
Character
Copyright 2008
Introduction
The heart has a smooth glistening external surface surrounded by a variable amount of epicardial fat. It is red to maroon in color, muscular, rubbery, and distensible, but less so than organs of the gastrointestinal tract. Its inner surface is covered by a smooth white glistening surface edotheliumwhich has an underlying fibrovascular endocardium and subendocardium.
Thr atria have thin muscular walls, while the ventricles, particulalrly the left ventricle are much thicker.
|
Shining Glistening Endothelium of the Left Ventricle |
|
The left ventricle that has been opened along the ventricular septum shows the septal wall to your left and the free wall with the papillary muscles to your right. Note the glistening endothelium which has a whitish sheen. The myocardium lies directly under the endocardium. It is lighter red, muscular and rubbery. Note also the two sets of papillary muscles, the fibrous nature of the valves and the fibrous continuity of the mitral valve with the aortic valve. A VSD is noted onthe superior aspect of the septum. Courtesy Ashley Davidoff all rights reserved copyright 2009 08345b.8 |

|
The Glistening Endothelium |
|
The post mortem specimen reveals the opened the left atrium and a view of the anterior leaflet (al) and the posterior leaflet (pl)of the mitral valve. The patent foramen ovale is shown on the septal side of the left atrium. The glistening surface of the endothelium is seen throughout the LA, extending seamlessly onto the mitral valve. It is seen in cross section (white arrow) as part of the the thin smooth and white endocardium, together with a thin myocardial layer(maroon arrow) and pericardial layer (pink arrow). Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 01791c01.8s |

The heart is distensible, and on occasion in order to examine the heart, the anatomist ot pathologist distends the heart in a closed system with fixatives that include formalin, followed by embedding the heart in wax. The distensibility of the heart enables this process to display a distended heart, as it might appear in vivo.
|
Distensible nature of the Heart at Post Mortem |
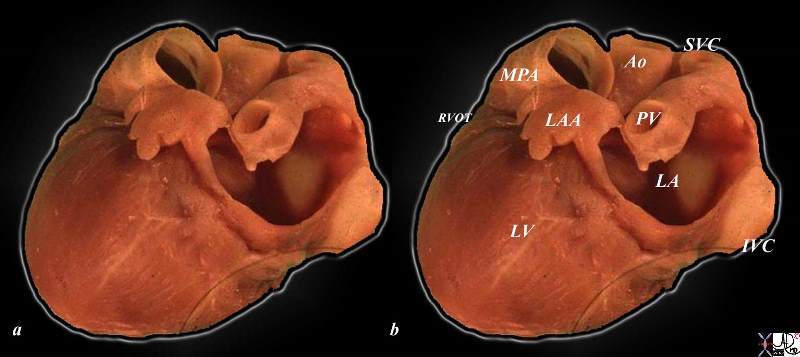
| The post mortem specimen was distended with fixatives including formalin under gravitational pressure, and then fixed in wax. The heart is viewd in a lateral projection tipped slightly to show the lateral and posterior wall of the LV. The main paulmonary artery (MPA), right ventricular outflow tract (RVOT), left atrial appendage (LAA) aorta(Ao), superior vena cava (SVC) pulmonary vein (PV) left atrium (LA) left ventricle (LV) and inferior vena cava (IVC) are shown. The distensible nature of the heart is demonstrated.
Courtesy Ashley Davidoff copyright 2009 all rights reserved 06559b03c01.8s |
|
Correlative in Vivo CT scan of the Heart Showing Distensibility |
|
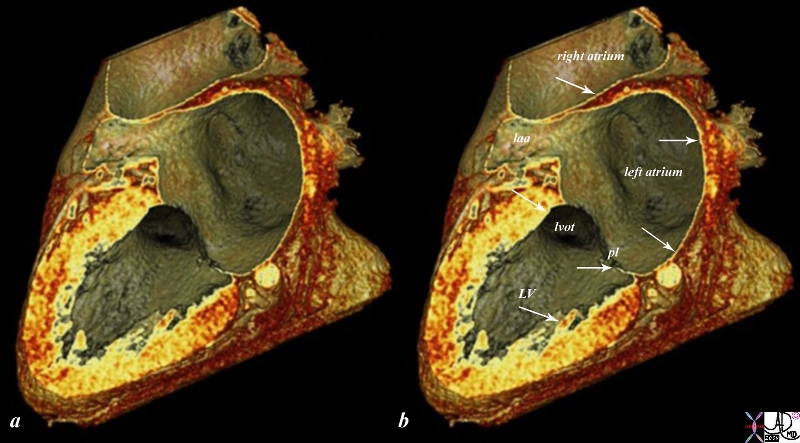
The reconstructed CTscan is in the same plane as the autopsy specimen above, and shows a distended left ventricle (LV) and left atrium (LA) and right atrium (RA). The thin endocardium (white arrows) throughout the heart is one continuous sheet of tissue connected across the whole circulatory system and it is more fibrous in nature. The thin white layer is seen in the left atrium, left atrial appendage (laa) over the posterior leaflet of the mitral valve (pl), in the left ventricle (LV) and in the right atrium. The surface of the left ventricle, left ventricular outflow tract (lvot) and right atrium are also lined by the endothelium. Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 47824c02.8s |
Characterising the heart on Imaging
On plain X-ray the the heart is characterized by its soft tissue density which is quite limited except when calcium is present in any of the components, best characterized by calcific pericarditis.
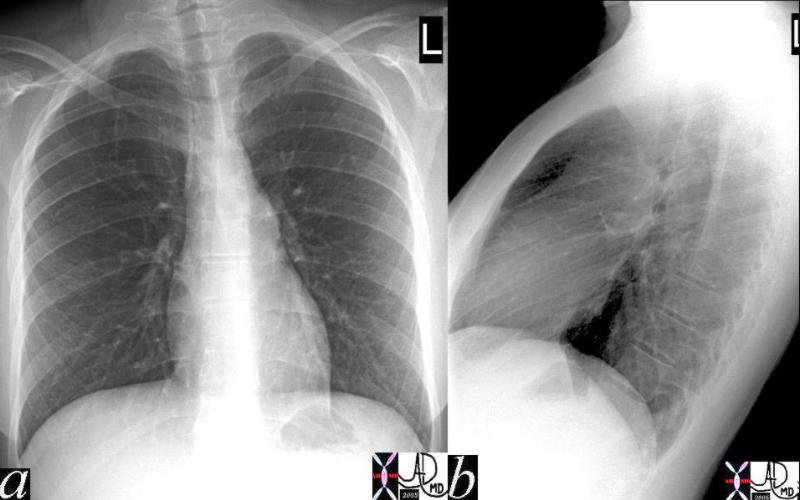
Normal X-ray Density |
|
X-rays characterize tissue by the attenuation characteristics of tissue. This normal chest X-ray defines the heart as soft tissue structure similar in density to the liver and spleen but dissimilar in density to the bone and air and fat. The evaluation is limited for characterization of the heart. 41819c Courtesy Ashley Davidoff MD medical students code chest imaging radiology plain film CXR lung normal |
CT imaging
CT scan is an advanced digital form of X-ray imaging that enables the gray scale to expand as well as allowing for axial tomographic technique. Characterization of the tissues is by density evaluation which is the net effect of the the way the X-rays are attenuated by the tisues. The density of each structure is reflected and measured by its Hounsfield units
CT Density Scale in Hounsfield Units
Air -1000 black
Fat -100HU light black
Water 0HU dark gray
Soft Tissue about 20-60HU light gray
Calcification +1000 white
cancellous bone +400HU white
contrast variable white
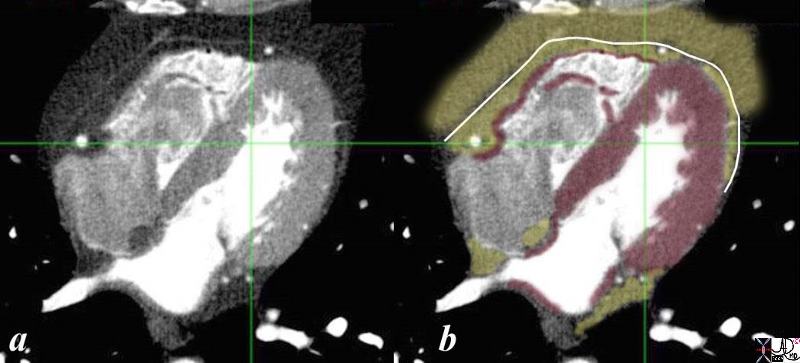
Characterizing the Heart by CT Density |
| CTscanning is the digital form of X-ray evaluation characterizes tissue by showing their density. The myocardium is shown as a gray density in image a, usually measures between 20 and 70 Hounsfield units, being on the low end before contrast and on the high end after contrast. In image b the myocardium is in maroon. The pericardial density is also soft tissue in nature and appears as a thin gray line in (a) and overlaid in white in b. Its CT density is also of a soft tissue nature. It is seen in exquisite detail in this image, despite it being submm in thickness because it is surrounded by fat on either side. The epicardial and pericardial fat are lower density (light gray in a and overlaid in yellow in b).
Contrast in the left side of the heart, coronary arteries and pulmonary veins is bright white because this study was timed to optimize the visualization of the coronary arteries. On the other side of the heart, unopacified blood (dark gray) is entering the right atrium at the tail end of the intravenous bolus injection, chasing the last potuion of the bolus in the right ventricle which contains a combination of unopacified and opacified blood. A tiny dot of black air is seen in the anterior portion of the RV introduced during the injection. This small amount has no effect on the heart. Courtesy Ashley Davidoff MD copyright 2009 45147b01c01.8s |
Fat in the Myocardium |
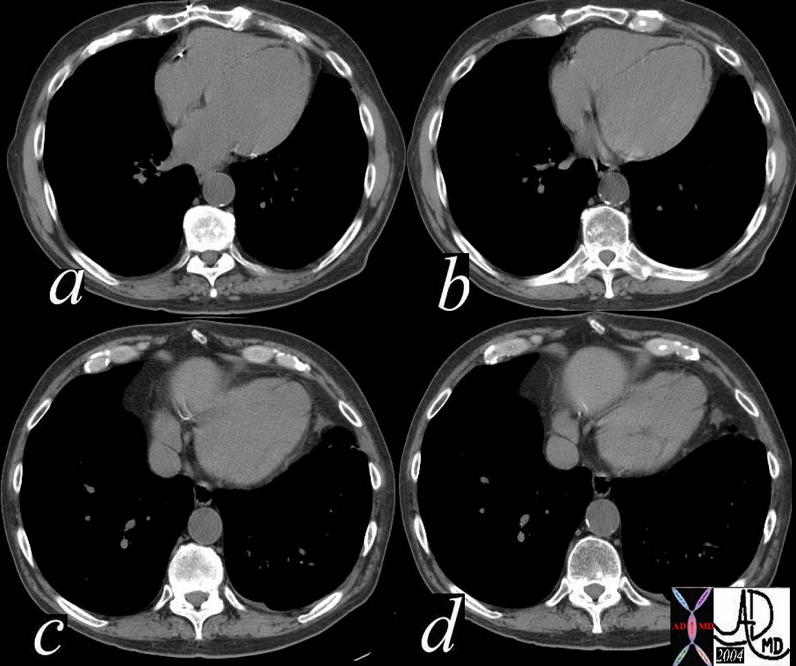
| The CT scan without contrast through the heart, shows a fine curvilinear black curviliear density in the distal septum and apex, that had a fat density (a,b). This appearance is abnormal and is characteristic of an old apical myocardial infarction. The characterization of the tissue as demonstarted bythis CT, is not possible with chest x-ray, and is best seen using CT technology.
There is also associated significant associated thinning of the myocardium also compatible with the prior infarction. There are a few punctate dystrophic calcifications in the septal component of the lucency. (a,b) The lucent abnormality also extends to the apex and the free wall of the LV. In images c and d the apex bulges forming an apical aneurysm. The findings are consistent with previous infarction with fatty changes in the infarcted region. Courtesy Ashley Davidoff MD. 38325c copyright 2009 |
Characterizing the Contractile Nature of the Heart
This aspect of characterizing the heart is one of the most important aspects of imaging and is best performed by technologies that have high temporal resolution that includes angiography, and echocardiography. MRI and CT have evolving and improving temporal resolution, but have not reached that of angiography and echocardiography.
For continuous loop right click on image and then click “loop is off”
This loop represents an unusual contraction abnormality of the apex of the left ventricle which pushes outward instead of inward at the peak of systole. this dyskinetic motion is commonly seen in patients with LAD disease, but this was a young patient with normal coronary arteries. This entity is called Takotsubo cardiomyopathy
Courtesy Michael Maysky MD
Copyright 2009
For continuous loop right click on image and then click “loop is off”
IHSS
This loop represents an echocardiogram of a patient with IHSS- idiopathic hypertrophic subaortic stenosis which is seen as a focal thickening of the septum. This area is slightly more echogenic than remaining myocardium. The septal leaflet (aka anterior leaflet) of the mitral valve is drawn toward the septum during systole (systolic anterior motion of the mitral valve = SAM) which is well demonstrated. these events can only be characterized by a dynamic study with high temporal resolution such as echocardiography.
Courtesy Michael Maysky MD
Copyright 2009
009vb01 from ashley davidoff on Vimeo.
Characterisation by MRI has been a major advance in evaluating structural and functional changes in the myocardium in health and disease. The technique of characterizing tissue involves magnetic fields and electromagnetic waves mostly by manipulating the hydrogen atoms in the tissues which interact because of the intrinsic spin of the proton. Apart from exquisite morphological, and functional evaluation, it has allowed for the evaluation of regions of acute and chronic ischemic entities in differentiating between infarcted myocardium vs stunned myocardium, and scarred myocardium, as well as being able to differentiate ischemic cardiomyopathies from other myopathies such as sarcoidosis.
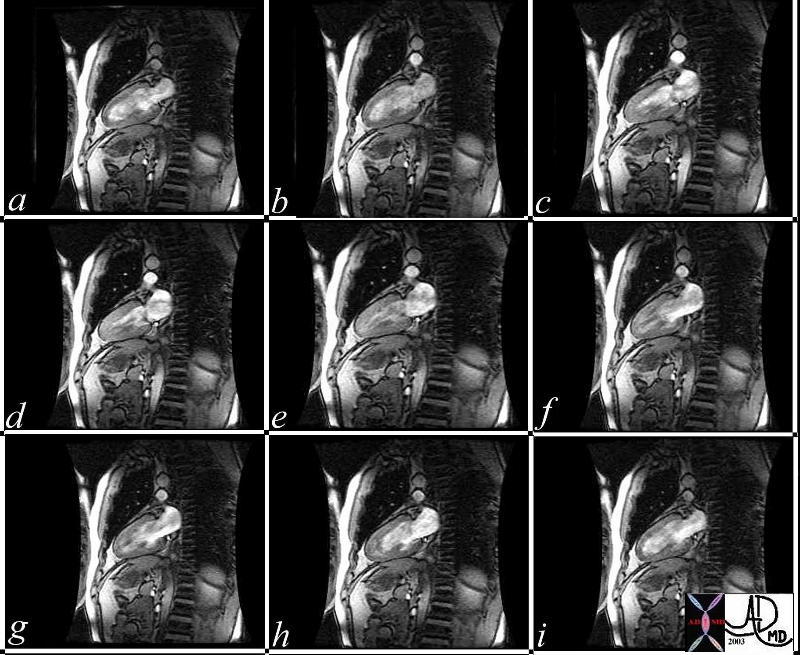
Normal left Ventricular Function and Structure |
| This series of MRI images of the LV and LA are a beautiful sagittal depiction of a normal heart in systole and diastole. Note the changes in LV cavity size as the heart in diastole (a) goes through progressive systole (b,c,d,e,f) and then goes through diastole again. (g,h,i)
Courtesy Rebecca Schwartz MD 38132c copyright 2009 |
Acute infarction is demonstrated by increase water content in the infarcted region characterized by bright region on T2 weighted sequences. Myocardial thinning in acute infarction is alsopresent. However the most specific is the accumulation of gadolinium in the infarcted region 5-10 minutes after injection. Delayed enhancement of infarcted myocardium differentites normal myocardium from ischemic myocardium. The area first involved is the subendocardial region, but if the entire wall is involved, transmural delayed enhancement occurs.
Scar tissue is characterized by administering a contrast agent and using a sequence called inversion recovery resulting in black normal myocardium and white scar tissue.
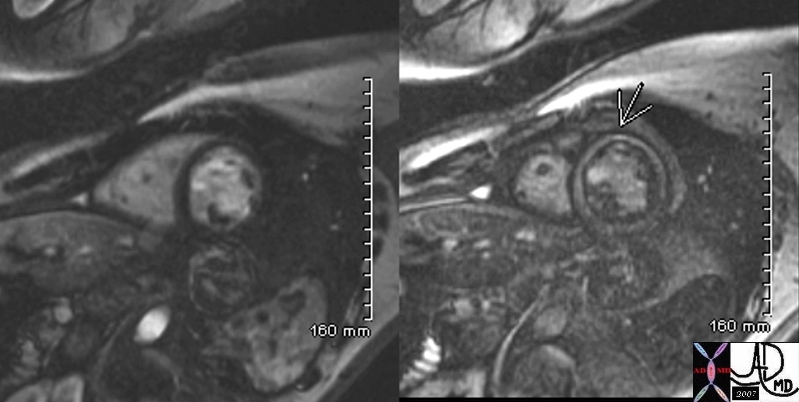
Delayed Circumferential Enhancement in Mid Myocardial Region |
|
This 34 year old male with sarcoidosis presents with dizziness and complete heart block. The delayed gadolinium study (right image) shows diffuse, non subendocardial enhancement. This is not consistent with ischemia, and rather with cardiomyopathy. Sarcoidosis cardiomyopathy was diagnosed. Davidoff MD 49740c01 |
Full thickness