congested hila.
- TTE: EF 25% with severe global hypokinesis and grade 3 diastolic dysfunction
- Right heart cath
- RHC
- elevated filling pressures with
- wedge of 30 mmHg and
- RA 10 mmHg
- elevated filling pressures with
- RHC
- Coronary Cath
- INDICATIONS:
Congestive Heart FailureCORONARY CIRCULATION:
Left Dominant
Left Main: Normal
LAD:
Left Anterior Descending: Normal
LCX:
Left Circ: Normal
RCA:
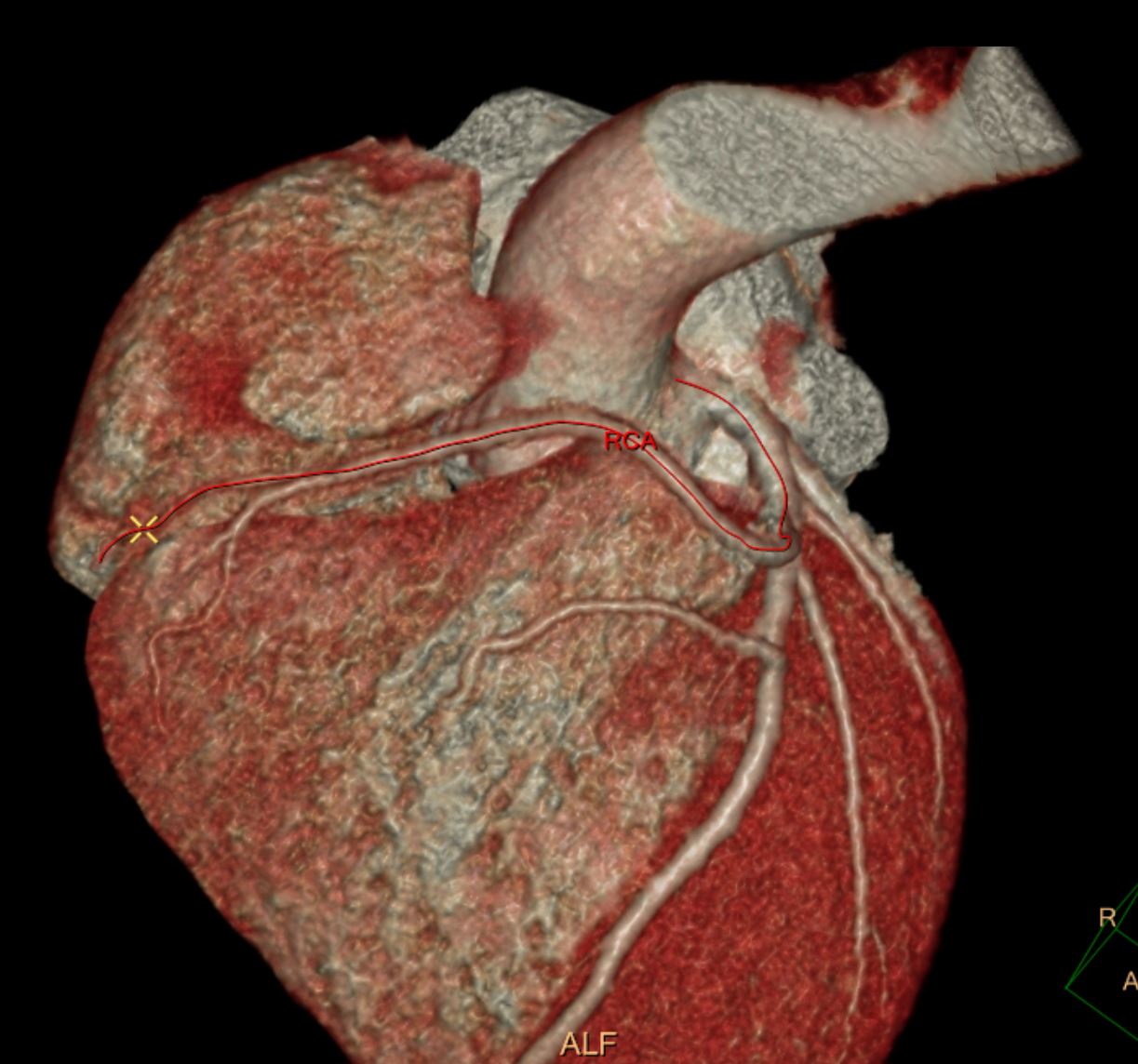
RCA: Anomalous origin from proximal LAD, normal, non-dominant - Coronary CT today to evaluate course of anomalous RCA showed
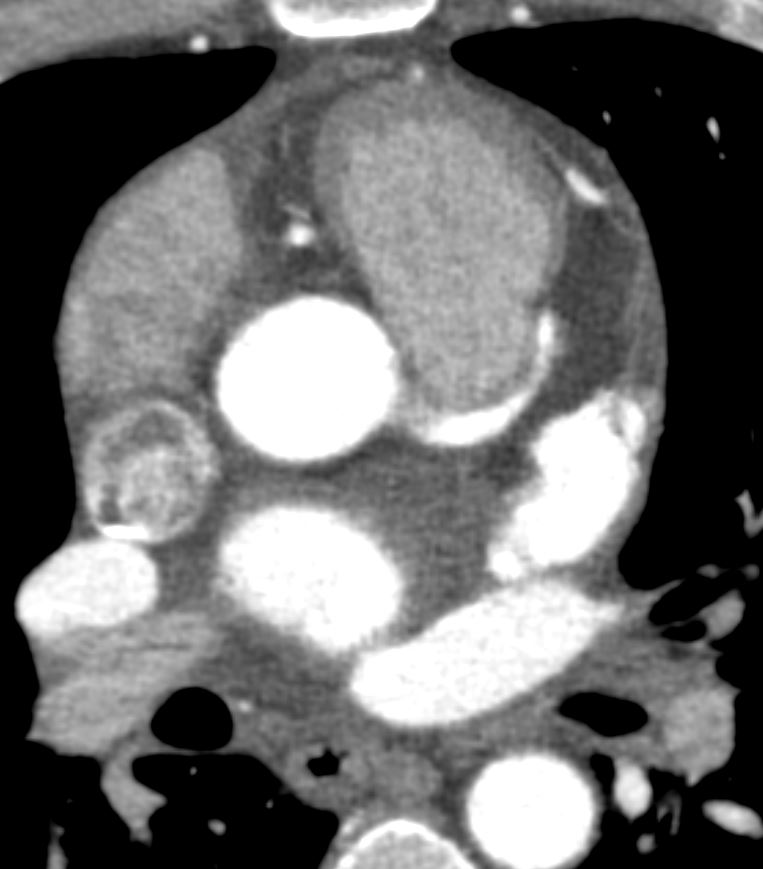
- anomalous right coronary artery with prepulmonic course,
- severe globally depressed biventricular function, and
- no significant coronary artery plaque or stenosis.

Anomalous origin of the RCA from the proximal LA – non dominant right CA
Ashley Davidoff
thecommonvein.net
Anomalous origin of the RCA from the proximal LA – non dominant right CA
Ashley Davidoff
thecommonvein.net
Anomalous origin of the RCA from the proximal LA – non dominant right CA
Ashley Davidoff
thecommonvein.net