
- 32 year old female
- dyspnea since a child
- hx of Swyer James syndrome
- absent perfusion to her RUL
- 20 years ago diagnosed with PAH on cardiac catheterization.
- Rx oral therapies which a
- controlled her symptoms.
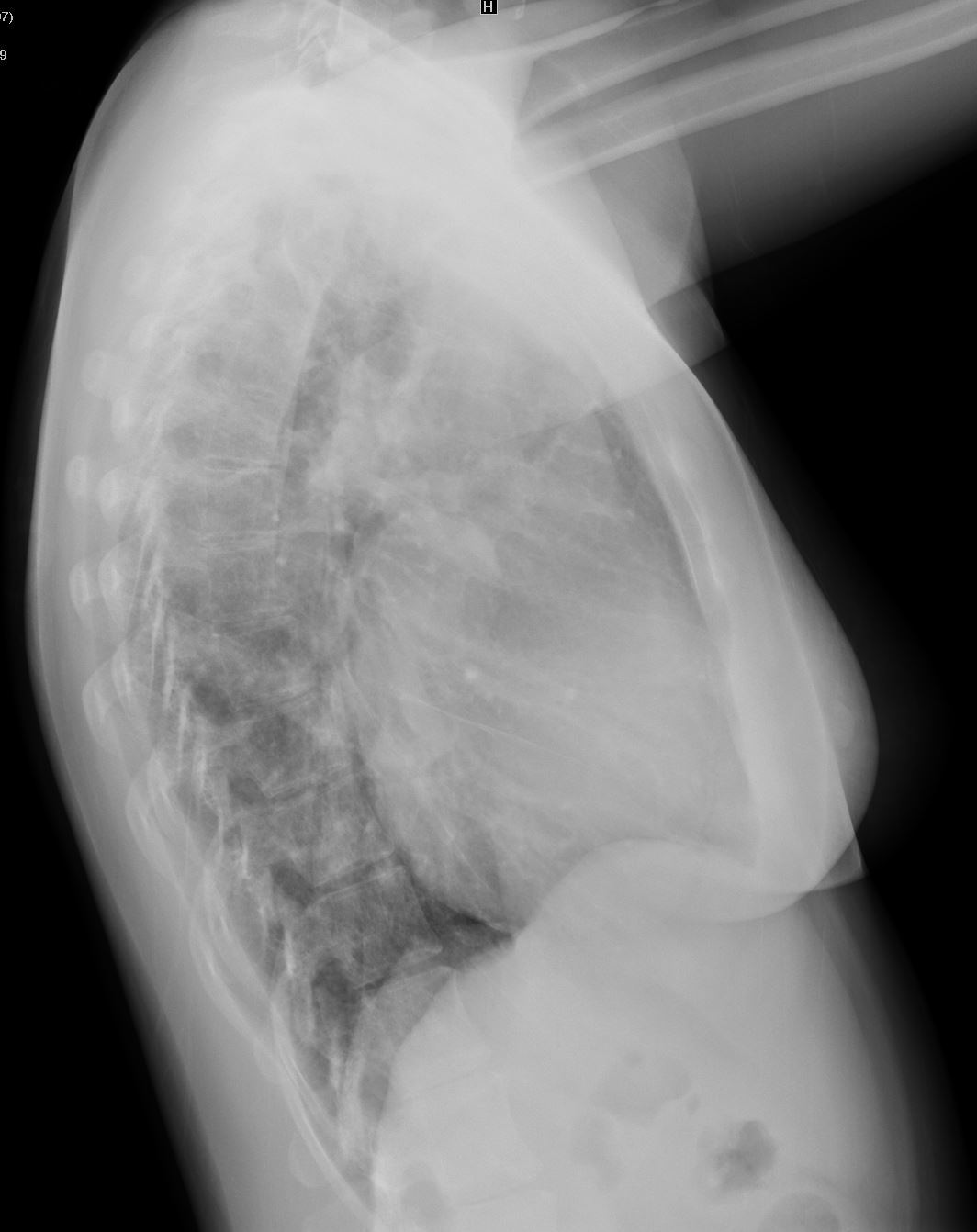
CXR
CXR shows cardiomegaly, with enlarged main pulmonary artery and enlarged bilateral enlarged pulmonary arteries.
The right upper lung field is lucent consistent with the patients known Swyer James Syndrome
Additionally, the right and left hilum are prominent, which again may be secondary to pulmonary hypertension

The right upper lung field is lucent consistent with the patients known Swyer James Syndrome
Ashley Davidoff MS TheCommonVein.net LPA-from-Aorta-001
Left Ventricular Hypertrophy
Ashley Davidoff MS TheCommonVein.net pulmonary artery off aorta 002
Echo
- The left atrium is severely enlarged.
- RV systolic function
- mild RV dysfunction.
- RV wall thickness is
- increased (8 mm).
- Mild ventricular septal flattenning
- mild to moderate tricuspid regurgitation.
- estimated PA pressure of
- ~105/45 mmHg.
- Mild to moderate pulmonic valvular regurgitation.
- inferior vena cava is < 2.1 cm and exhibits reduced respiratory
variability consistent with a - right atrial pressure of ~ 8 mm Hg.
- consistent with severe pulmonary hypertension.
- Chest CT showed
- possible PDA
- physical exam not consistent
- no differential cyanosis,
- no erythrocytosis and
- normal LV dimensions.
- ? additional shunting
Aorta to LPA
Ashley Davidoff MD TheCommonVein.net
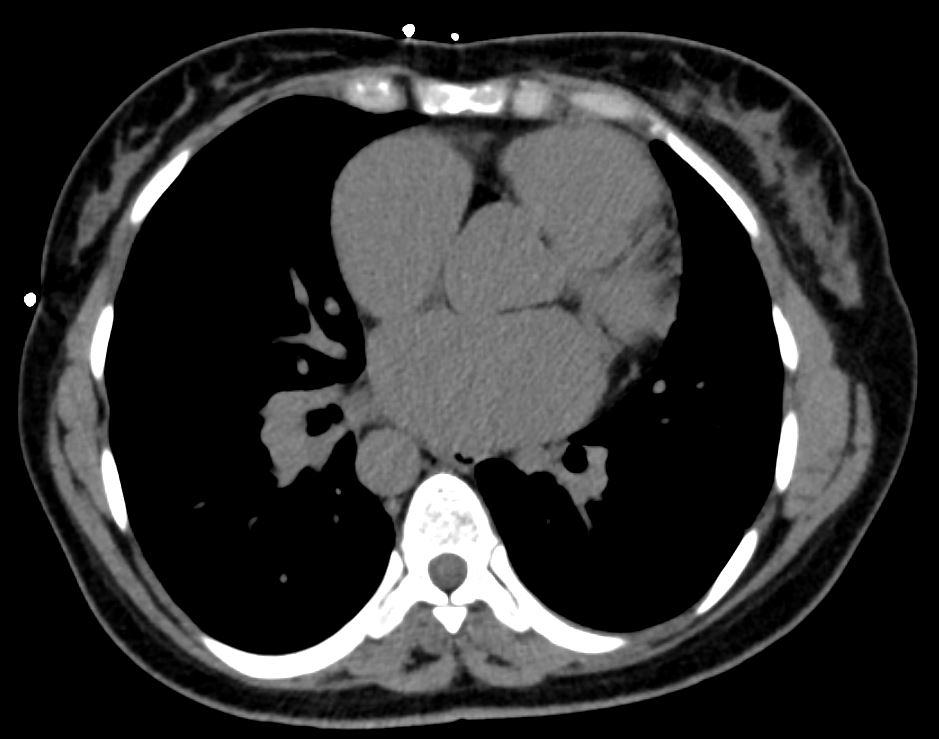
LAE
Ashley Davidoff MD TheCommonVein.net LPA-from-Aorta-003
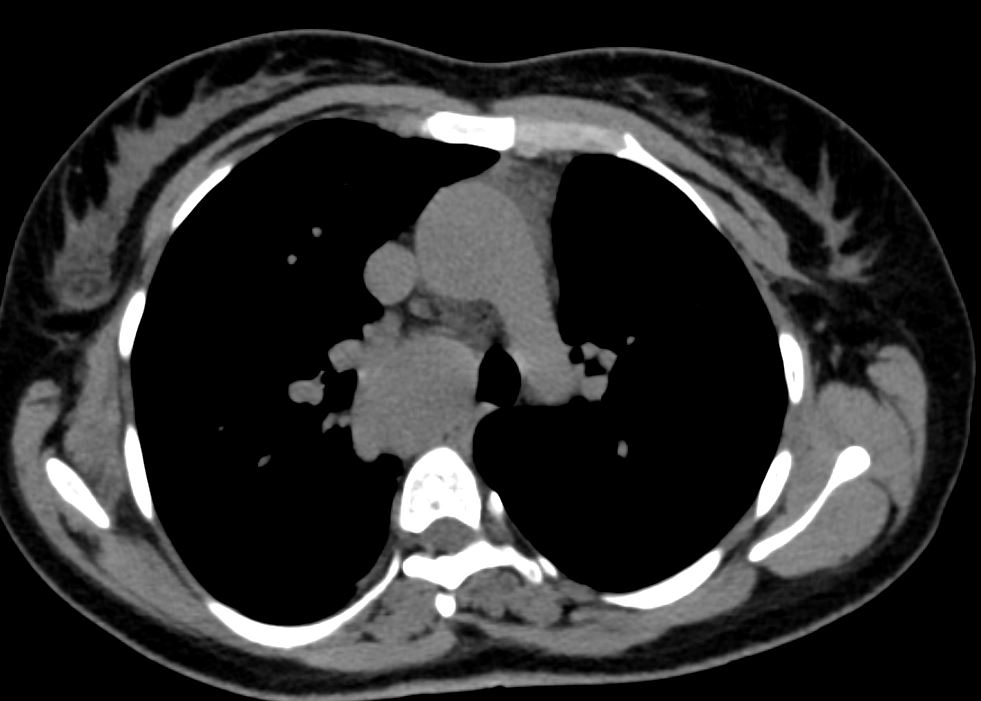
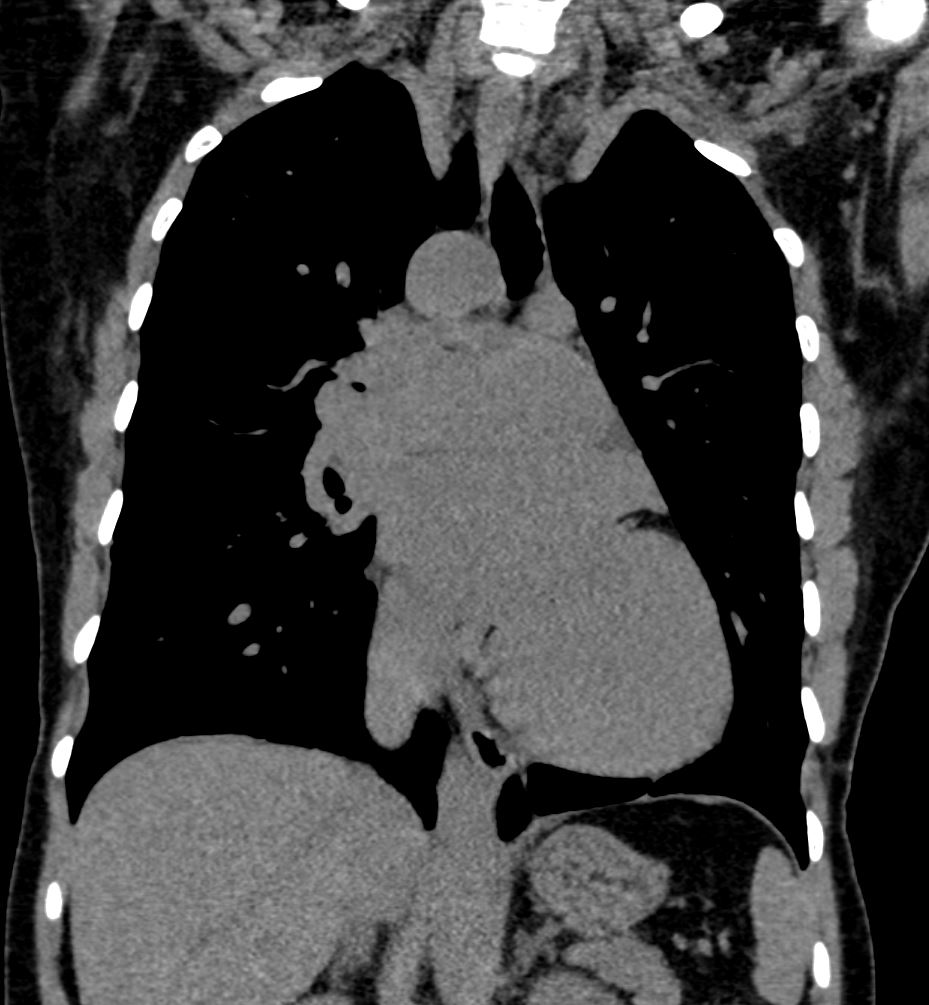
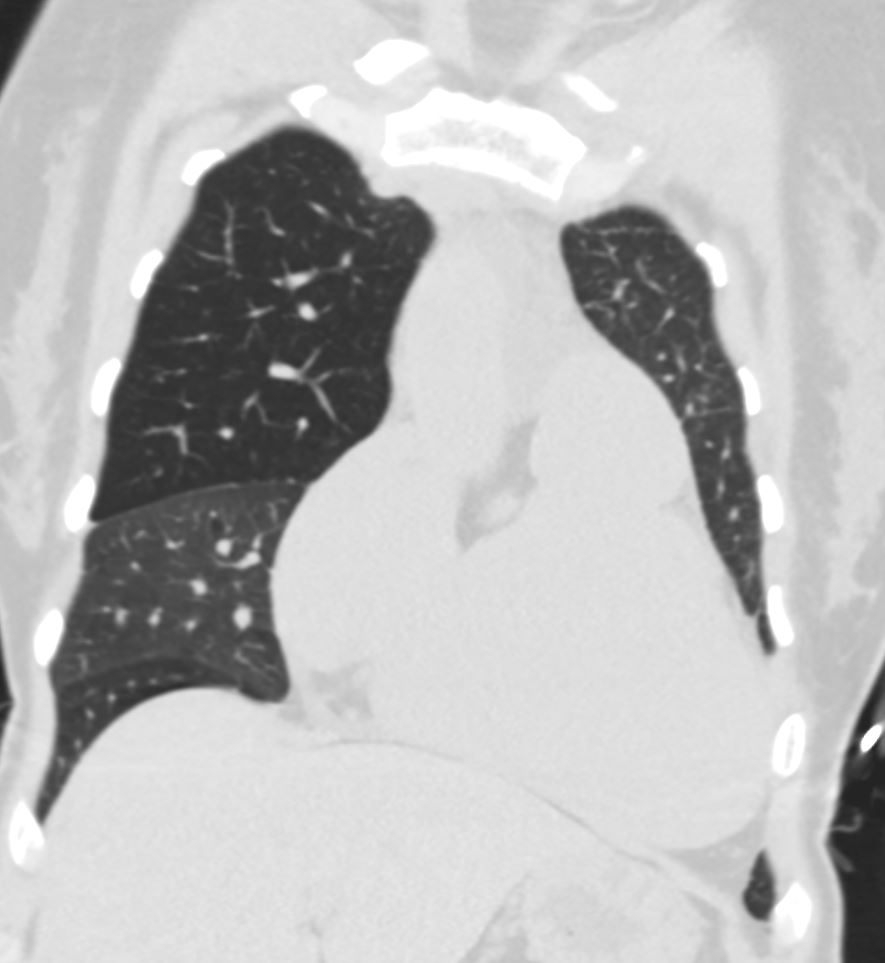
Enlarged MPA and Pulmonary Hypertension
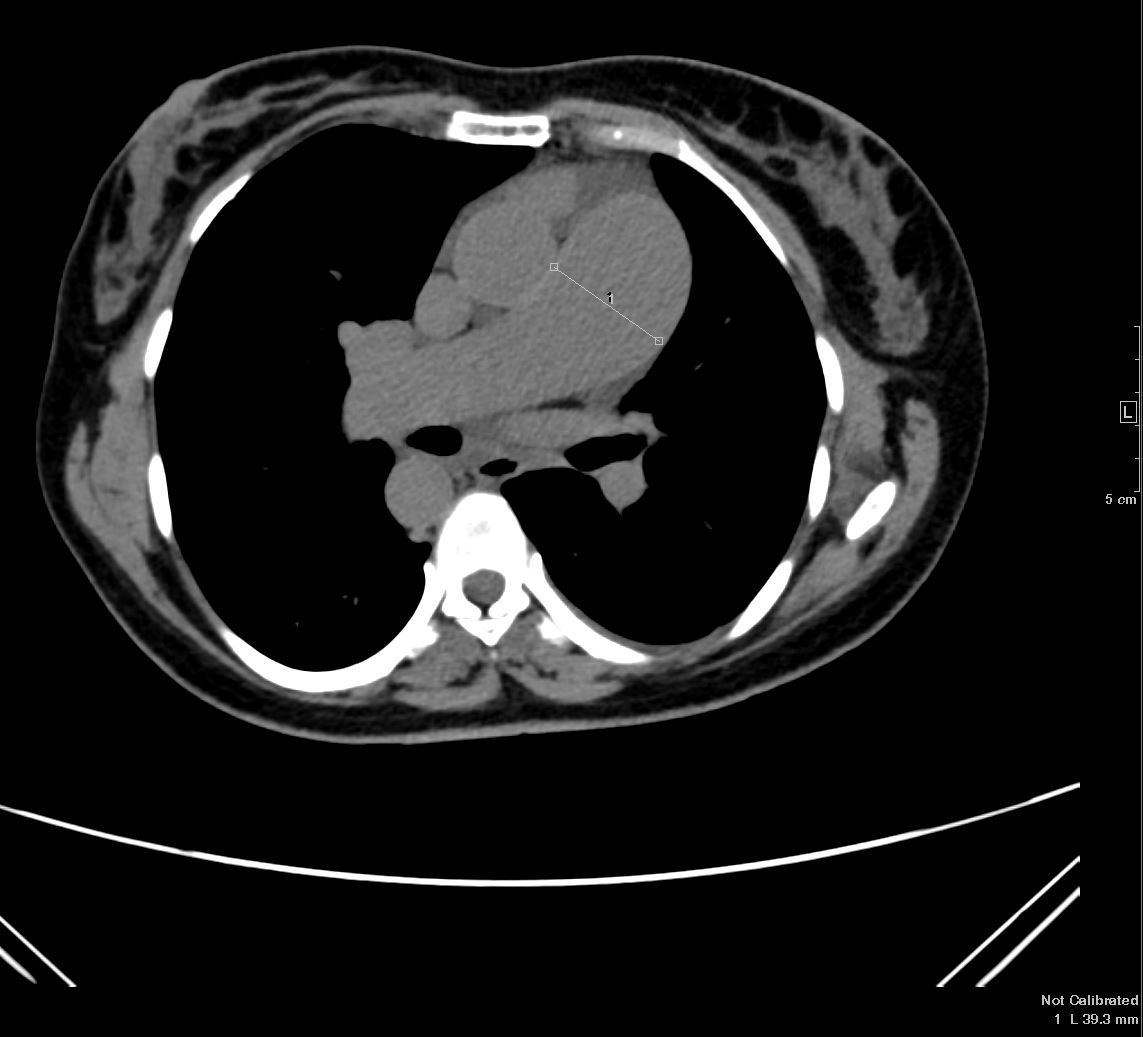
CT shows an enlarged main pulmonary artery Ashley Davidoff MD TheCommonVein.net
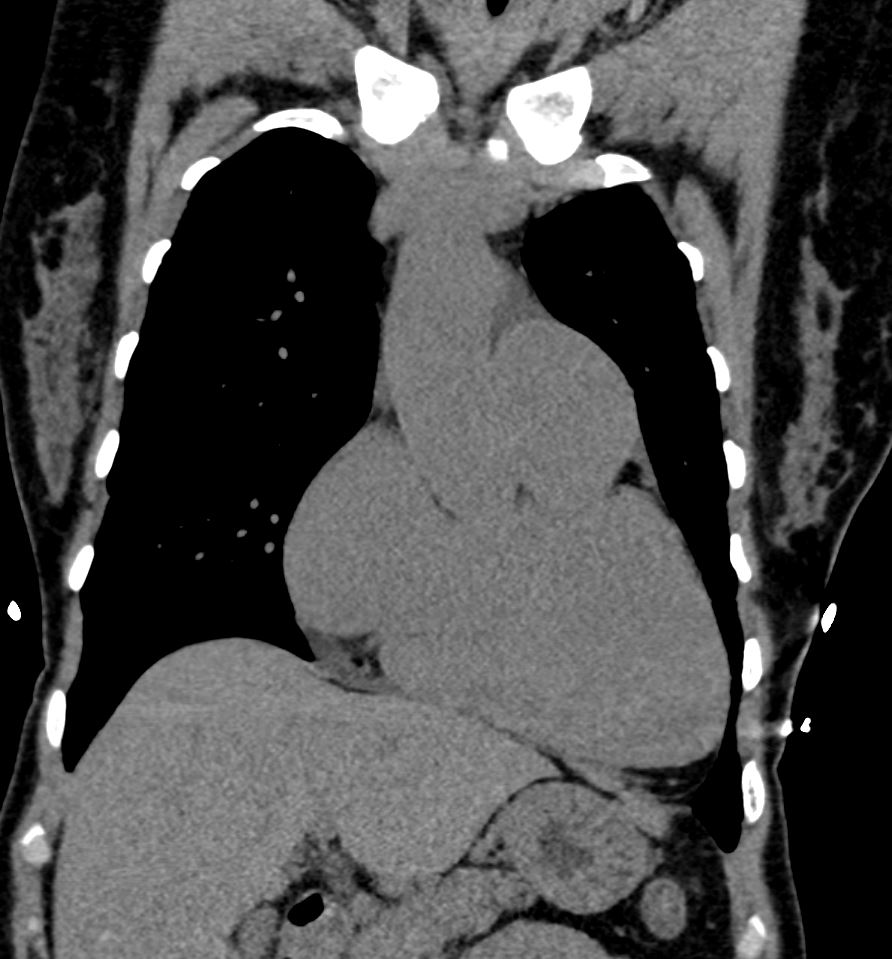
Coronal CT shows an enlarged main pulmonary artery Ashley Davidoff MD TheCommonVein.net LPA-from-Aorta-003b
RAE and LVE
Ashley Davidoff MD TheCommonVein.net LPA-from-Aorta-003
Right Aortic Arch

Ashley Davidoff MD TheCommonVein.net LPA-from-Aorta-003
Ashley Davidoff MD TheCommonVein.net LPA-from-Aorta-003b
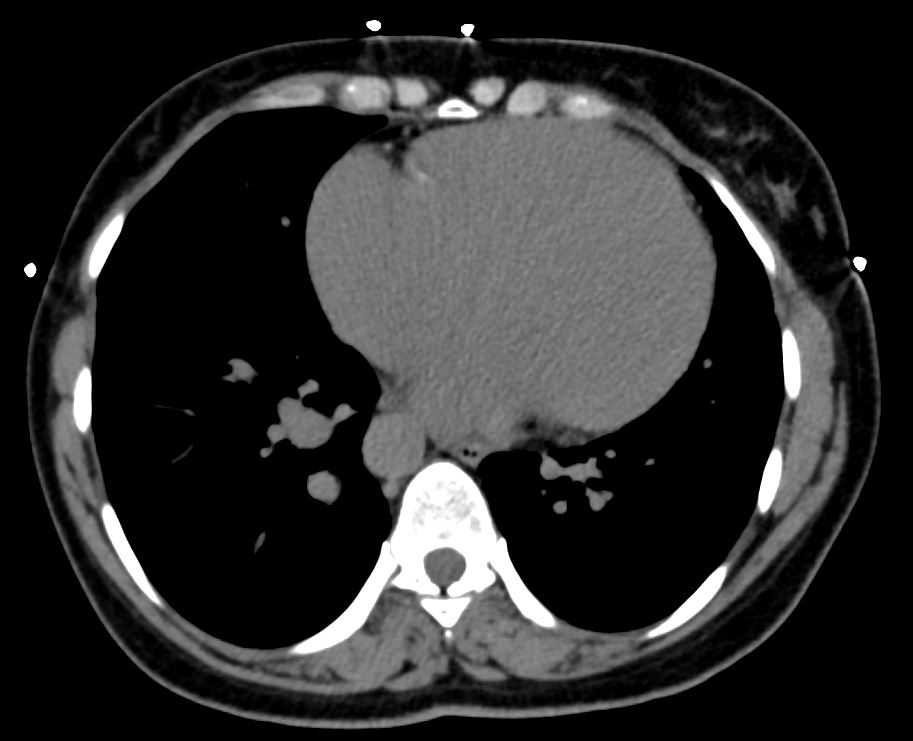
PDA Aorta to Right Pulmonary Artery

Ashley Davidoff MD TheCommonVein.net LPA-from-Aorta-003
? PDA Aorta to Right Pulmonary Artery

Ashley Davidoff MD TheCommonVein.net LPA-from-Aorta-003a

CT in sagittal projection suggests a PDA from the right aortic arch to the pulmonary artery Ashley Davidoff MD TheCommonVein.net CT LPA-from-Aorta-003a01
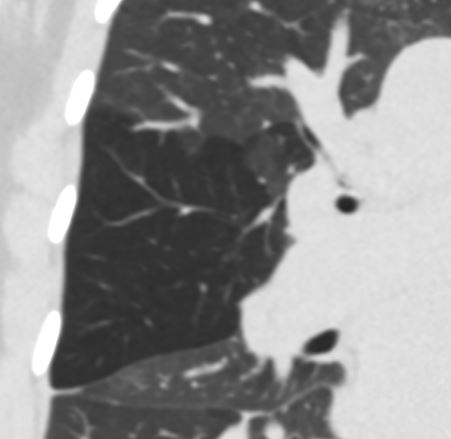
Swyer James
Hyperlucent Anterior Segment of the RUL
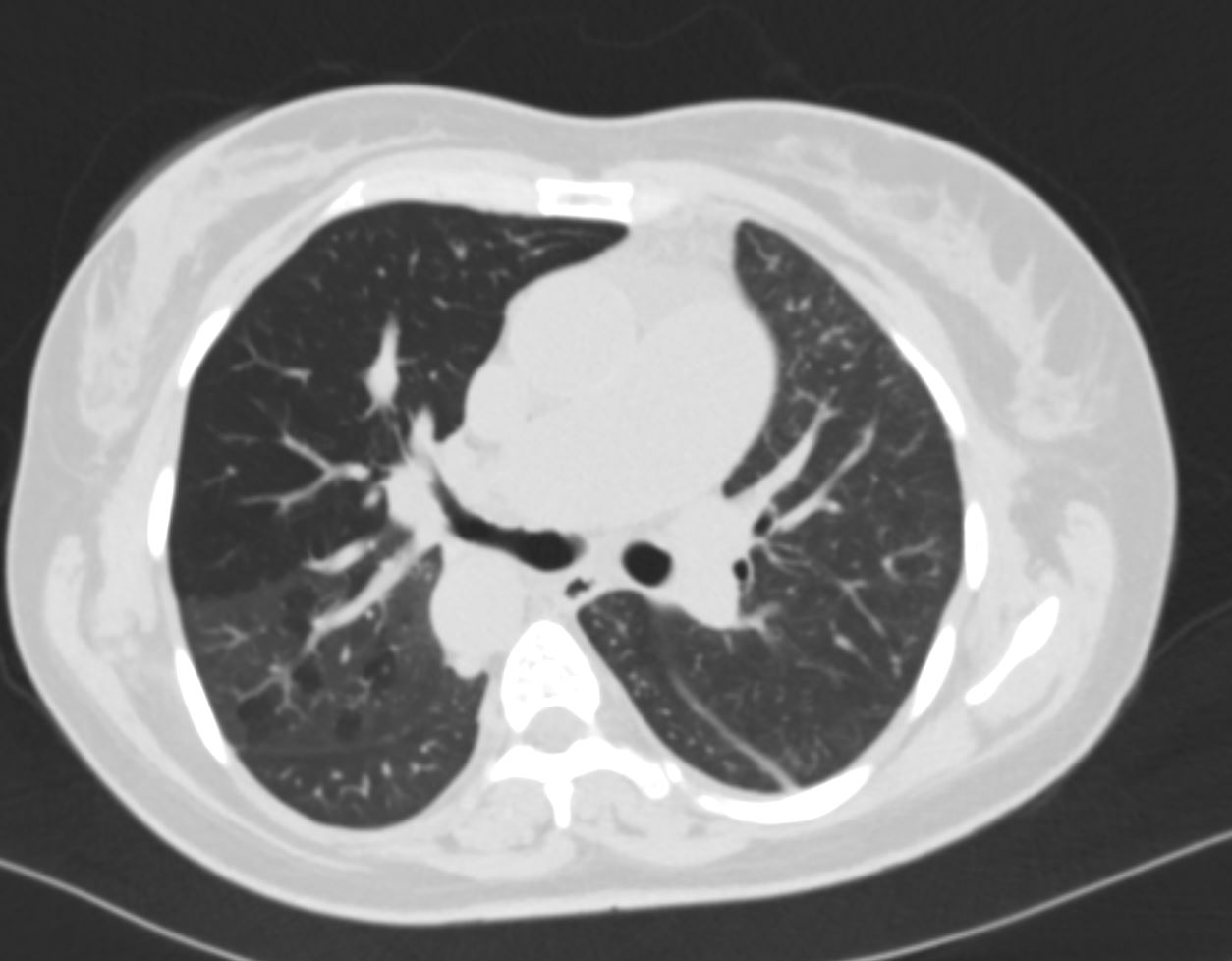
CT in axial projection suggests shows a hyperlucent anterior segment of the right upper lobe, narrowing of the segmental airway, and mosaic attenuation in the posterior segments Ashley Davidoff MD TheCommonVein.net artery-off-aorta-012

CT in coronal projection shows a hyperlucent anterior segment of the right upper lobe Ashley Davidoff MD TheCommonVein.net artery-off-aorta-013
Do you see a bull made of the soft tissues looking at the lucent lung?
Keep your eye on the eye of the bull as it will get progressively smaller as the bull goes to sleep and the airway narrows
CT in coronal projection shows a hyperlucent anterior segment of the right upper lobe Note the patent segmental airway subtending the upper lobe If you look with an artistic eye you can see a bull made of soft tissues looking at the hyperlucent lung The patent segmental airway is the “eye of the bull”) Ashley Davidoff MD TheCommonVein.net artery-off-aorta-014
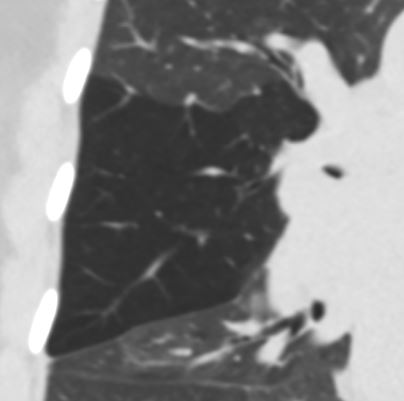
CT in coronal projection shows a hyperlucent anterior segment of the right upper lobe Note that the “eye of the bull” has become smaller as the anterior segmental airway becomes progressively narrowed Ashley Davidoff MD TheCommonVein.net artery-off-aorta-014b
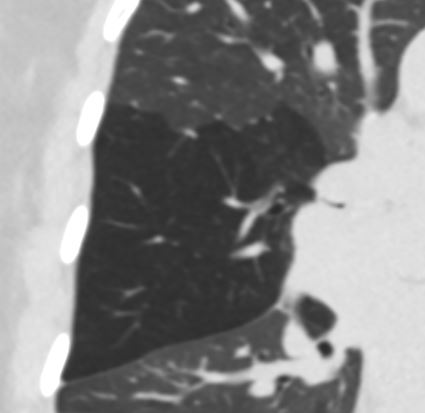
CT in coronal projection shows a hyperlucent anterior segment of the right upper lobe Note that the “eye of the bull” has become smaller as the anterior segmental airway becomes progressively narrowed Ashley Davidoff MD TheCommonVein.net artery-off-aorta-015
CT in coronal projection shows a hyperlucent anterior segment of the right upper lobe extending to the apex. This finding helps us understand why the ventilation in the VQ scan is deficient in the upper lung extends to the apex despite normal aeration of the superior segment Ashley Davidoff MD TheCommonVein.net artery-off-aorta-016
AP Ventilation View NM Shows Non Ventilation of the Right Upper Lung Field and Absent Ventilation of the Left Lung

AP of the ventilation component of the VQ scan shows non ventilation of the right upper lung field and absent ventilation of the left lung. The absent ventilation of the right upper lung field is explained by the expanded hyperlucent anterior segment of the right upper lobe which reaches to the right apex (see image above). The non ventilation of the left lung is explained by the absent pulmonary blood flow and the QP QS mismatch – just like a large occlusive PE to the left lung Ashley Davidoff MD TheCommonVein.net artery-off-aorta-016
Perfusion Scan – No Perfusion of the Left Lung

AP of the perfusion component of the VQ scan shows non perfusion of the left lung. The absent perfusion of the left lung is explained by the absent pulmonary blood flow since the blood to the left pulmonary artery is arising from the aorta – just like a large occlusive PE to the left lung Ashley Davidoff MD TheCommonVein.net artery-off-aorta-017
- Anomalous origin of the right or left pulmonary artery
- from the aorta
- rare prevalence of 0.33%
- 30% mortality rate within the first 3 months after birth (
- Anomalous origin of the right pulmonary artery
- most common subtype,
- accounting for more than 80% o
- >70% of patients with anomalous origin of the right pulmonary artery also have a
- PDA,
- anomalous origin of the left pulmonary artery
- less commonly associated with PDA
- first description by Fraentzel in
1868 - proximal subtype has been reported to be
- secondary to the disappearance of the fifth and sixth arches on the left,
- distal subtype occurs with a persistent
- fifth and absent sixth aortic arch
- PDA and
- atrial septal defect to be the most commonly associated congenital anomalies
Links and References
See TCV 5896