
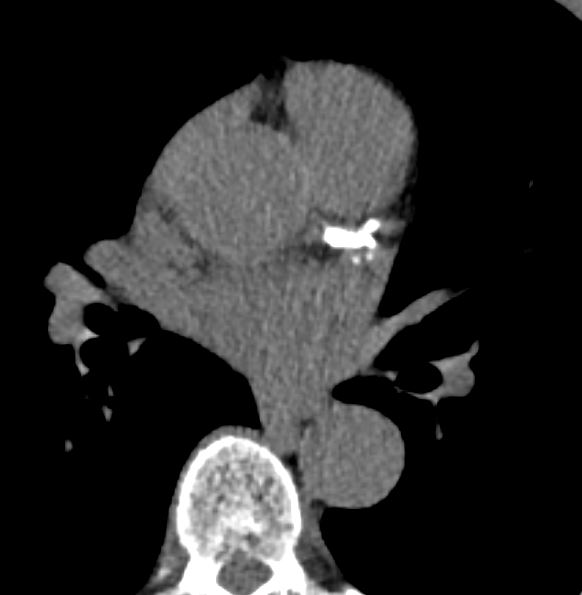
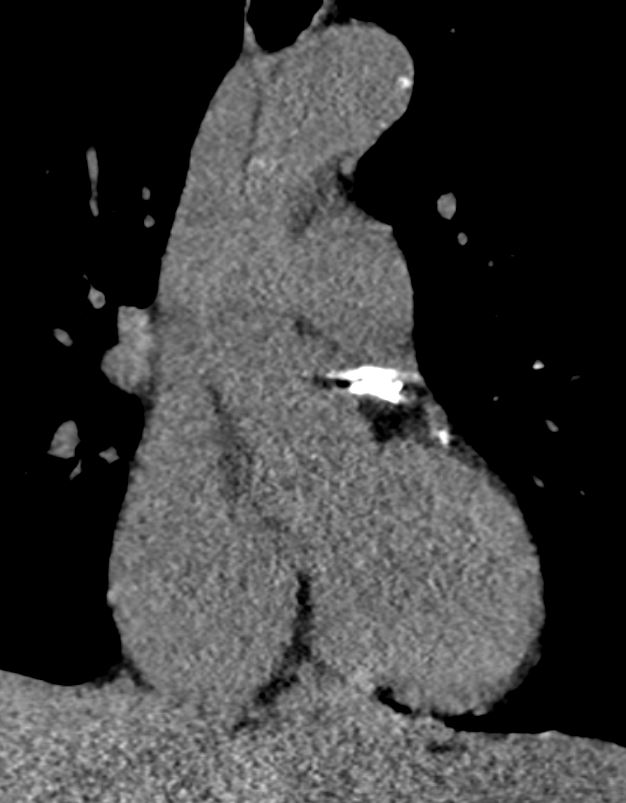
CT Lung CAncer Screening Study
Heavy calcification of the left main coronary artery and significant
calcification of the LAD, moderate calcification of the RCA and mild
calcification of the circumflex

CardiacCAth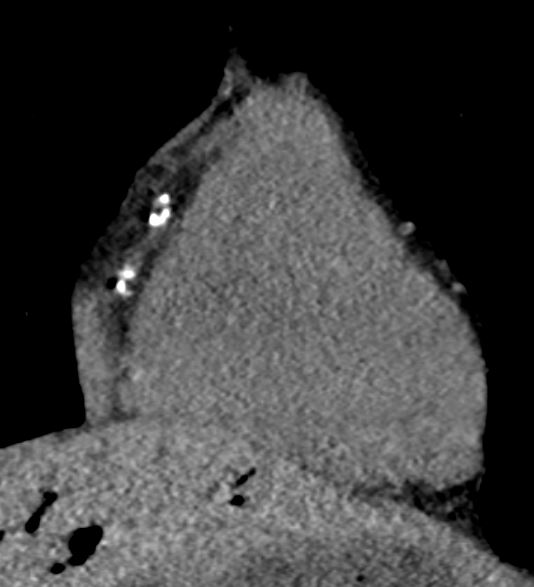

Cardiac Cath
INDICATIONS:
Chest pain
CORONARY CIRCULATION:
Right Dominant
Left Main: Mild Luminal Irregularities less than 30%
LAD:
Left Anterior Descending: Normal
LCX:
Left Circ: Mild Luminal Irregularities less than 30%
RCA:
RCA: Mild Luminal Irregularities less than 30%
Links and Refererences
Kwan, A, C et al The accuracy of coronary CT angiography in patients with coronary calcium score above 1000 Agatston Units: Comparison with quantitative coronary angiography Journal of Cardiovascular Computed Tomography 15 412-418 2021
For subjects in the lung cancer screening window, the relative risk of death due to ischemic heart disease is greater than 3 times that of a non-smoker (2).
Moreover, smoking reduces the time to development of coronary artery calcium (up to 10 years earlier for current smokers) when compared with non-smokers (3). .
Without any other risk factors, smokers already fall into the low end of intermediate risk.
In a nested case control study of over 4,500 individuals, 3 mm gated CT Agatston scores were compared with same day 6 mm non-gated Agatston scores. Not unexpectedly, scores were systematically lower on the thicker sections of the non-gated studies (due to volume averaging and hence underestimation). Despite this, there was a strong correlation with increasing calcium scores and mortality (14).
Agatston with coronary calcium defined as a lesion greater than 130 Hounsfield units with an area of at least 1 mm2.
Risk can then be stratified by overall scores with a score of zero indicating absence of calcified plaque, 1–10 minimal plaque, 11–100 mild plaque, 101–400 moderate plaque, and >400 severe plaque (5)