
HX 50-year-old female with fatigue and palpitations
Initial echo showed mildly reduced ejection fraction of 49%, mildly enlarged LA, with normal sized LV cavity, and mild LVH, and mild diastolic dysfunction with regional wall abnormalities. There was no evidence of RV dysfunction.
The first MRI showed a normal ejection fraction of 38%, with basal hypokinesis and LGE in the lateral and basal region with subendocardial sparing. Additional LGE was noted along the basal septal region. Dilated cardiomyopathy was felt to be likely.
Subsequent MRI done 2 months later showed mildly enlarged left ventricle with an EF of 44% with LGE in the lateral and anterior , extending from the base to mid body with transmural involvement. Additionally intramural involvement of the inferior wall and patchy intramural enhancement of the septum and anterior wall .
Subsequent echo showed overall improvement but with dilated left and right atria and normal LV and RV, improved regional wall abnormalities, EF of 50-54%, and normal PA pressure (<36mmHg)

Ashley Davidoff MD.
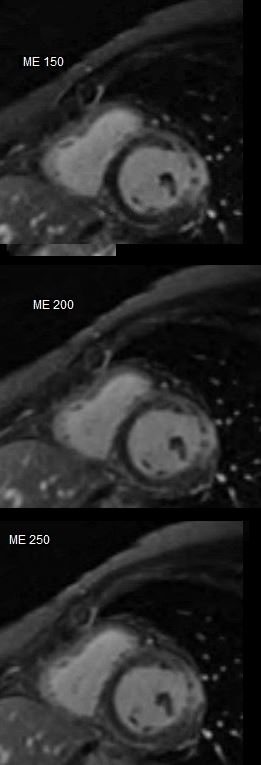
INABILITY TO NULL
Ashley Davidoff MD.
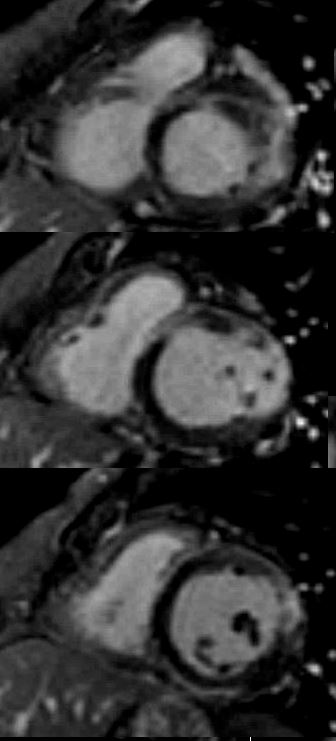
LGE pattern shows anteroseptal mid myocardial and linear pattern and transmural in the lateral wall.
Ashley Davidoff MD.

Ashley Davidoff MD.
References and Links
Buchholz S et al Cocaine-induced myocardial injury identified as multiple mid-wall foci of enhancement by contrast-enhanced cardiac MRI and large troponin rise
- TCV