
Chest Pain
The Common Vein Copyright 2008
Author Dima Quraini MD
Editor Ashley Davidoff MD
Chest pain is defined as the painful sensation that is classicially felt in the front part of one’s body, between the neck and the upper abdomen. It can have many causes, that range from life threatening conditions such as myocardial infarction and aortic dissection, to more benign conditions such as indigestion, heartburn, and gastoesophogeal reflux, costochondritis, and muscular aches. We do however include in the module back pain that may reflect significant chest disease such as pulmonary embolism, pleurisy, and aortic dissection, while also sometimes reflecting abdominal disease such cholecystitis and kidney stones..
| Characteristics of Chest Pain |
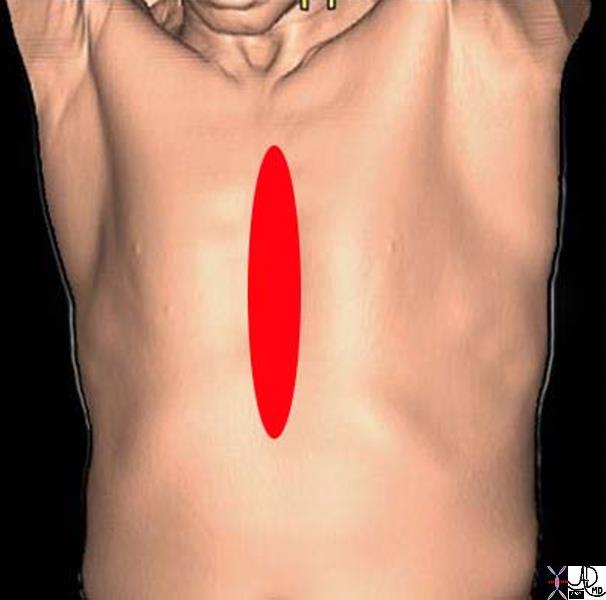
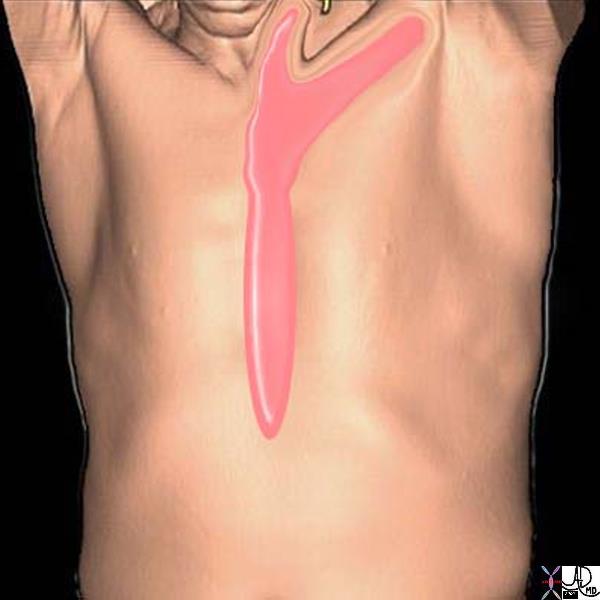
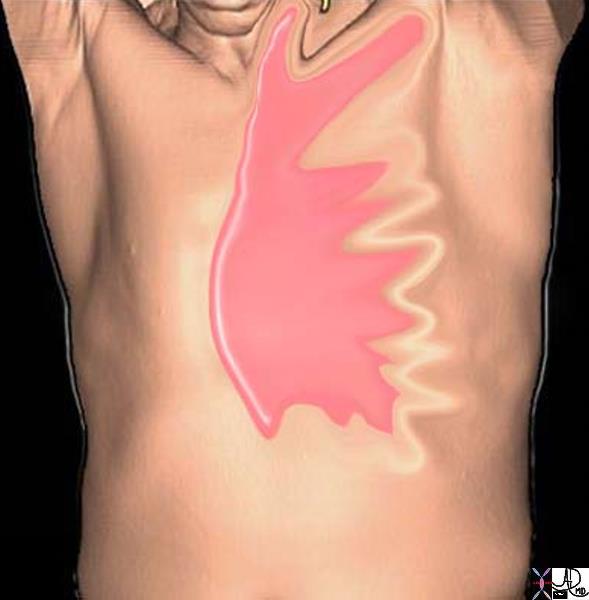
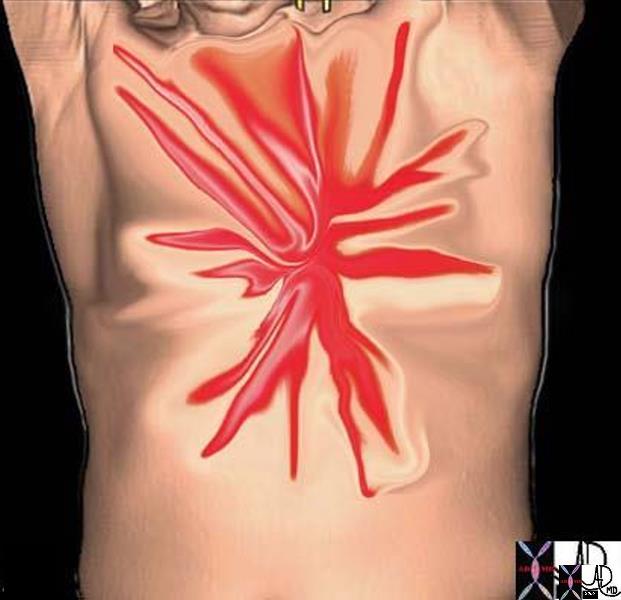
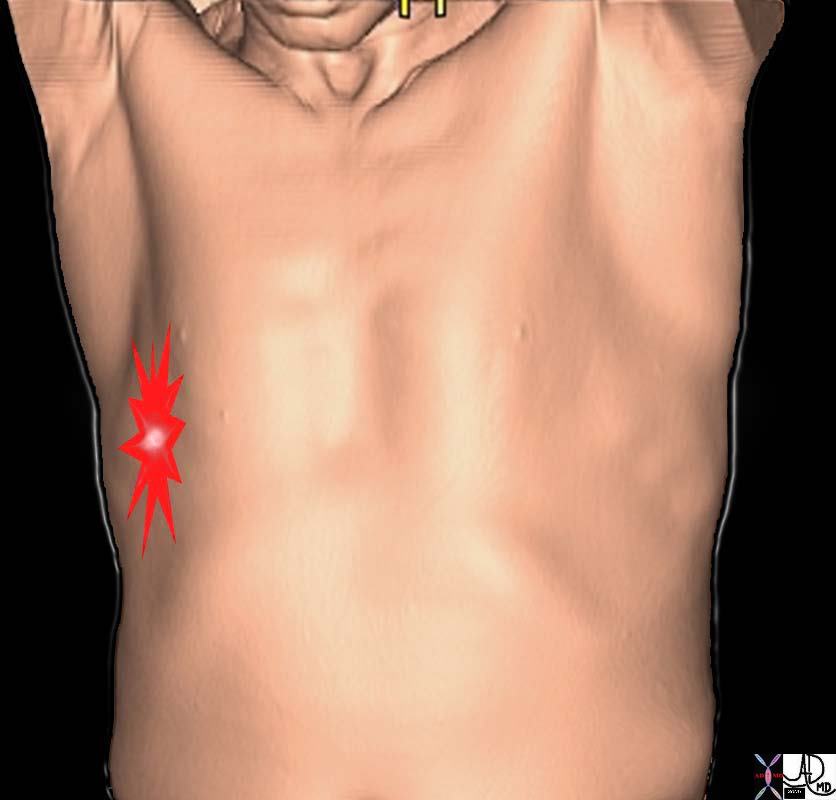
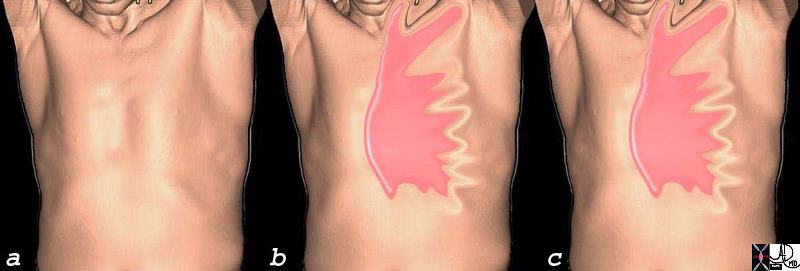
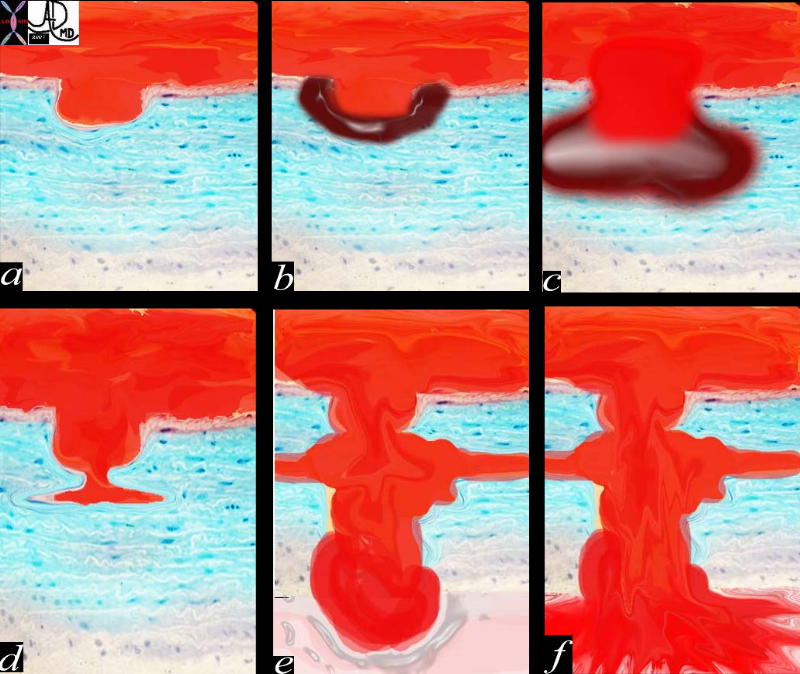
| In the above diagram and through the text, we attempt to depict the nature of the pain diagramatically. The more severe pains are shown in brighter red and the spiculated shapes reflect sharper pain. Thus the top left image is severe burning retrosternal pain characteristic of GERD with esophagitis. The top middle image is a pressure type pain that radiates o the neck, characteristic of angina and sometimes seen in esophageal spasm. The top right image is a more diffuse discomfort or pressure and is seen in angina and myocardial infarction. The bottom left image is sharp lancinating severe almost devastating pain characteristic of acute aortic dissection. The focal sharp pain in the middle image aggravated by deep inspiration is characteristic of pleuritc pain and pericarditis, whil the pain along a dermatome on bottom right is seen in herpes zoster (shingles).
71197c05a 71197c07a 42540c02a05 71197c08a 71197b03p 71197c04a Davidoff Art Courtesy Ashley Davidoff MD Copyright 2008 |
Chest pain sometimes does not result in sufficient discomfort for the patient to seek medical attention, and unfortunately sometimes serious disease is not necessarily associated with severe pain.
Diagnosis of the underlying causes often is the result of a careful clinical history, and triage to further diagnostic workup usually includes a chest X-ray, EKG and cardiac enzymes.
Medical therapy for pain includes analgesics, antacids, anticogulation and intravenous thrombolytics. Minimally invasive therapy provides intraarterial therapy, angioplasty, and stenting, while surgical therapy provides coronary bypass and repair of dissections.
Background to entity
Chest pain is one of the most common complaints encountered in the emergency room, hospital ward or physician’s office. It is essential as a caregiver to have a thorough understanding of the variety of chest pain syndromes in order to distinguish between life threatening disease and the benign entities. Meticulous attention to the history and the characteristics of the pain often is the most important aspect in diagnosis. Patients who are mistakenly discharged after presenting with chest pain secondary to myocardial infarction suffer twice the mortality rate than patients who were admitted. Also, missed diagnosis of serious diseases lead to cumbersome legal costs. However, many other diseases associated with low short-term mortality present with chest pain rendering the hospitalization of all patients presenting with such a complaint inconvenient and costly to an overburdened health system.
Structural Considerations
The chest is composed of muscle, bone and nerves that create the chest wall that itself harbors the heart, the pericardium, the large vessels, the lungs, the pleura and the esophagus. Any process involving these structures can cause chest pain.The pain may be visceral as in cardiac pain and esophageal pain, but on the other hand may be somatic when the pericardium, pleura, or skin is involved.
Causes and predisposing factors
The differential diagnosis of chest pain is large and encompasses diseases from many systems. Inflflammatory, infectiuos, neoplastic, trumatic, circulatory, immune, idiopathic disorders can all be the cause of chest pain. A well-obtained clinical history is crucial in determining the origin of the pain and in guiding the ensuing management. The clinical history should focus on the characteristics of the pain, the time of onset, the aggravating and relieving factors and any accompanying symptoms. The patient’s prior medical history is also important as it may make one diagnosis more likely than another.
Past medical history and family history
The patient’s prior medical history is important as it can provide clues about the cause of the patient’s current presentation. Patients with known coronary artery disease, hypertension and diabetes mellitus are at increased risk of undergoing an acute coronary syndrome. A family history of coronary artery disease particularly in young parents (men <55yrs, women <60yrs) predispose the patient to coronary disease. Younger patients presenting with chest pain may also suffer from myocardial ischemia or infarction particularly in the context of cocaine use. Therefore, a detailed history of substance use including tobacco and alcohol consumption should be obtained. A urine toxicology screen can be checked if there is a suspicion of drug use.
Risk factors
Risk factors for other causes of chest pain should also be sought . For example, a prior episode of deep venous thrombosis or pulmonary embolus, sedentarism, a recent surgical intervention or underlying malignancy may suggest a pulmonary embolus as the cause of a patient’s chest pain. A young tall patient who presents with an acute onset of chest discomfort and shortness of breath is unlikely to be undergoing an acute coronary syndrome. He or she would be more likely to have a spontaneous pneumothorax and if MArfanoid, aortic dissection must be considered. Uncontrolled hypertension predisposes patients to aortic dissection.
Cardiovascular causes of chest pain:
Myocardial ischemia and infarction
Myocardial ischemia is one of the most common and serious causes of chest pain in patients. Approximately 20% of patients presenting to an emergency room with chest pain have underlying myocardial ischemia or infarction. Although most patients presenting with chest discomfort are discharged without a diagnosis or a non-cardiac cause to their pain, it is crucial to seek the symptoms and signs of myocardial infarction as it carries a high mortality if left untreated. However, with early recognition and the timely institution of appropriate therapy, the mortality rate is significantly reduced.
The disparity between oxygen supply and consumption may result from coronary atherosclerosis, coronary thrombus, coronary vasospasm or emboli. Thrombus formation secondary to a ruptured plaque leads to an abrupt loss of oxygen supply to the heart muscle supplied by the diseased coronary artery and leads to unstable angina or myocardial infarction.
Other rarer causes of acute occlusion of oxygen supply to the myocardium include a coronary embolism, coronary dissection or coronary vasculitis. Chronic angina, on the other hand, is due to the chronic narrowing of coronary arteries due to atherosclerosis. When oxygen demand is increased in the setting of tachycardia such as would occur during exercise or stress, the oxygen supply is limited by atherosclerosis and therefore is unable to meet that increase in oxygen demand. This disparity between oxygen supply and demand leads to myocardial ischemia and chest pain.
Angina
The classic presentation of myocardial ischemia was first described by Dr William Heberden in a lecture before the Royal College of Physicians in 1768. He claimed that “the seat of it, and sense of strangling and anxiety, with which it is attended, may make it not improperly be called angina pectoris”. The pain is usually precipitated by excercise or emotional stress, and lasts between 30 seconds and 30 minutes. The onset is acute, and intensifies within minutes, and is characterized by adjectives such as tightness, pressure, or heaviness, most commonly in the retrosternal region but it may involve the precordium. It is aggravated by continued excercise, and is characteristically relieved when the physical or emotional stress is abated or following administartion of nitroglycerine. The discomfort may radiate to the neck, jaw, or left arm. Associated symptoms include an impending sense of doom originally described as “angor animi” which literally means anguish of the soul. This sensation sometimes accompanies other life threatening situations when there is massive outpouring of catecholamines, such as aortic dissection and pulmonary embolism. Associated symptomss include shortness of breath, nausea and diaphoresis. It is usually although not necessarily precipitated by exercise or emotional stress. The episodes of angina recur usually with the same degree of excercise, and patients can predict their excercise tolerance. These episodes can also progress in frequency and can present while the patient is at rest, but do not usually wake the patient from sleep.
An important distinction should be made between patients presenting with a single and acute episode of chest pain versus patients who chronically develop chest pain on exertion. The latter is termed stable angina and can be managed medically unless the patient is symptomatic despite optimal medical therapy.
Stable Angina – Predictable Patterns a) No pain – excercise b) Pain Pressure Typical Distribution c) Relieved by Rest, TNG |
| Angina is characteristically a dull pressure like pain, that is precipitated by stress usually after a predictable distance of a walk or run for example. In a, the patient has no discomfort, develops pain after a fixed distance, and then stops. The pain is relieved
71197c07c substernal chest pain burning esophagus heart cardiac esophagitis reflux substernal chest pain radiating to neck and left arm relieved by rest and sublingual nitroglycerine angina CTscan 3D Courtesy Ashley Davidofff MD |
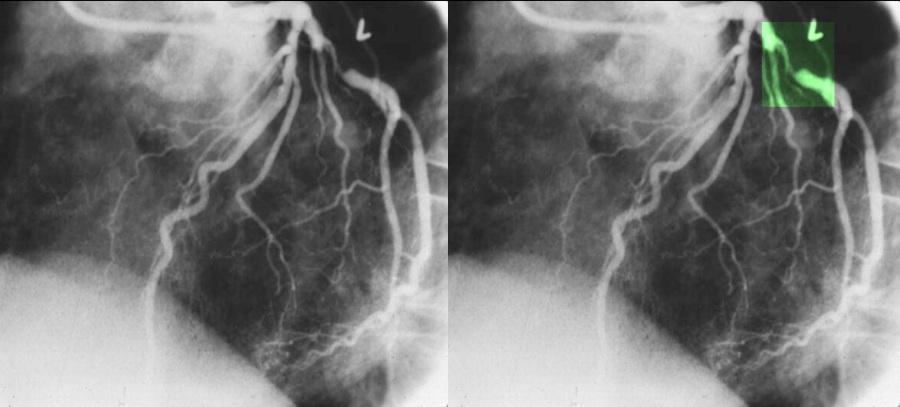
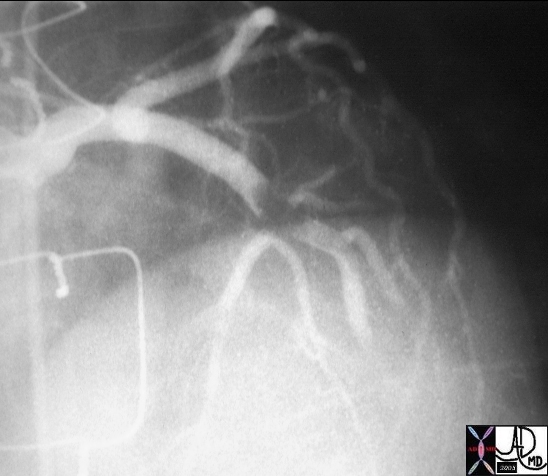
>70% Stenosis of the Left Circumflex Coronary Artery
|
| The coronary angiogram in the LAO projection shows a severe proximal stenosis (>70%) of the circumflex with some post stenotic dilatation. The second image has a green overlay indicating the region of disease with the post stenotic dilatation.
Courtesy Ashley Davidoff MD. 07023c |
On the other hand, the acute onset of chest pain at rest or minimal activity would be concerning for an acute coronary syndrome. Those patients need to be managed more aggressively as they are at risk of developing myocardial death or infarction.
Acute coronary Syndrome
When the pain appears to be of cardiac origin, and reflects a more serious nature in that it lasts longer than 20 minutes, is not relieved by rest or nitroglycerine then an entity called acute coronary syndrome is entertained.
The pain of acute myocardial infarction may be very similar to the pain of angina in its character and distribution but it is not relieved by rest nor nitroglycerine. It usually arises spontaneously, but may be brought on after eating a large meal or going out into the cold. It is relentless, ongoing, often accompanied with the “angor animi” sense of doom. It may be more severe than angina but not necessarily. Associated symptoms include nausea, diaphoresis, palpitations or shortness of breath
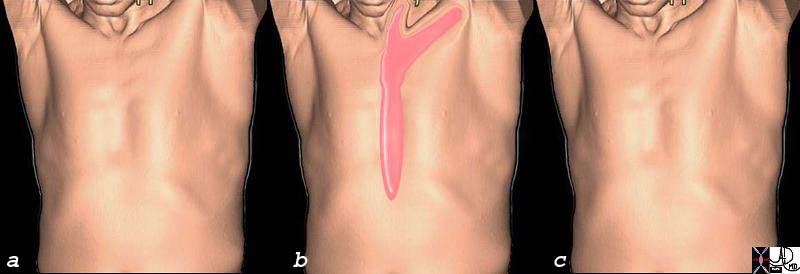
Acute Coronary Syndrome (a )is prior to the event, (b) Sudden Severe Pain Pressure Discomfort (c) Unrelieved by TNG and Rest and 1 hour later |
| In the diagram above, image a represents the patient without pain before the event. Sudden and evolving chest discomfort or pressure with radiation to the neck and left arm occurs (b) that is not relieved with nitroglycerine, and remains for longer than 20 minutes (c) suggests an acute coronary syndrome.
71197c08c.800 substernal chest pain burning esophagus heart cardiac esophagitis reflux retrosternal chest pain radiating to neck and left arm unrelieved by rest and sublingual nitroglycerine myocardial infarction time hours CTscan 3D Davidof art Courtesy Ashley Davidofff MD |
Acute coronary syndrome (ACS) is the term used to describe any one of the 3 following entities: unstable angina, non-ST elevation myocardial infarction (non Q wave MI) and ST elevation myocardial infarction (Q wave MI). Myocardial ischemia is the pathophysiological substrate for all the entities above, encompassed by the term acute coronary syndrome. Myocardial ischemia is caused by an imbalance between myocardial oxygen demand and supply secondary to coronary stenosis, obstruction, thrombosis or spasm. The chest pain in an acute coronary syndrome is caused by ischemia.
Unstable angina
Unstable angina is the clinical presentation of acute myocardial ischemia characterized by new onset chest pain within 1 month, chest pain at rest, chest pain lasting more than 20 minutes and not improving with nitroglycerin or chest pain more severe, more frequent and lasting longer than previously, without evidence of myocardial necrosis (no elevation of cardiac enzymes) and with or without EKG changes of ischemia. UA is a clinical diagnosis.
Myocardial infarction
Myocardial infarction is a circulatory disorder that is characterized by the necrosis of myocardial tissue caused by myocardial ischemia, and clinically characterized by the presence of symptoms of acute myocardial ischemia (ischemic chest pain or chest pain equivalent as dyspnea, diaphoresis, lightheadedness, palpitations), associated with characteristic EKG changes and biochemical markers of myocardial necrosis as reflected by typical rise and fall of cardiac enzymes: troponin I or T, CK-MB. Pathological diagnosis of myocardial infarction requires evidence of myocyte cell death (i.e. necrosis of the myocardium) as a consequence of prolonged ischemia.
An alternate approach to classifying these entities is based on the EKG, depending on the presence of elevation of the ST segment
Non ST elevation:
unstable angina (UA)
myocardial infarction (NSTEMI)
The incidence of finding thrombus in the coronary arteries in these patients is between 35-70%.
ST elevation:
ST elevation myocardial infarction (STEMI)
The incidence of finding thrombus in the coronary arteries in these patients is about 90%.
The diagnosis and classification therefore rest on the character of the EKG changes and biochemical markers of myocardial necrosis as reflected by typical rise and fall of cardiac enzymes: troponin I or T, CK-MB and classified as ST elevation (STEMI) or non ST elevation myocardial infarction (NSTEMI) based on the EKG

ST elevation in Anterior Myocardial Infarction |
| The 12 lead EKG shows ST segment elevation in leads V1- V4 (blue) indicating a ST segment elevation myocardial infarction. (STEMI )
76096 heart cardiac infarction STEMI 12 lead EKG blue lead shows ST elevation in leads V1 -V6 consistent with STEMI EKG Courtesy Philips Medical Systems |
The pathological diagnosis of myocardial infarction requires evidence of myocyte cell death (i.e. necrosis of the myocardium) as a consequence of prolonged ischemia.(Luepker)
Treatment depends on the type of infarction (STEMI vs NSTEMI), but attempts are usually made to lyse thrombus and open the vessels by angioplasty or stenting in a timely manner in order to salvage myocardium at risk.
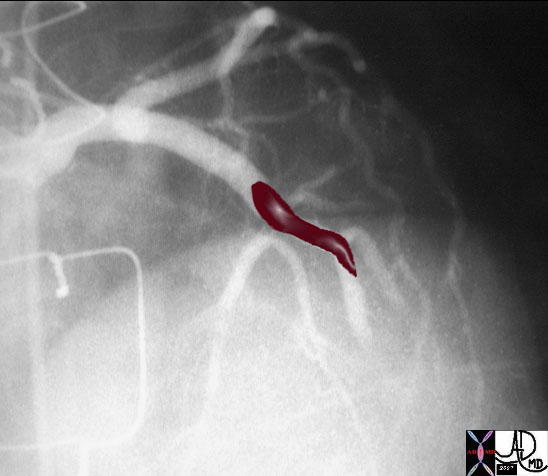
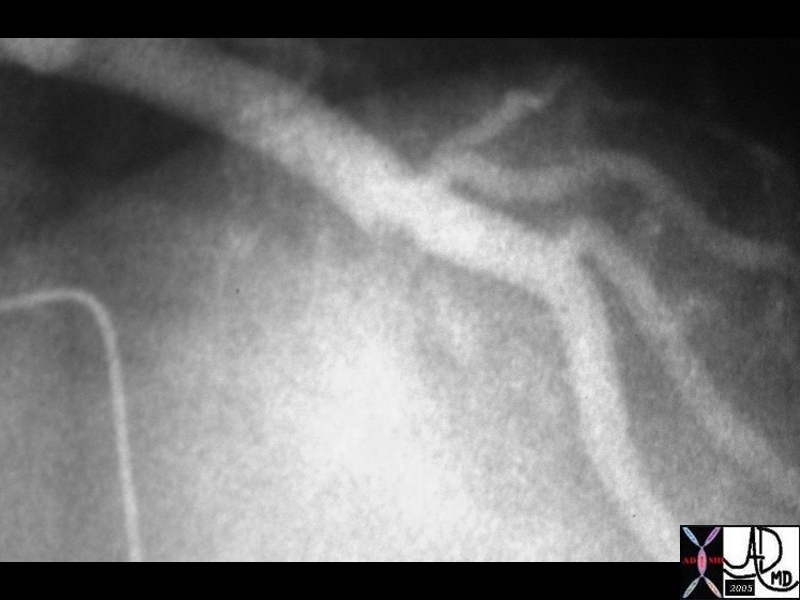
Thrombus in LAD then Thrombolysed |
|
| The first image on the left shows a cned down LAO projection if the LAD in a patient with acute thrombosis of the left anterior descending artery. In the second image the thrombus in the artery is overlaid in maroon. Following thrombolysis *third image minimal irregularity of the endothelium is seen. This may be residual thrombus or the site of a plaque rupture
16950 16950b02 16956 cardiac heart coronary artery LCA thrombus acute MI Courtesy Ashley Davidoff MD |
Atypical characteristics of the pain make the pain less likely to be secondary to myocardial ischemia or injury. Per the AHA/ACC guidelines, the pain is considered atypical if it is pleuritic in nature, if the primary or sole discomfort of pain is in the middle or lower abdominal region, if it can be localized with one finger, if it is reproduced with movement or palpation of the chest wall or arms, if it persists for hours or if it very brief and lasts seconds. An atypical presentation of pain makes cardiac ischemia less likely, however not impossible as the cause of pain. Certain groups of patients such as women, diabetic and elderly persons notoriously present with atypical manifestation of myocardial ischemia.
Pericarditis
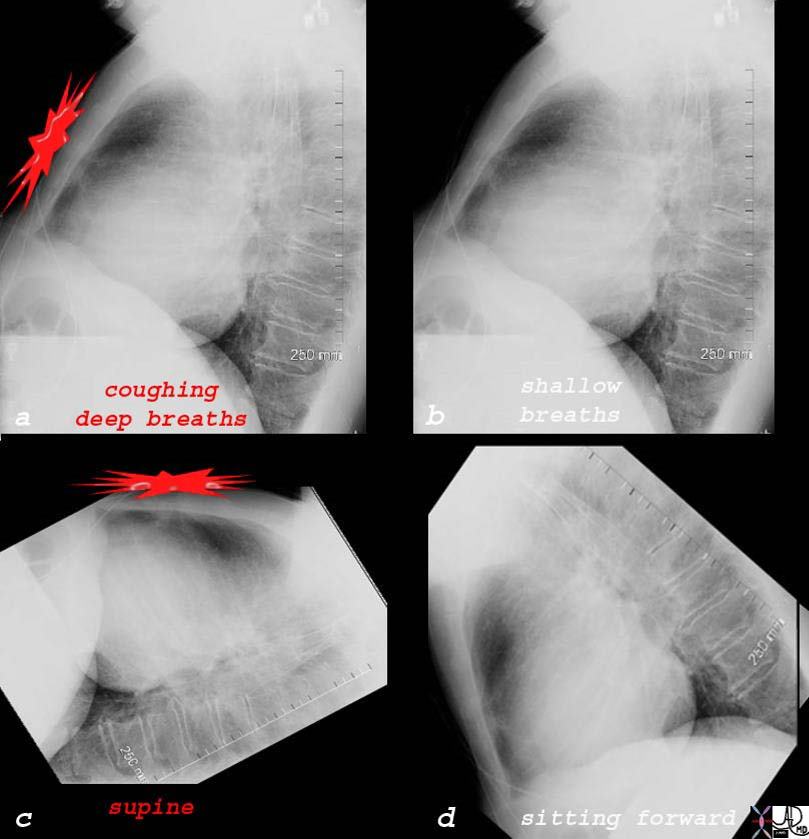
The pain of acute pericarditis can also be quite typical. Characteristically the pain tends to be aggravated by movement . It is usually central, pleuritic chest pain that, as a result of the pathway of the phrenic nerves, can radiate to one or both trapezius ridges. The pain may be aggravated by breathing simulating pleuritic pain or when the patient lies down. Pain may worsen when patients lie down and may improve when they sit up and lean forward.
 Aggravating and Relieving Characteristics of Pain from Pericarditis Aggravating and Relieving Characteristics of Pain from Pericarditis |
| The most characteristic feature of the pain of pericarditis is that it is relieved by sitting up or forward. Image a shows the characteristic sharp pain occurring in the precordium, as being intense and pleuritic in nature aggravated by coughing and deep breathing but relieved by sitting up, and shallow breathing (b). The pain is also aggravated by lying down, (c) but is relieved by sitting forward (d)
76031c01d02 chest heart pericardium pain aggravated by coughing and deep breathing relieved by shallow breathing and sitting forward acute pericarditis pericardial effusion lateral chest X-ray plain X-ray Courtesy Ashley Davidoff MD |
Pericarditis is an inflammatory or infectious disorder of the pericardium and has a multitude of causes. It is commonly encountered in patients inflicted with autoimmune diseases such as rheumatoid arthritis or lupus, patients with uremia and patients who have undergone cardiac surgery. Pericarditis may also result from a viral, bacterial or fungal infection.
Patients presenting with bacterial pericarditis tend to be very sick and usually present with fever and sepsis rather than isolated chest pain. Myocardial ischemia or infarction can result in inflammation of the pericardium either acutely or a few weeks after the acute event. Dressler’s syndrome is a specific immune syndrome consisting of fever and pericarditis occurring weeks after a myocardial infarction. The incidence of ischemia or infarct related pericarditis has declined since the advent of early coronary revascularization and the use of thrombolytics.
Acute pericarditis results in a serositis so that the inflammed pericardium presents with a somatic pain, and also exudes fluid into the pericardial space.
Acute pericarditis can be complicated by pericardial tamponade if there is a rapid accumulation of pericardial fluid.
The clinical presentation includes central, pleuritic chest pain described above. On auscultation of the heart, a monophasic, diphasic or triphasic pericardial rub can be appreciated. Pericardial rubs are highly specific for pericarditis however require careful or skillful auscultation to be picked up. Their low sensitivity is also due to their fleeting or intermittent nature.
The diagnosis is suspected by the classical clinical presentation, and larger pericardial effusions may cause decrease EKG voltages. However the diagnosis is best confirmed with echocardiography
 Large Pericardial Effusion – Echocardiogram Large Pericardial Effusion – Echocardiogram |
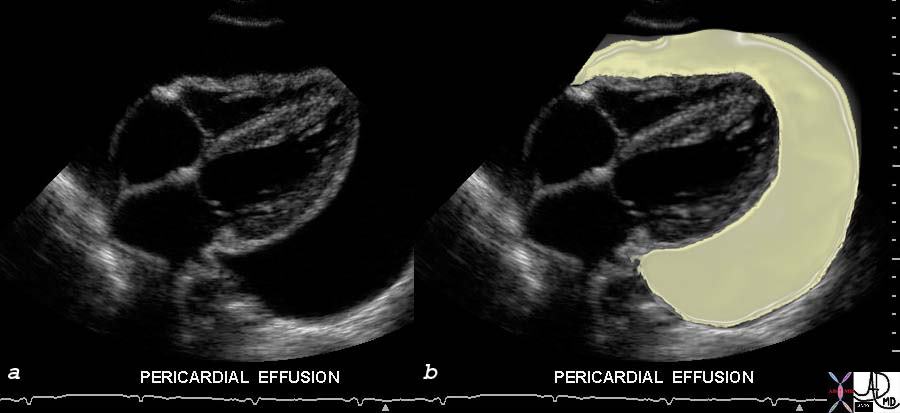
| The study of choice for the patient with pericarditis is echocardiography, since both the pericardium and myocardium can be evaluated. It is not uncommon for there to be an associated myocarditis that requires evaluation and echo can evaluate both issues. When the pericardial effusion becomes large it sometimes relieves the pain but it brings other issues as the potentialfor tamponade. This is also assessed using the echo combined with new clinical symptoms of cardiorespiratory difficulty.
33140c01 This gray scale echo of the heart showing a 4 chamber view, and demonstrating a large collection of fluid around the heart, characteristic of a pericardial effusion. Courtesy Philips Medical Systems 33140 code cardiac heart echo pericardium effusion imaging cardiac echo overlay Davidoff MD |
Lateral Chest Examination Showing Pericardial Effusion |
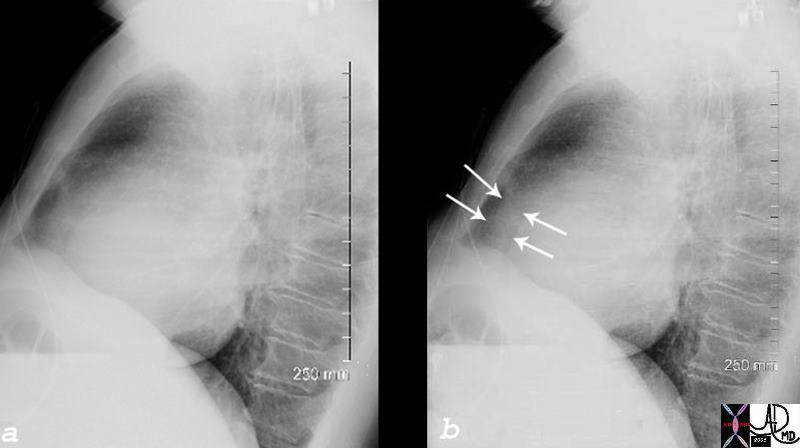
| The chest X-ray is not a sensitive test foe pericardial effusion but since it may be the first imaging test in the patient with chest pain it is important to recognize pericardial effusion as seen on the lateral examination (arrows). On the frontal examination the shape of the cardiac silhouette is said to look like a water bottle.
76031c01d04 chest heart pericardium aggravated by coughing and deep acute pericarditis pericardial effusion lateral chest X-ray plain X-ray Courtesy Ashley Davidoff MD |

Acute Pericarditis |
| Since CT scan is often used in the work up of chest pain it may be the study which in fact confirms the clinical supicions or the radiological suspicions. The chest X-ray of this patient shows a waterbottle shape on the frontal CXR, the pericardial collection on the lateral examination, (b – same patient as noted in the prior image reflected by the arrows) and the pericardial effusion on the CT examination (gray fluid around the heart in c and d).
76031c01d heart cardiac pericardium pericardial effusion enlarged fluid between two fat layers sandwich sign visceral pericardium parietal pericardium epicardial fat pericardial fat plain film CXR plain X-ray Courtesy Rebecca Schwartz |
Treatment includes anti-inflammatory drugs such as aspirin, NSAID or prednisone. Aspirin is effective; however the mostly utilized treatment for pericarditis is ibuprofen. It can be combined with colchicine that can help prevent recurrent episodes of pericarditis. The combination therapy should last 7 to 14 days then tapered over a week or two to prevent recurrence. Oral prednisone is used in patients with severe pericarditis and who do not respond to NSAIDs.
Aortic dissection
Aortic dissection is a sudden catastrophic disruption of the aortic wall caused by a shearing tear of the intima, and seconday involvement of the media by the advancing dissection and hematoma. The event characterised by a splitting of the arterial wall along the the longitudinal plane of the aorta.
The pain of aortic dissection is dramatic. It is classically hyperacute, sudden, severe, lancinating, excruciating, tearing, stabbing, throbbing reaching its maximum intensity at the moment of onset. On the other hand, “nothing is always” and some patients may present with minimal or no symptoms. The duration of the pain is not measured in minutes and may simulate the pain of myocardial infarction. The pain may be felt in the anterior chest, the neck, and or the back sometimes reflecting the location of the dissection with ascending dissections noted with anterior chest pain, arch dissections with neck pain and descending thoracic dissections noted with interscapular or back pain. Since dissections may involve the coronary arteries, and more commonly the right, myocardial ischemic pain may be present as well.
It is historically interesting to note that in 1910 William Osler recognized that “. . . spontaneous tear of the arterial coats is associated with atrocious pain, with symptoms, indeed, in the case of the aorta of angina pectoris and many instances have been mistaken for it”
The pain is caused by the stretching of the aortic wall, and hence its potential to have a throbbing character. It is not aggravated by position or body movement, nor relieved other than by analgesia, tincture of time, or repair.
The impending sense of doom originally described as “angor animi” literally means anguish of the soul may accompany the pain. This sensation sometimes accompanies other life threatening situations when there is massive outpouring of catecholamines, such as myocardial infarction and pulmonary embolism.
|
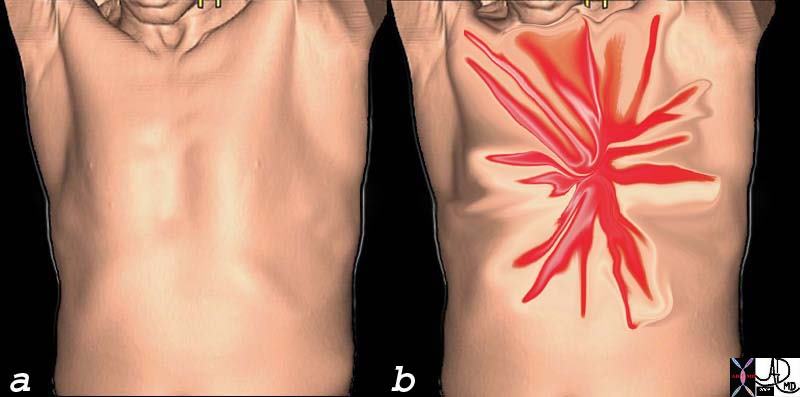
Acute Severe Lancinating, Shearing, Chest Pain of Acute Aortic Syndrome |
| This image is intended to reflect the severe (bright red) lancinating, sharp, thunderbolt like character (spiculated shape) of the chest pain that the patient with acute dissection may experience. One moment the patient is healthy without symptoms (a) and the next, there is catastrophic pain that reaches maximum intensity at the time of onset. (b) This is one of the pain syndromes in medicine one fears. It represents the one of the most severe forms of chest pain one can experience.
71197c10c chest pain character shearing sharp lancinating acute aortic syndrome aortic dissection penetrating ulcer acute aortic hematoma ruptured aorta ruptured dissection CTscan davidoff Art Courtesy Ashley Davidoff MD 49640c06 |

Lancinating Shearing Back Pain of Acute Aortic Syndrome |
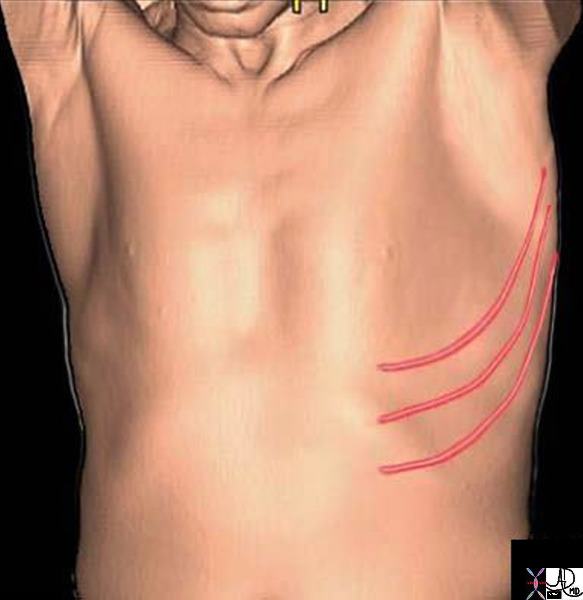
| The pain of dissection may be felt either in the front of the chest and or the back. Either way the pain can have similar characteristics – ie sharp, thunderbolt like, severe, and rapidly and almost instantaneously reaching maximum intensity coincident with the onset.
but can 49640c06 chest pain character shearing sharp lancinating acute aortic syndrome aortic dissection penetrating ulcer acute aortic hematoma ruptured aorta ruptured dissection CTscan Courtesy Ashley Davidoff MD |
Typically, aortic dissection occurs in patients with uncontrolled hypertension, pregnancy, atherosclerosis and diseases such as Ehlers-Danlos and Marfan. Asymmetric blood pressure or pulses or a new diastolic murmur due to aortic regurgitation may be appreciated on the examination of the patient. Aortic dissection represents a medical emergency.
Clinically the pain syndrome may be classical and the finding of unequal pressures or the association of complications such as stroke, Horners syndrome hoarseness, new onset aortic reurgitation or pericardial hemorrhage may help make the diagnosis. The study of choice to confirm the diagnosis and assess severity is however CTscan both without and with contrast, which is able to cofirm the diagnosis and evaluate the extent of the disease
The treatment depends on the extent of the dissection. Patients with an ascending aortic dissection require urgent surgery while patients with descending aortic dissection are managed medically. Such patients require optimal control of their blood pressure to limit the extent of the dissection.
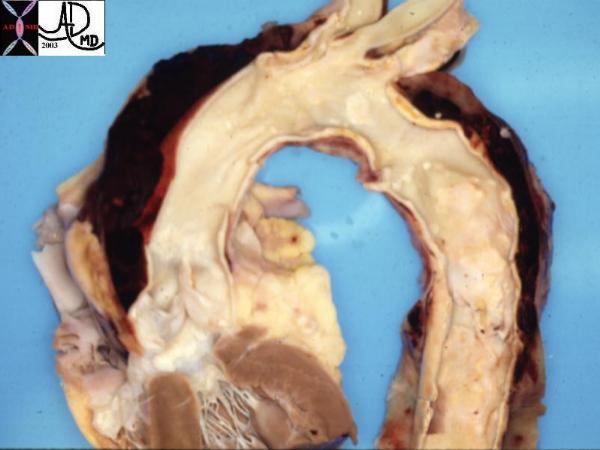
Fatal Acute Dissection |
| This pathological specimen shows an aortic dissection starting at the root of the aorta and extending across the arch and into the descending portion. The false lumen is filled with clotted blood.
Courtesy Henri Cuenoud MD 13421 code CVS thorax AO aorta dissection grosspathology |
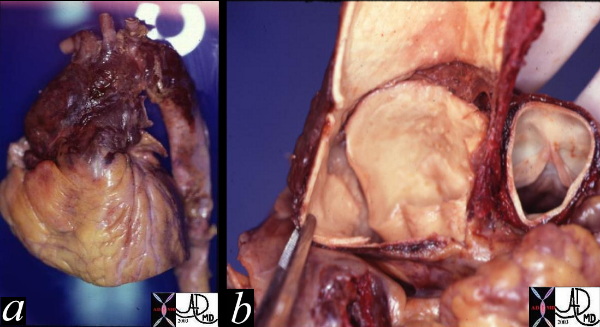
Rupture |
| These two pathological specimens show a ruptured dissection isolated to the ascending aorta. The external view (a) shows hemorrhagic change surrounding the ascending aorta with blood tracking into and through the adventitia. Image b, shows the internal intimal tear which in this case is almost circumferential. The dissection only involved the ascending aorta and it was therefore classified as type II in the deBakey system and type A in the Stanford system. Courtesy Henri Cuenoud MD. 13413c code CVS aorta ascending thorax dissection rupture grosspathology |
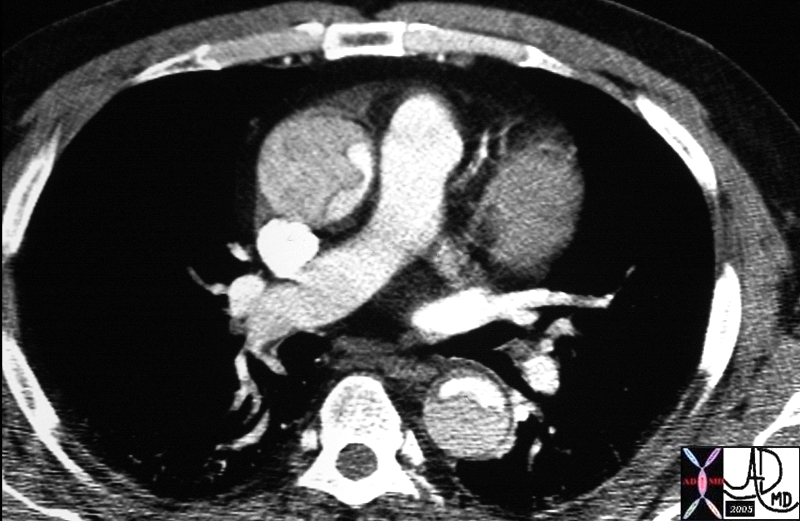
Type A Dissection |
| The CT image shows a dissection in the ascending aorta. The lumen consists of the smaller true lumen (with white contrast) and the false lumen (larger with grayer density) The involvement of the ascending aorta make s it a type A dissection and therefore treatment requires surgical repair. In this patient however the dissection extended to the descending aorta as well. Either way a type A dissection requires surgery.
20448 descending aorta ascending aorta fx dissection fx crescent dx aortic dissection type A CTscan Courtesy Ashley Davidoff MD DB |
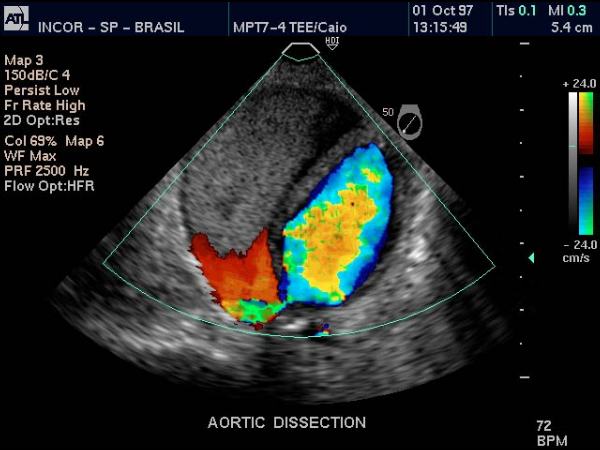
Desceding Thoracic Dissection shown by Color Flow Transesophageal Echcardiography |
| The transesophageal echo using Doppler US of the descending thoracic aorta shows flow in the true lumen (color) and no flow in the thrombosed lumen (gray echoes) in this patient with aortic dissection.
Courtesy Philips Medical Systems 33166 |
Acute Aortic Syndrome
Acute aortic syndrome” (AAS) is a complication of atherosclerotic disease of the aorta that is charcaterized by a classical clinical presentation of sudden acute searing pain in the chest or back, usually in an hypertensive patient. Since the pathogenesis of this disease results in acute distension of the aortic wall its pain characteristics simulate acute aortic dissection. Hence the same dramatic pain characteristics that occur in dissection apply to acute aortic syndrome, characterized by a sudden acute, severe, shearng or lancinating, pain that reaches maximum intensity at onset. Similarly though as well, the symptoms may be minimal or absent.
The clinical features and pathology of the two entities can be quite different. Whereas dissection is usually in a younger age group, acute aortic syndrome is seen in the older atherosclerotic age group and is more commonly associated with hypertension. Classic aortic dissection is characterized by the presence of intimal tear that usually progresssses to the media and then rapidly dissects for quite a distance (sometimes the entire aorta) and will usually have a reentrance site. Intramural hematoma is characterised by the presence of severe atherosclerotic plaque, with acute hemorrhage into the aortic media which may remain as a hematoma in the media or may progress to a dissection. The dissection though is usually limited because the atherosclerois and inflammatory changes and fibrosis present in the wall prevent s an easy route for progression. The rentrance of the dissection in AAS is usually absent and hence thrombosis of the focal dissection results.
Searing Chest or Back Pain of Acute Aortic Syndrome |
| 49640c06 chest pain character shearing sharp lancinating acute aortic syndrome aortic dissection penetrating ulcer acute aortic hematoma ruptured aorta ruptured dissection CTscan Courtesy Ashley Davidoff MD |
The cause of AAS is an acute mural hematoma. This may result from a hematoma into a plaque, into a penetrating ulcer, or a hemattoma in a focal dissection. The space occupation and sudden distension associated with the disease process by one of these disorders results in the classical pain syndrome. The disorders are best diagnosed by using a combination of non-contrast CT combined with a contrast enhancing CT.
The hematoma in the wall may be complicated by a classicial dissection , where the tear in the wall extends along the longitudianl plain. Aortic rupture can occur as well.
 Pathogenesis of Penetrating Diseases of the Aorta and Acute Aortic Syndrome Pathogenesis of Penetrating Diseases of the Aorta and Acute Aortic Syndrome |
| The lumen of the aorta with blood is demonsrated in red. The intima of the wall is the thin light pink layer just under the red lumenal layer. The media or elastic layer is in teal, while the outer layer is a light yellow color (a)
This diagram illustrates the progression from a ulcerated plaque (a), to a mural hematoma(b). The ulcer in c has penetrated the into the media itself and is called a pentrating ulcer with a mural hematoma. (c). In d, a smal focal dissection with flowing blood is seen, and this can either thrombose or progress to a full dissection(e) or penetrate through the wall and be contained (e) or eventually rupture into the mediastinum (f)
42409c01.800 aorta artery atherosclerosis atheroma acute aortic syndrome a aortic ulcer b = acute mural hematoma c = acute mural hematoma large d = focal dissection e penetrating ulcer f rupture histology histopathology Davidoff art pathogenesis Courtesy Ashley Davidoff MD |
Treatment is based on the size position and nature of the lesion, as well as comorbid conditions, and thus would be either surgical or medical.

Penetrating Ulcer |
| The CTscan through the upper chest shows ulcerations in the aorta (bright red) with a cap (maroon) overlying the larger ulcer. In acute aortic syndrome it is the hemorrhagic rupture of the plaque and the distension of the aortic wall that causes the pain.
48363c01 descending thoracic aorta fx aortic ulcer fx atherosclerosis atheroma fx penetrating ulcer CTscan Courtesy Ashley Davidoff MD |
Pulmonary embolus
The pain of pulmonary embolism is also fairly dramatic but is most commonly pleuritic in nature meaning it is somatic, sharp, aggravated by deep inspiration and coughing and relieved somewhat at expiration. It results from pleural involvement from a distal pulmonary infarction. However, patients with massive pulmonary emboli involving the larger and central vessels can present with substernal chest pain as a result of vessel distension. Patients with massive pulmonary emboli may also present with respiratory distress, hypotension and failure of the right ventricle secondary to a sudden increase in the right ventricle’s afterload. The impending sense of doom originally described as “angor animi” (anguish of the soul as described above) may accompany the pain of pulmonary embolus particularly if the pulmonary embolus is large and or there is a massive outpouring of catecholamines.
|
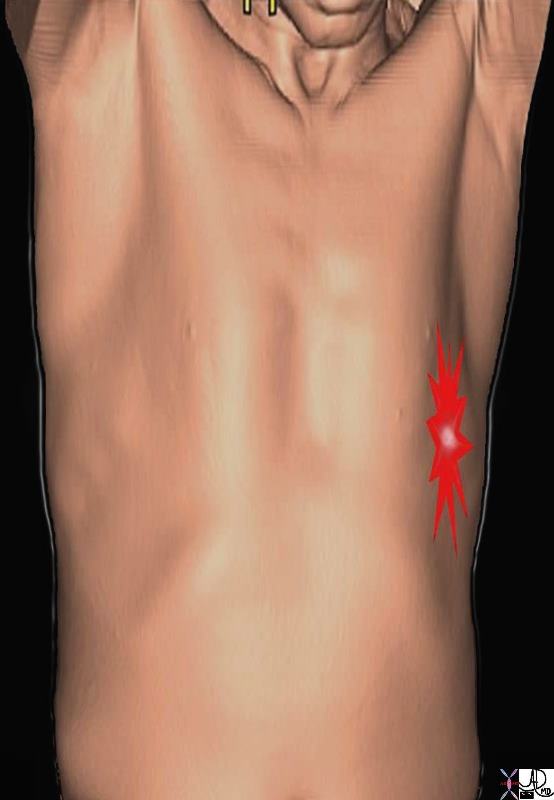
Pleuritic Chest Pain |
| The pleuritic pain demonstrated on the right side of this patient is characterized by focal intense (bright red) and sharp pain that is aggravated by deep breaths and by coughing. The location corresponds to the disease and to the images described below.
71197b03p chest lung pleura pleuritic pain PE pulmonary Embolus pneumonia pleurisy aggrrvated by deep inspiration coughing rib fracture pleuritic pain pleurisy CTscan 3D Courtesy Ashley Davidoff MD |
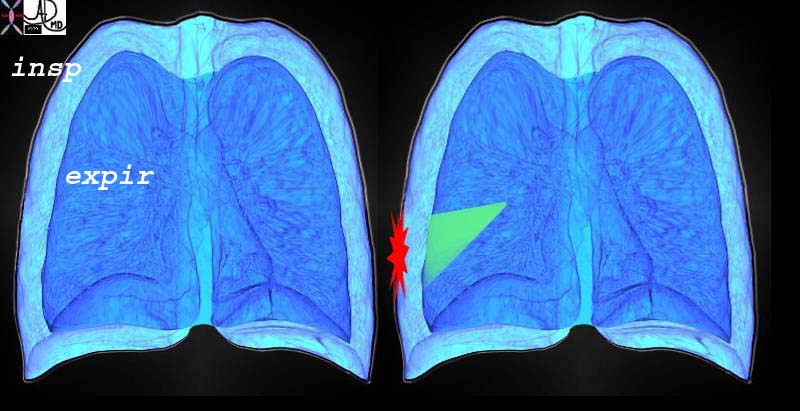
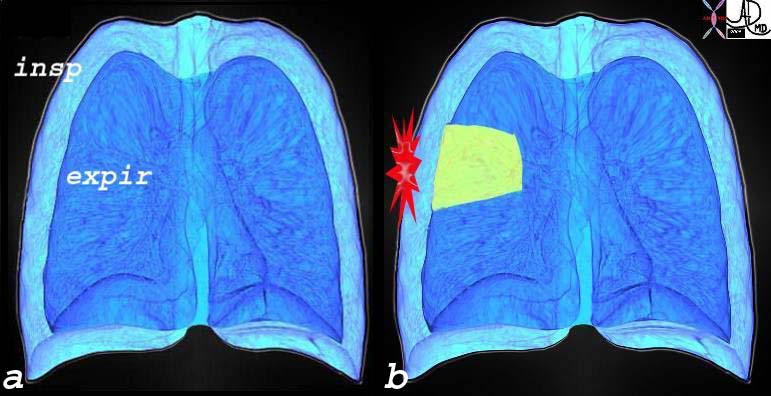
| Sharp Intense Pleuritic Pain on Inspiration Due to Pulmonary Embolus and Pulmonary Infarction |
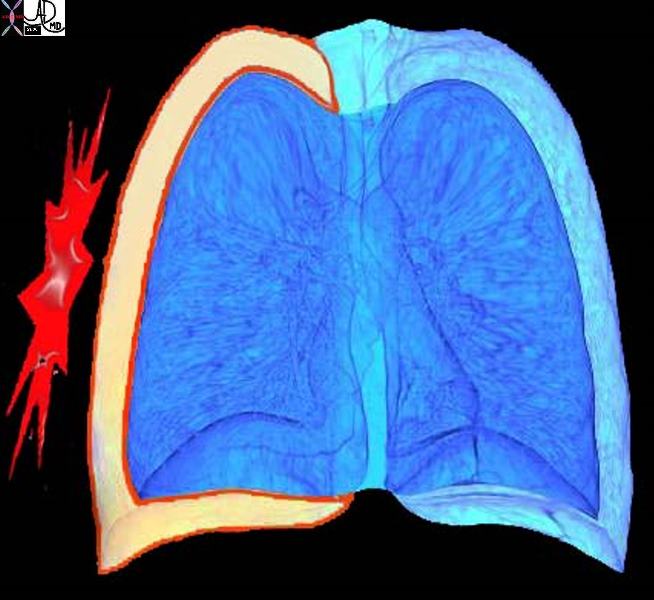
| This diagram re-enforces the concept of the pleuritic pain being related to respiratory movements and is focal and overlying the disease process. The outer part of the diagram represents the expanded lung of inspiration and the inner less voluminous lung represents the deflated lung of expiration. The green wedge represents the infarcted are of lung from the pulmonary embolus that abuts and involves the visceral and parietal pleura.
42540c02d lung inspiration expiration pain on inspiration focal severe pain pleuritic pain PE pulmonary embolus Davidoff art Courtesy Ashley Davidoff MD |
Pulmonary thromboembolism (PE) is a circulatory disorder of the pulmonary arteries characterized by embolic occlusion of one or more pulmonary arteries by bland thrombus.
Thrombotic PE is a leading cause of morbidity and mortality particularly among hospitalized patients. Most commonly the thrombi originate from the deep venous system of the lower extremities. Less common sources include pelvic veins, upper extremity veins, right heart chambers and in situ thrombosis. The causes for the deep venous thrombosis are crystallized by Virchows triad; venostasis , endothelial injury, and hypercoaguability. Patients immobilised for long periods (prolonged flights, prolonged bed rest) are predisposed because of stasis. Hypercoaguable states are sometimes inherited and and are sometimes part of malignant cconditions.
Acute thrombus in the veins is minimally adherent to the wall of the vessel and hence the propensity to embolize to the right heart and then to the lungs resulting in a variable degree of occlusion of the pulmonary circulation. In general the larger the thrombus load the greater the clinical cosequence.
Clinically the presentation ranges from asymtomatic to sudden death. A variety of pulmonary symptoms include dyspnea, pleuritic chest pain, tachypnea, cough, anxiety, while clinical examination may reveal non specific rales, tachycardia, or low grade fever.
The diagnosis is based on high clinical suspicion by the “clot concious” care giver, usually in the presence of lowered oxygen saturations and increase in the alveolar-arterial gradient . Visualization of thrombus in the pulmonary circulation using CT angiography is the gold standard however.
Treatment is usually by anticoagulation and in a selected few where the thrombus load is life threatening thrombolysis or thrombectomy are considered.
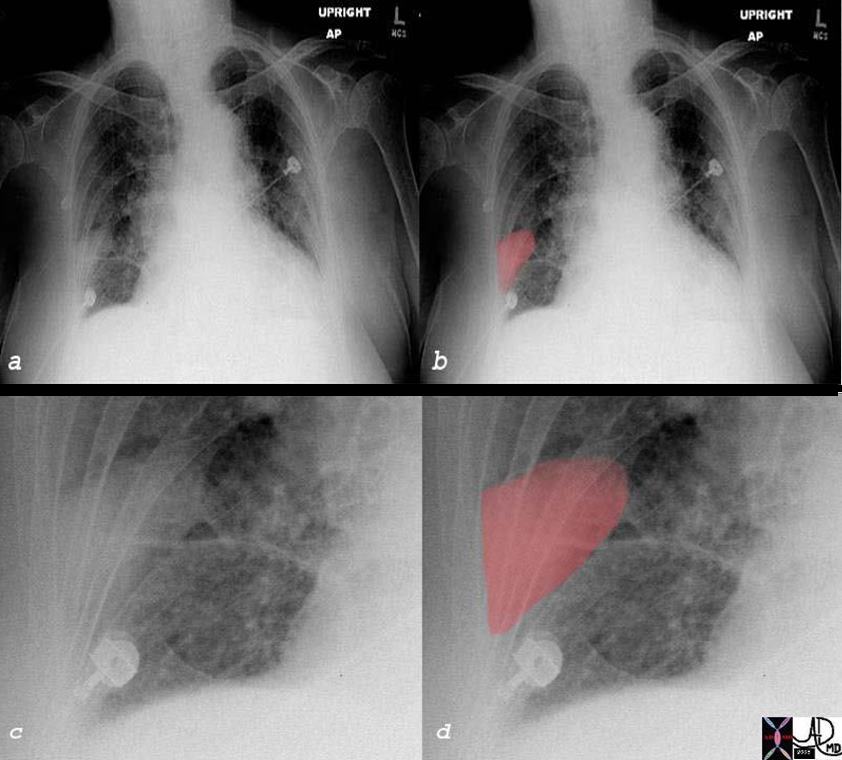
Wedge Shaped Defect on CXR Hamptons Hump – Pleural Based Infarction |
| The plain film of a patient with right sided pleuritic pain and hypoxemia is shown. Image a shows a vague wedged shaped defect in the right lower lobe (overlaid in red in b), enlarged in c and d. This wedge shaped peripheral based defect is known as Hampton’s hump, and is suggestive of a pulmonary infarction, and subsequently proven as seen on the images below. When a pulmonary embolus causes an infarction, it may be seen as a wedged shaped defect on the CXR. Since the pulmonary circulation of the lung is an end arterial circulation, the most distal portion of the segment of the lung and its pleura will be affected. The accompanying inflammatory process will involve the pleura and pleuritic pain ensues.
39693c01b chest lung lower lobe peripheral wedge shaped defect infiltrate Hampton’s hump PE pulmonary embolus infarction heart cardiac enlarged failure chf circulatory vascular CXR chest X-ray plain film imaging radiology Courtesy Ashley Davidoff MD |
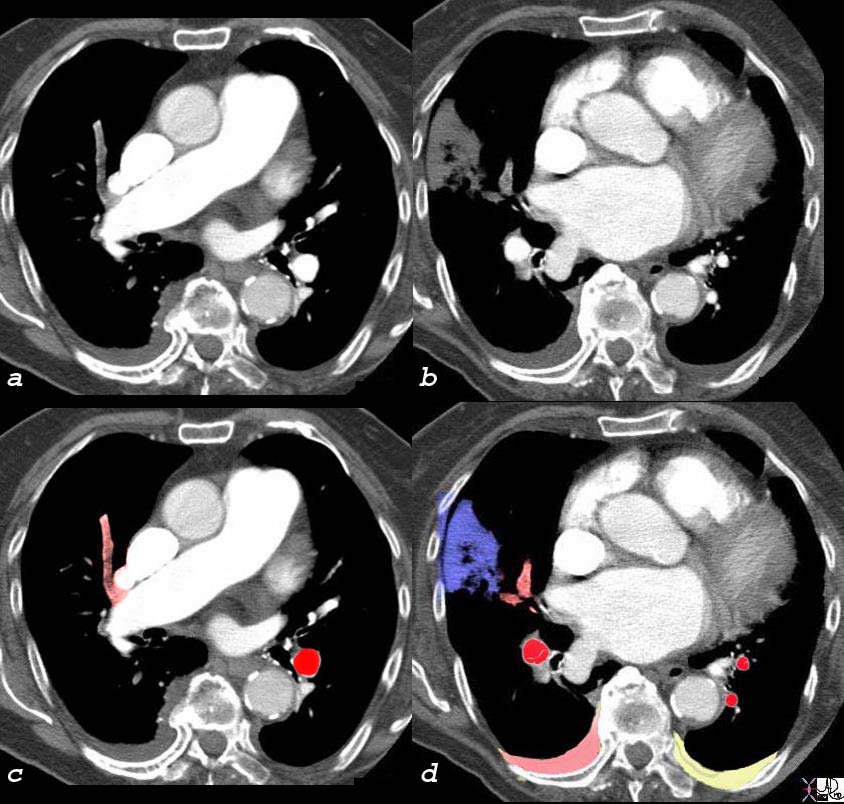
Occlussive Embolic Disease with Pulmonary Infarct |
| The CTscan of this patient shows an occlussive embolus (gray in a overlaid in pale red in c) as well as the branches of this vessel (gray in b and overlaid in pale red in d) resulting in a peripheral pleural based infarction (gray in b and overlaid in blue in d). There are bilateral effusions with right effusion (pink overlay) likely to be hemorrhagic and the left effusion likely to be transudative. Pulmonary infarction as seen in this case is not common since the lung receives oxygen directly from the alveoli, as well as from the bronchial arterial circulation. However in this patient, there was associated congestive heart failure and perfusion and ventilation were rduced at base line. When one adds insult to injury with a PE, compensatory mechanisms are not available and infarction ensues.
39693c05b chest lung lower lobe peripheral wedge shaped defect infiltrate Hampton’s hump PE pulmonary embolus infarction heart cardiac enlarged failure chf bilateral pleural effusions hemorrhagic pleural effusion inferred circulatory LAE left atrial enlargement vascular CTscan imaging radiology Courtesy Ashley Davidoff MD |

| Occlussive Embolic Disease with Pulmonary Infarct
Wedge Shaped Peripheral and Pleural Based |
| This is a post mortem specimen of a lung in a patient who had primary lung carcinoma with metastatic liver disease, portal vein thrombosis, a small pulmonary embolus (3) and a hemorrhagic pulmonary infarct in the LUL. Note the intimate relationship of the infarct to the pleural surface.
Courtesy Ashley Davidoff MD. 32190c code lungs pulmonary artery thrombosis embolus PE infarction hemorrhage hemorrhagic wedge shaped grosspathology a87-462 Hamptons hump |
Pneumonia
Patients with pneumonia can also present with chest pain, classicilly due to involvement of the pleural surface with the inflammatory process. Thus the pain would be similar to that described above with pleuritic PE pain, somatic and sharp, aggravated by deep inspiration and coughing and lessened by shallow breathing. Patients usually present with shortness of breath, a productive cough and fever as well.
Sharp Intense Pleuritic Pain on Inspiration Due to Peripheral Based Pneumonia |
| The pleuritic pain of pulmonary embolus, pneumonia or pleurisy is not distinct in itself, but the associated findings relating to the specific disease will help differentiate the variety of causes of pleuritic chest pain.
In this instance a periphral based pneumonia abuts the pleural surface and parapneumonic pleural inflammation involves both the visceral pleura and the parietal pleura. When the lung moves with respiration the rubbing of inflammed structures and particulalrly the pleura brings about the sharp focal pleuritic pain localized over the pneumonia. 42540c02a01 lung inspiration expiration pain on inspiration focal severe pain pleuritic pain PE pulmonary embolus Davidoff art Courtesy Ashley Davidoff MD |
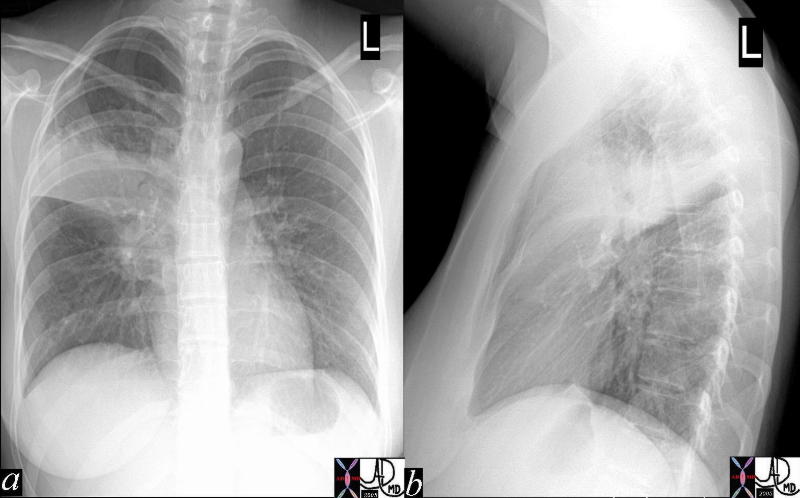
Right Upper Lobe Pneumonia |
| The AP and lateral CXR shows a right upper lobe pneumonia actually localized to the right upper lobe on the PA view (a) while on the lateral view it appears that the posterior segment of the right upper lobe is involved. In this patient the pleuritic pain may be felt in the back.
41800c Courtesy Ashley Davidoff MD medical students code chest infiltrate lung pneumonia right upper lobe RUL |
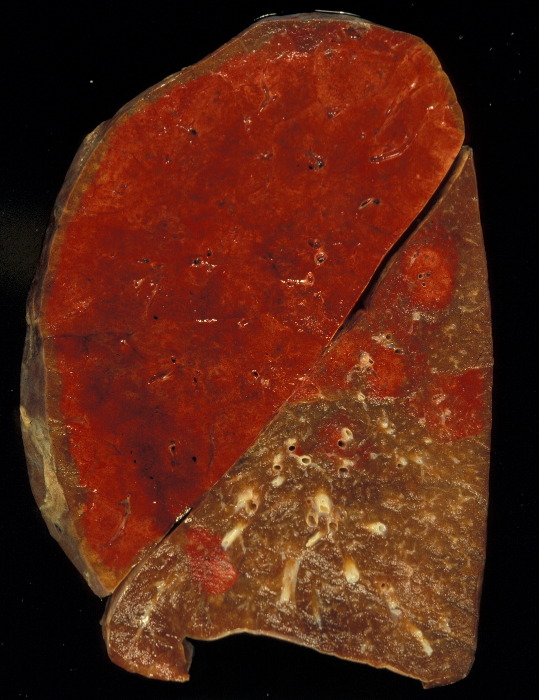
| Hemorrhagic Pneumonia |
| The gross pathology specimen shows a hemorrhagic lobar pneumonia (red hepatisation) in the left upper lobe with patchy subsegmental bronchopneumonic disease in the lower lobe. The relationship to the surface pleura may result in pleuritic pain.
Courtesy Jeffrey Pierce and Ashley Davidoff MD 32320 |
An infection of the trachea or bronchi, tracheobronchitis, may present with sternal chest pain in a patient. The patient may also experience some discomfort in breathing and a cough that can worsen the pain.
Pneumothorax
Accumulation of air in the pleural space leading to collapse of the underlying lung can occur spontaneously in tall and slim young adults or in patients with history of emphysema. Such patients usually present with an acute onset of unilateral pleuritic pain that may be associated with dyspnea. Depending on the size of the pneumothorax, it can be managed conservatively by observation or by evacuation of the air through placement of a chest tube.
  Tall ThinYoung – Spontaneous Pneumothorax with Mediastinal Shift Tall ThinYoung – Spontaneous Pneumothorax with Mediastinal Shift |
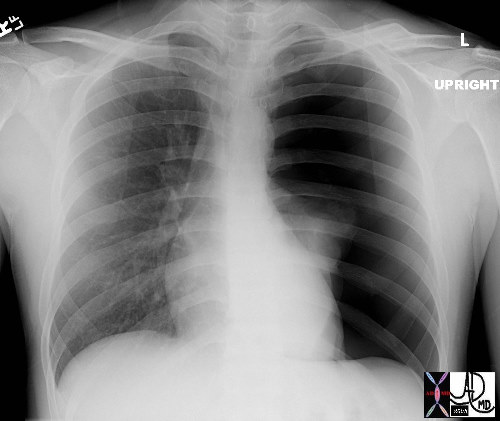
| This is the type of CXR that sends shivers down the spine. The overall blackness of the left chest cavity, in association with a nubbin of lung tissue in the ipsilateral hilum and rightward mediastinal shift is characteristic of a tension pneumothorax with total atelectasis of the left lung. Immediate and urgent decompression with a chest drain is indicated. One must also remeber that if a tall thin young patient presents with chest pain the diagnosis of dissecting aneurysm in a patient with Marfans syndrome has to be considered.
Courtesy Ashley Davidoff MD 42525 code lung pleura dx tension pneumothorax plain film CXR 5star medical students |
Pleurisy
Pleurisy is an inflammatory disorder of the pleura, having a multitude of causes but resulting in pleuritic pain, and pleural effusion.
The pain as stated is usually pleuritic but can be dull, burning sharp or stabbing. It is relatively acute in onset and can be quite severe (6-7/10). It is aggravated by coughing and deep breaths, and may be relieved by shallow breaths, and lying with the affected side down because chest wall motion is limited. Antiinflammatory medications may relieve the pain. Associated symptoms may include fever, cough, or productive cough.
The diagnosis is suspected clinically by the historyand dullness to percussion, whispering pectiriloqouy reflect an effusion. A pleural friction rub may be heard.
The chest X-ray helps making the diagnosis of a pleural effusion and in the appropriate clinical setting will confirm the clinical suspicion. Rib films if a fracture is suspected are indicated.
Treatment is directed to the cause but symptomatic treatment includes ibuprofen, indomethacin or naproxen.
Pleuritic Pain and Effusion – Pleurisy |
| The pleuritic pain is sharp, severe, and aggravated by deep breathing and coughing and relieved by shallow breathing and lying ipsilateral side down. The image on the right shows an overall increase in density of the right chest suggestive of a pleural effusion which is non specific and may accompany many of the diseases discussed.
42540c08 44665 pleural effusion chest lung pleura pleuritic pain pleurisy Davidoff Art Courtesy Ashley DAvidoff MD |
Pulmonary hypertension
Patients with pulmonary hypertension may be inflicted with chest pain that is thought to be secondary to underlying right ventricular hypertrophy and ischemia.
Pulmonary hypertension is a circulatory characterized by an abnormally high pressure in the pulmonary arteries. The diagnosis is defined as a systolic pressure that is greater than 30mmhg or a mean pressure that is greater than 20mmhg.
There are many causes for the disorder including, left heart failure, mitral valve disease, chronic lung disease, (cor pulmonale) and congenital left to right shunts. Patients with chronic thromboembolic disease may have hypertension and acute embolic disease may be associated with acute hypertension. When the cause is known it is called secondary hypertension. In many the cause is unknown in which case it is called primary pulmonary hypertension. In some some cases there is a genetic predisposition.
Clinically the entity results and manifests in shortnes of breath, coughing, wheezing, chest pain, fatigue, fainting, dizziness, light-headedness, and swelling in the legs. The diagnosis is confirmed by identifying an enlarged right ventricle, abnormally loud P2 sound, a systolic ejection murmur, and perhaps a pulmonary diastolic murmur, by electrocardiography which shows right ventricular hypertrophy. Echocardiography can not only evaluate right ventricular and right atrial size, but can accurately estimate the pulmonary arterial pressure if there is tricuspid regurgitation. While the CXR CTscan and MRI can evaluate pulmonary arterial size and right ventricular size, the most acurate evaluation of the entity is via cardiac cateterization which measures the pressures directly.
Treatment is directed to the cause when known, usually with medication, and oxygen. In patients with underlying mechanical causes such as left to right shunts a surgical option is possible if the fixed component of the hypertension is not excessive.
Pulmonary Hypertension – Scleroderma |
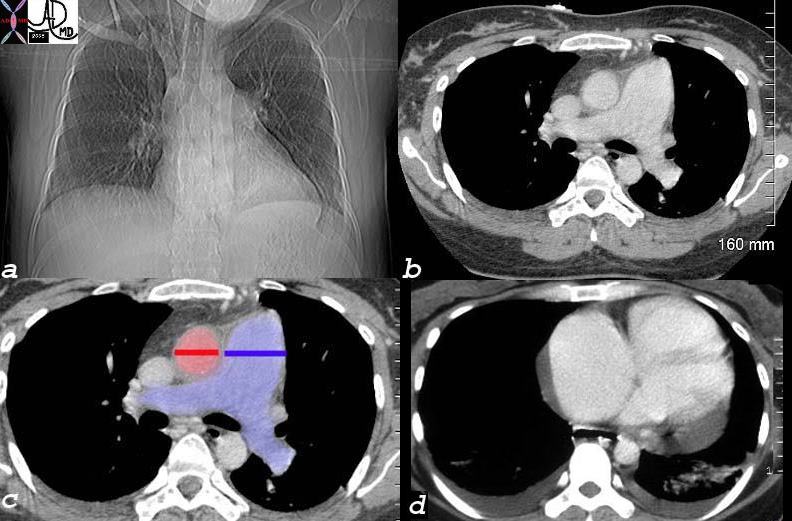
| This unfortunate 32 year old female with scleroderma has many causes for chest pain but the cause under discussion is a relatively uncommon cause for chest pain – pulmonary hypertension. This is best diagnosed with echocardiogram or cardiac catherization but in this CT the large pulmonary artery (blue – which should be the same size of the red aorta normally) is indicative of pulmonary hypertension. Her heart is enlarged (a) and she has a pericardial effusion, and bilateral pleural effusions (d) both of which can cause pain. In addition she has an enlarged patulous esophagus (seen as a black slit behind the heart (d) characteristic of scleroderma, and associated with reflux which is another cause for chest pain.
30464c12 32 female lungs pleura heart cardiac RA RV right ventricle right atrium pericardium esophagus ILD basal interstitial lung disease pericardial effusion pleural effusion cardiomegaly enlarged esophagus patulous esophagus gallbladder wall edema congestive cardiac failure RHF right heart failure rifht ventricular enlargement RVE RAE right atrial enlargement pulmonary hypertension cor pulmonale dx scleroderma Courtesy Ashley Davidoff MD |
Gastrointestinal causes of chest pain
Gastrointestinal pathologies are a leading cause of non cardiac chest pain. Gastroesophageal reflux can cause pain as a result of gastroepsphageal distension, inflammation, or spasm induced by the reflux. The pain therefore can have multiple clinical presentatiuons that range from discomfort, squeezing, pressure, dull pain, and burning pain to pain that mimics angina or myocardial infarction. Esophageal spasm for example may also respond to nitroglycerine which becomes clinically a challenging situation. Esophageal irritation by the highly acidic gastric secretions due to gastro-esophageal reflux can cause a burning retrosternal pain which characteristically is relieved by anatacids and proton pump inhibiotrs.
Dull Pain, Burning Sensation, and Angina-like symptoms GERD |
|
| GERD with or without esophagitis and spasm can often masquerade as cardiac pain varying from substernal discomfort, and pressure like symptoms, to substernal pain and burning (b) to discomfort that radiates to the neck and shoulder (c) but also is sometimes relieved by nitroglycerine. The pain however is not precipitated by excercise nor relieved by rest.
71197c06a 71197c05a substernal chest pain burning esophagus heart cardiac esophagitis reflux angina MI myocardial infarction subsernal chest pain CTscan 3D Courtesy Ashley Davidofff MD |
GERD is a common mechanical disorder of the lower esophageal sphincter that is caused by multiple factors including obesity, transient relaxation of the LES and hiatus hernia. It is exacerbated by the consumption of a lipid-rich meal, caffeine, mint and chocolate. An elevated abdominal pressure seen in gravid or obese patients can also lead to gastroesophageal reflux.
The reflux of acidic gastric contents onto the esophageal mucosa results in distension of the esophagus and inflammatory changes commonly complicated by erosive esophagitis. Such patients may also experience esophageal spasm that produces a squeezing retrosternal pain that can be difficult to clinically differentiate from a myocardial cause of pain it can also be relieved with nitrates.
Up to 15% of adults in Western society report symptoms monthly or weekly, while 7% report daily symptoms.
The diagnosis is probably best made clinically. The clinical presentation varies from the classic retrosternal burning sensation to chest pain, waterbrash (hypersalivation), and halitosis. It has been suggested that up to 60% of non-cardiac chest pain can be attributed to GERD. The absence of gastroesophageal reflux in a barium swallow does not exclude the diagnosis.
The mainstay of therapy for GERD remains the Proton Pump Inhibitors (PPI) and the H2 Blockers.
 Small Hiatus Hernia (a) and Large Amount of Reflux (b) Small Hiatus Hernia (a) and Large Amount of Reflux (b) |
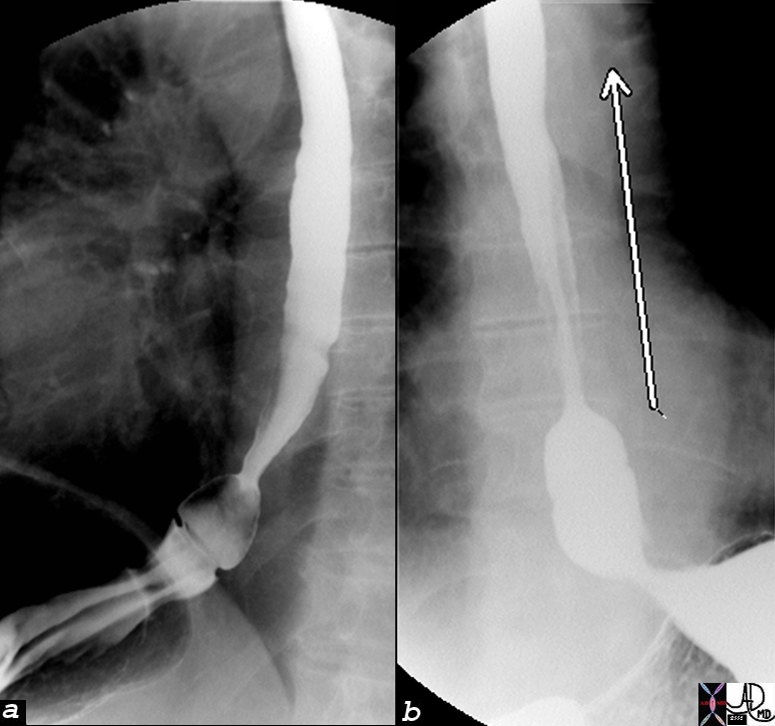
| The images are from a barium swallow showing a small puch like hiatus hernia above the diaphragm in a and gasrtresophageal reflux indicated by the arrow in b.
76171c01 esophagus GE junction gastroesophageal junction squamo-columnar junction z line epiphrenic ampulla gasrtric mucosa small hiatus hernia large amount of reflux to thoracic inlet double contrast barium swallow Courtesy Ashley Davidoff MD |
 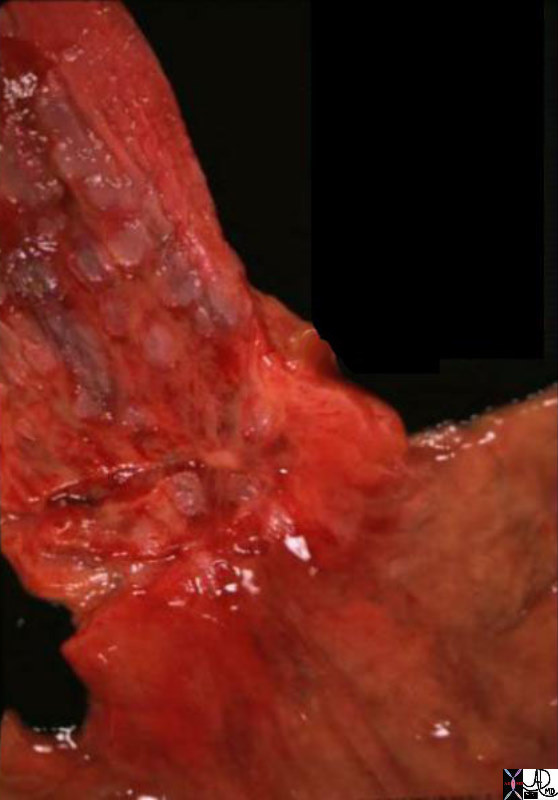
The Normal (left) and Abnormal (right) Red and Swollen GE junction – Reflux Esophagitis |
| The normal gastroesophageal reflux is marked in the image on the left (surgical specimen) by the transition from the white squamous lining of the esophagus to the salmon colored lining of the stomach. In the image on the right , a post mortem specimen) there is severe esophagitis and the normal white lining of the esophagus is replaced by inflammed red, indicating severe esophagitis.
01239b01.800 esophagus stomach GE junction gastroesophageaal junction inflammed inflammation GERD red swollen reflux esophagitis grosspathology Courtesy Ashley Davidoff MD |
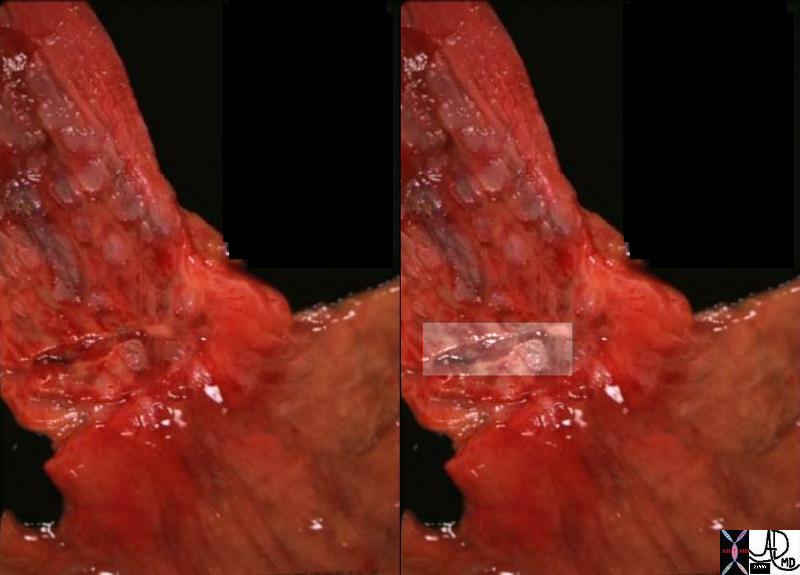
| Linear Ulcer in a Hyperemic Background of Diffuse Esophagitis |
| On closer inspection of the post mortem specimen, one can identify a linear ulcer of the esophagus, that is in fact painful in itself just to look at. It is overlaid in a cream rectangle on the right image.
01239c esophagus stomach GE junction gastroesophageaal junction inflammed inflammation GERD red swollen reflux esophagitis linear ulcer grosspathology Courtesy Ashley Davidoff MD |
| Pain Relieved by nitroglycerine- Unrelated to Excercise and Rest |
| The diagram illustrates a patient without pain (a) who develops substernal pain radiating to the neck and left shoulder. He takes nitroglycerine and the pain is relieved. (c) The pain was however not related to excercise and was not relieved by rest and lasted 10 minutes. Wht is the most likely cause of the pain? Sometimes esophageal spasm associated with GERD can respond to nitroglycerine and this is th most likely diagnosis. The patient however should undergo a stress test to ensure that he does not have ischemic heart disease.
71197c07c substernal chest pain burning esophagus heart cardiac esophagitis reflux substernal chest pain radiating to neck and left arm relieved by rest and sublingual nitroglycerine angina CTscan 3D Courtesy Ashley Davidofff MD |
 Nor Nor mal and Esophageal Spasm mal and Esophageal Spasm |
| The patient on the left image has a normal appearing single contrast barium swallow, but the patient on the right has a cokscrew esopohagus reminiscent of esophageal spasm. This appearance is also sen inthe aging esophagus and is called presbyesophagus and is usually asymptomatic.
39562b01.800 01232 esophagus normal anatomy single contrast barium swallow Courtesy Ashley Davidoff MD |
Chest Pain -Back Pain
The high back pain syndromes are included in this module because diseases in the chest can present with back/chest pain and they need to be differentiated from the abdominal causes of back pain. Thus aortic dissection, pneumonia, pleurisy and pulmonary embolism can localise to the back.
There are abdominal disorders that originate in subdiapgragmatic locations that can present with back pain including including acute and chronic pancreatitis, acute cholecystitis, splenic and liver diseases. Acute pancreatitis is quite distinct and usually presents with epigastric pain that may also go to the back. The most common cause is as a result of an alcoholic binge, and thus in the young patient there are some leads to follow. In the older patient gallstone pancreatitis could present as a diagnostic dilemna, but the issue is resolved once the serum amylase and lipase is evaluated. Chronic pancreatitis and pancreatic carcinoma may present with high back pain and these usually require CTscanning to establish the correct diagnosis.
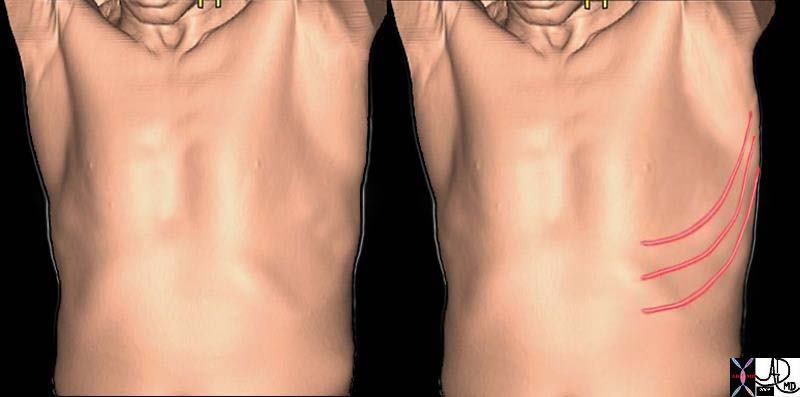
Acute cholecystitis usually presents with right upper quadrant pain but may also present as interscapular pain often with a band like distribution between the scapulae
 Band Like Interscapular Pain Band Like Interscapular Pain |
| The interscapular band like back pain is part of both lower chest and upper abdominal disease.
49640c03 chest back pain belt interscapular band like pancreas gallbladder retroperitoneum retroperitoneal structures CTscan Courtesy Ashley Davidoff MD 3D |
Acute pyelonephritis will present as a high backpain, will be unilateral and usually is exquisitely tender. The diisease is usually diagnosed with white cells in the urine and a history of cystitis. Renal colic may also present as high back pain, but the presence of hematuria and radiation (loin to groin) pattern when present, creates specificity for the diagnosis.
Skin
The pain of herpes zoster shingles is quite severe and can last a month. The onset is insidious and and is characterized s burning throbbing or stabbing. It is tender to the touch and may show a rash or vesicles along the affected dermatome. Usually only one dermatome is involved but it may involve 2 or 3 dermatomes. the thoracic dermatomes are most commonly involved. Associated finding include systemic symptoms of the the virus (20%) and parasthesias in the involved dermatome.
Dermatomal Pain |
| Pain that distributes along a dermatome is characteristic of Herpes Zoster (aka shingles) The dermatomes involved are usually thoracic and between one and 3 dermatomes are involved with burning and sometimes severe pain associated with a rash with vesicles.
71197c04 skin chest pain dermatome pain herpes anatomy CTscan 3D volume rendering Courtesy Ashley Davidoff MD |
Musculoskeletal causes :
Rib Fractures
Rib fractures are a source of incapacitating pain. The somatic nature, focal over the area of injury usually is caused by involvement of the underlying periosteum and pleura and hence the pain is pleuritic in nature, aggravated by deep breathing and coughing and relieved to some extent by shallow breathing. The most common cause is known traumatic incident, but fractures may occur with coughing spells, with little precipitating cause in the osteoporotic elderly, and as stress fractures in athletes (eg disc throwers) from excessive and repetitive forces.
The entity is most commonly diagnosed using plain X-rays and occasionally in the osteoporotic patient bone scan may be used to identify the cause of chest pain.

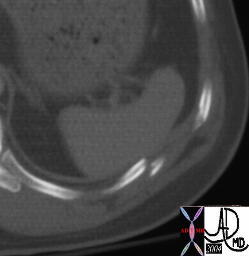
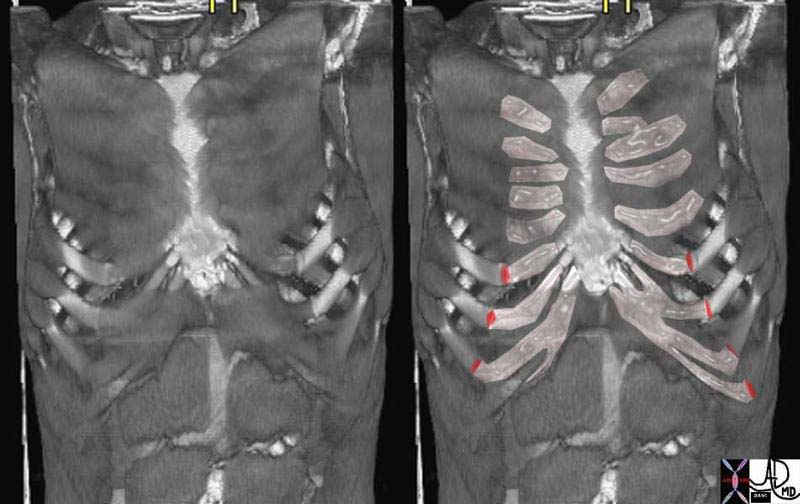
Rib Fractures |
| Multiple hot spots (black dots) are seen along multiple sequential posterior ribs on the right characteristic of multiple rib fractures. The involvement of multiple ribs and their close linear and contiguous spatial relationship make trauma much more likely than metastases.
r49688.800 bone heart uptake in ribs right posterior probably related to rib fractures. Finding of interest is the uptake in the heart which should not be seen with a bone scan and it indicates a recent myocrdial infarction NM radioisotope Courtesyt Alan Ashare MD |
| Dangerous Rib Fractures |
| This patient was discharged from the hospital with a normal spleen but with a rib fracture in close proximity to the spleen . He represented with splenic rupture probably caused by penetration of the spleen by the fracture fragment. Courtesy Ashley Davidoff MD 20805 spleen + fx normal + dx delayed rupture + imaging radiology CTscan rib fracture adjacent to the spleen trauma |
Costochondirits
Costochondiritis is due to the inflammation of the costochondral or costosternal joints and can cause anterior chest pain in young adults and elder patients. The pain is usually described as sharp and can be brief, intermittent or persistent and dull. The pain is usually well localized, involves more than one junction in most patients and can be pointed out by the patient with one digit. Sometimes the patient is not aware of the pain but minimal compression of the rib cage from the lateral force results in a characteristic localization of the pain at the costochodral junction. It is a benign cause of chest pain. Patients should be reassured prior to discharge.
Costochondritis |
| The location of the pain in patients with costochondritis is very characteristic in its location along the costochondral junctions as outlined in the above coronal 3D reconstruction of a CTscan (red)
71201c04.801 bone ribs costal cartilage costochondral junction costochondritis muscles intercostals serratus anterior pectoralis normal anatomy CTscan Courtesy Ashley Davidoff MD |
Other disorders of the ribs and sternum such as osteomyelitis and metastases are usually quite focal, somatic in character and not usually confused with acutely life threatening conditions.
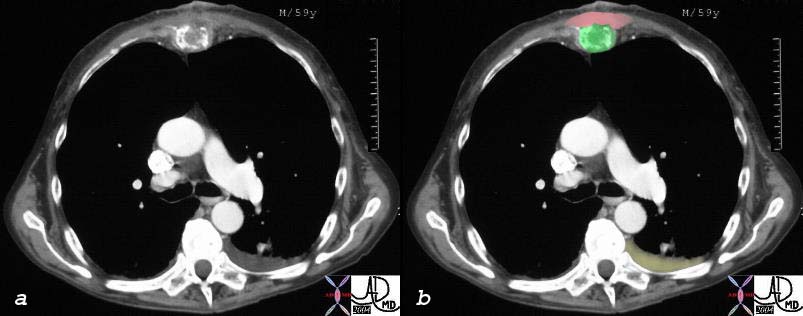
| Metastasis to the Sternum from Pancreatic Carcinoma |
| The sternum noted anteriorly in this axial CT section through the chest shows an expanded and destroyed sternum (green) with swelling in the soft tissues anterior to the sternum (pink). A left sided chest effusion (yellow is noted incidentally.
30101a01 Courtesy Ashley Davidoff MD bone sternum body fx expansile lytic mass dx metastasis pancreatic primary pancreas carcinoma neoplasm malignant growth tumor cancer CTscan |
Muscular Causes
Muscular aches and strains from excercises are quite common but usually there are known precipitating causes such as recent excercise. Myositis from viral disease is usually a dull pain involves other muscles and is associated by other systemic symptoms of the illness.
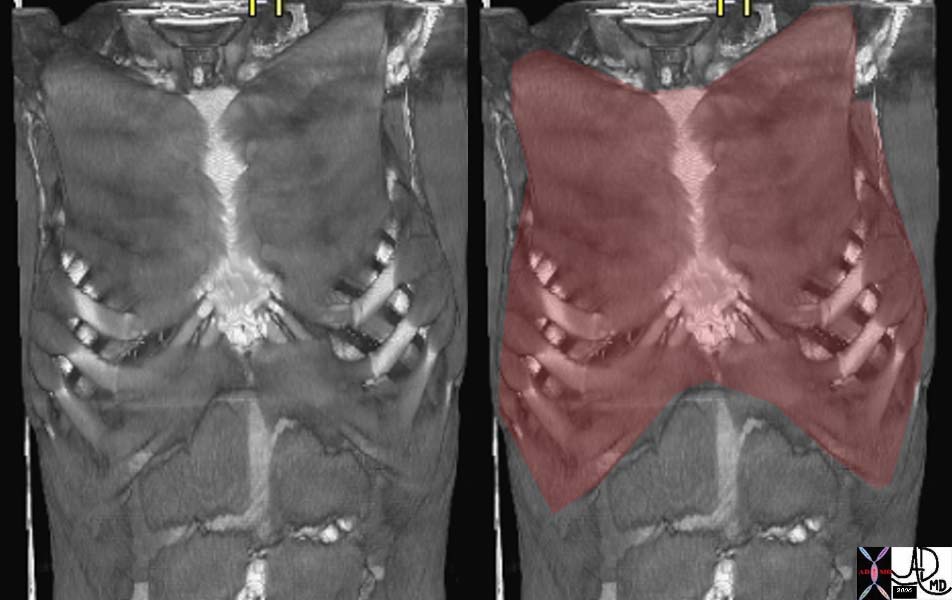
Muscles of the Anterior Chest Wall |
| The 3D image reconstructed from the raw CT data shows the musculature of the anterior chest wall and the recti of the abdominal muscles. There are many muscles in the anterior and posterior chest wall that could become inflammed or strained.
71201c05 muscles intercostals serratus anterior pectoralis normal anatomy CTscan Courtesy Ashley Davidoff MD |
There are some unusual causes of myositis including polymyositis and dermatomyositis which are also part of a systemic illness. Infected myositis secondary to osteomyelitis may also cause chest pain.
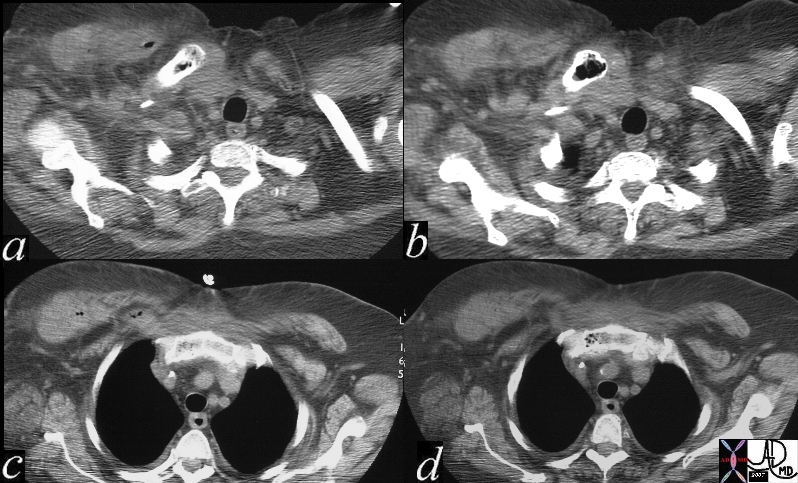
Myositis and Osteomyelitis |
| This unusual case of an osteomyelitis (air in clavicle and b) (air sternum image d) together with a swollen right sided pectoralis major that also contains air (a and c) was caused by clostridium welchii.
15759c01 bone clavicle sternum muscle pectoralis major sternoclavicular joint clavicular fx air fx swollen fx induration air bubbles dx clostridium welchii dx wet gangrene infection CTscan Davidoff MD 15754 15755 15758 15759 15759c01 |
Clinical approach
The initial approach to a patient with chest pain is directed towards two goals: to determine a diagnosis and to ensure the safety of the patient throughout the process. Therefore, it is crucial to first assess the patient for any sign of respiratory distress or cardiovascular compromise and stabilize the patient if needed. A focused history and physical examination should be pursued in the stable patient in the aim of screening for life threatening conditions such as an acute myocardial infarction, aortic dissection or massive pulmonary embolus. While obtaining the history, it is important to determine the manner of onset of the pain, its character, duration and any associated symptoms.
History
Precipitating factors
Chest pain due to myocardial ischemia or infarction is classically precipitated by physical exertion such as shoveling snow, meal consumption and cold weather. Also, any situation leading to tachycardia or increased myocardial oxygen demand in a patient with limited myocardial oxygen supply secondary to coronary atherosclerosis can lead to an imbalance between oxygen demand and supply and myocardial ischemia.
A recent history of an upper respiratory tract infection may predispose a patient to a bacterial pneumonia or to pericarditis.
Pulmonary embolus is usually seen in patients who lead a sedentary lifestyle, have recently undergone surgery, have recently traveled or who have an underlying malignancy. Patients on oral contraceptive pills are also at increased risk of developing deep venous thrombosis and pulmonary emboli. Other patients may be at increased risk of developing pulmonary emboli due to a hereditary thrombogenic state.
Patients experiencing chest pain due to underlying gastroesophageal reflux may experience their symptoms after consuming a large, rich meal or after lying flat soon after a meal. Also, an increase in abdominal pressure secondary to either obesity or to a gravid state can lead to gastroesophageal reflux.
Duration
An episode of myocardial ischemia may last between two minutes to twenty minutes and leads to infarction if it persists. If the pain lasts seconds or has persisted for days, a diagnosis other than myocardial ischemia or infarction should be entertained.
Chest pain that lasts seconds after movement is suggestive of costochondritis or another musculoskeletal cause. Chest pain secondary to pneumonia or pulmonary emboli may last days till the resolution of the underlying problem.
Onset
A sudden onset of chest pain is concerning for life-threatening conditions such as myocardial ischemia, infarction, aortic dissection or pulmonary emboli. Other more benign conditions may also present acutely such as a pneumothorax or a rib fracture. Chest pain secondary to gastroesophageal reflux is more gradual in onset.
Character
Patients experiencing myocardial ischemia or infarction usually describe their pain as a “pressure” or discomfort rather than frank pain. They may also place a clenched fist above the sternum or to the left side of their chest to better describe their symptom.
The severe lancinating pain of acute dissection is dramatic and mostly ummistakeable.
Thesense of impending doom caused by massive outpouring of catecholamines (“angor animi”) occurs with dissection, acute MI and pulmonary embolus.
Chest pain that is due to a pulmonary pathology such as pneumonia, pneumothorax or pulmonary infarction secondary to a pulmonary embolus is usually pleuritic in character.
Gastroesophageal reflux may cause a retrosternal burning sensation.
Situation
The pain of GERD and angina are usually substernal, while cardiac pain may also involve the neck, chin and arm. Pleuritic pain from pneumonia, rib fracture, PE, or pleurisy is focal andd depends on the location of the disease.
High back pain occurs with dissection, but also occurs with abdiminal organs iof the upper abdomen.
Myocardial infarction can occur at anytime but more episodes are encountered in the early morning hours
Severity
Pain of acute dissection is maximum at the onset and the patients feel like they have been hit by a bolt of lightening. Pain due to myocardial ischemia or infarction peaks in severity within minutes leading the patient to discontinue any activity that precipitated the pain and to seek medical advice.
Patients with pulmonary embolus can present with acute onset of severe and sharp pleuritic pain.
Patients with costochondritis may also experience severe, sharp pain that leads them to seek medical care and reassurance.
Aggravating factors
Myocardial ischemia or infarction is usually precipitated and aggravated by exertion, emotional stress or any situation or activity that can lead to increase myocardial oxygen demand.
Patients with pericarditis experience worsening of their pain with change in movement and by lying flat.
Coughing and deep inspiration aggravates pleuritic pain.
Relieving factors
Patients with myocardial ischemia may find relief with rest or administration of sublingual nitroglycerin.
Patients with esophagitis may have relief with antacids.
Patients with pericarditis may have relief by leaning forward.
Associated symptoms
Patients with myocardial ischemia or infarction can present with shortness of breath, diaphoresis, palpitations, nausea and even episodes of emesis.
Other than presenting with pleuritic chest pain, patients with pulmonary emboli may complain of hemoptysis, shortness of breath and palpitations. Patients with massive pulmonary emboli may experience dizziness and even syncope.
Patients with viral pericarditis, or myositis may have fever elevated white count or malaise.
Physical examination
On physical exam, arterial blood pressure should be measured in both upper extremities and pulses should also be checked in all limbs as a discrepancy could hint to a diagnosis of aortic dissection. Upon auscultation of the heart, particular attention should be paid to any new murmur, rub or gallop. A diastolic murmur caused by aortic insufficiency can be acutely seen in a patient with aortic dissection.
The examination of the chest wall and lungs are also crucial in the search of a pulmonary cause of a patient’s pain. Absence of breath sounds in an area of the thorax that is tympanic to percussion leads one to suspect a pneumothorax whereas crackles upon auscultation accompanied by egophony and dullness to percussion make the diagnosis of pneumonia more plausible.
Electrocardiogram
The approach to a patient presenting with chest pain is mostly influenced by the history and twelve lead electrocardiogram (ECG). Actually, a twelve lead ECG should be obtained within 10 minutes of presentation of all patients with ongoing chest pain and as fast as possible in all patients with resolved episode of pain but whose history is suggestive of a cardiac origin of the pain. The ECG helps determine the probability of the patient to be actively experiencing myocardial infarction. The presence of ST segment elevation that was not present on a previous ECG during the episode of chest pain is associated with an 80% likelihood of myocardial infarction. Therefore patients whose history and ECG findings are suggestive of a ST elevation myocardial infarction (STEMI) should receive either thrombolytic therapy or be directed to a cardiac catheterization laboratory for angioplasty urgently. Patients with STEMI should also receive ASA, Beta-blocker therapy and a GP IIb/ IIIa inhibitor (if undergoing percutaneous coronary angioplasty). The prevalence of myocardial infarction is around 20% in patients with ST segment depression or T wave inversion during the episode of chest pain. A completely normal ECG makes the likelihood of underlying myocardial infarction slim yet still present as up to 4% of patients with a history of coronary artery disease and a normal ECG will still have underlying myocardial infarction and up to 2% of patients with no prior cardiac history will have myocardial infarction despite a benign ECG.
Once a history, physical exam and an ECG are completed, patients can be categorized according to their risk of having an acute coronary syndrome. An acute coronary syndrome includes unstable angina or a non-ST elevation myocardial infarction (NSTEMI) which consists of non specific ECG findings along with positive cardiac biomarkers. Patients who by their history and physical exam appear to have a non-ischemic cause of their chest pain can be safely discharged home if their condition permits so. If patients are considered to be at intermediate risk or at high risk of having cardiac ischemia as an explanation to their pain, they require hospitalization and further investigation.
Laboratory data
Cardiac enzymes
When myocardial necrosis occurs, cardiac enzymes are released in the bloodstream. Cardiac enzymes are therefore routinely checked in patients presenting with chest pain that is thought to be secondary to cardiac disease. The sensitivity of the cardiac enzymes is dependent on the time between the episode of chest pain and the time of blood draw. Also serial sampling increases the sensitivity of detecting acute myocardial injury. CK-MB has a sensitivity of 34% if checked early upon presentation (single assay) that increases to 97% if checked serially. CK-MB has 90% specificity as it also released from the brain. Troponin measurement has a higher specificity as it mostly found in cardiac cells. The sensitivity is 40% if checked early upon presentation and in a single manner but the sensitivity of the test rises to 84-89% if checked serially. The cardiac biomarkers are not only measured for their diagnostic use. Positive biomarkers in patients with underlying myocardial ischemia or infarction are associated with worse outcome. Such patients benefit from more aggressive therapy.
D-dimer
The measurement of a d-dimer level may help in lowering the probability of a pulmonary emboli in a patient whose pre-test probability is slow or intermediate. The measurement of the d-dimer is highly sensitive yet not specific for pulmonary emboli. Therefore a low d-dimer level in a patient who is thought to unlikely have pulmonary emboli makes the diagnosis of pulmonary emboli extremely low. However, the workup for pulmonary emboli will be pursued in a patient whose presentation is highly suspicious for a pulmonary emboli regardless of the d-dimer result.
Imaging
Plain chest radiograph:
A plain chest radiograph is usually the first imaging modality used to evaluate chest pain in the emergency department. It is an inexpensive test that may yield important information on thoracic structures such as the lung, heart and the great vessels. It is highly sensitive to non-cardiac pathologies that are in the differential diagnosis of chest pain such as pneumonia and pneumothorax. Although one cannot diagnose an acute coronary syndrome from a chest radiograph, many indirect findings such as changes in cardiac silhouette, pulmonary edema, calcification of the myocardium or coronary arteries may suggest underlying coronary artery disease.
CTscan
The multidetector CTscan has revolutionized the diagnostic workup of acute chest pain syndromes, since they provide high sensitivity and specificity for diseases in this arena including pulmonary embolism, aortic dissection, pericardial effusion, pleural effusion and pneumonia. The study is not a “one size fits all” and needs to be tailored to the focused clinical bias. hence a acute aortic syndrome patient needs a non contrast CT and then a contrast CT that is imaged in the aortic phase of the study, and also requires an abdominal CT to evaluatetjhe extension of the dissection if present. A rule out PE study requires that the images are obtained while the contrast bolus is in the pulmonary artery. while the portential to evaluatetjhe coornary arteries and LV function is real, the study of choice when myocardial infarction is considered is cardiac catherterization since intervention, time and contrats load are the major considerations.
Cardiac Catheterization.
In the acute coronary syndromes, and particulalrly in STEMI coronary angiography with intent to both diagnose and treat the disease in a timely fashion is the intent
Resting myocardial perfusion imaging (MPI) and transthoracic echocardiography:
Both observational and prospective studies conclude that a resting myocardial perfusion imaging performed in the emergency department help reduce the rate of unnecessary hospitalizations in patients presenting with chest pain. A normal resting MPI has a negative predictive value that is equal or superior to 99% whereas a normal serum troponin level drawn at the same time has a negative predictive value of 39%. However, resting MPI is mostly useful in patients with no prior history of myocardial infarction.
A transthoracic echocardiography is most helpful during a patient’s episode of chest pain as wall motion abnormalities can be visualized within seconds of coronary artery occlusion. The echocardiogram may also aid in patients in whom symptoms have resolved. Actually, a wall motion abnormality visualized with or without pain is associated with poor prognosis. The transthoracic echocardiography can help identify or rule out many causes of chest pain such as aortic dissection, pericarditis along with pericardial tamponade and pulmonary embolism. In brief, it is a highly sensitive exam for multiple pathologies and therefore not very specific.
Stress echocardiography and radionuclide scans:
Stress echocardiography or radionuclide scans are preferred stress imaging modalities in patients with an abnormal baseline ECG or who have an inconclusive treadmill exercise ECG. Although these imaging modalities are more expensive and less available than a treadmill exercise ECG, they have a higher sensitivity to detect coronary artery disease. Also, they provide more information on extent and possible location of disease.
Red Flags
When a patient presents with chest discomfort, it is crucial to exclude life threatening diseases such as aortic dissection or myocardial infarction as both are associated with high mortality rate if left undetected and untreated. red flags should be raised in all patients with red flags.
Although udden severe pain that is lasting rasises a red flag, some of these severe diseases can present with minimal symptoms.
Aortic dissection is an often missed cause of chest pain. A high level of suspicion is necessary. A tearing character of the pain along with a radiation to the back that is associated with a difference in blood pressure is concerning for aortic dissection.
Patients presenting with chest pain, which is by history suggestive of myocardial ischemia, and are found to have ST segment elevation on a twelve lead electrocardiogram need to be directed to a cardiac catheterization laboratory urgently.
Pleuritic pain almost always has an underlying disorder, and therefore should be evaluated methodically until the cause is identified.
Conclusion
Chest pain is an important and serious symptom. As mentioned frequently in the module, the nature of the pain established in the history is the critical step in the evaluation. Thus careful and thoughtful questioning should be the initial diagnosstic methodology. Since many of the conditions are relatively common it would not be unusual for a patient to have for example both reflux esophagitis and angina. Thus the finding and treating of one may not abate the symptomatology.
We have outlined the common causes and character of the pain syndromes. When a patient is suspected of an acute myocardial event and particularly an AMI, the patient should be informed in a calm yet serious way of the events that may unfold. Included in the workup would be the admission to a coronary care unit, the drawing of serial bloods for enzymes and the performance of EKG. Cardiac catheterization, sometimes on an emergency basis is performed for diagnostic and therapeutic reasons.
When considering myocardial ischemia, atypical characteristics of the pain make the pain less likely to be secondary to myocardial ischemia or injury. Per the AHA/ACC guidelines, the pain is considered atypical if it is pleuritic in nature, if the primary or sole discomfort of pain is in the middle or lower abdominal region, if it can be localized with one finger, if it is reproduced with movement or palpation of the chest wall or arms, if it persists for hours or if it very brief and lasts seconds. An atypical presentation of pain makes cardiac ischemia less likely, however not impossible as the cause of pain. Certain groups of patients such as women, diabetic and elderly persons notoriously present with atypical manifestation of myocardial ischemia.
When dissection is the concern, then the essential diagnostic information is the location of the dissection since ascending dissections require surgery.
When pulmonary embolism is the suspicion, the presence of emboli requires the initiation of anticoagulation therapy.
There are many instances where the cause of the pain is not established, but careful follow up of these patients is essential.
References
Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine
Lee T, Goldman L. Evaluation of the Patient with Acute Chest Pain. NEJM 2000; 342: 1187-1195
Luepker RV, Apple Fs et al: Case definitions for acute coronary disease in epidemiology and clinical research studies. Circulation 108:2543, 2003
Picano E, Economic and biological costs of cardiac imaging – Cardiovasc Ultrasound 2005; 3:13
Prasad SK, Assomull RG, Pennell, DJ Recent developments in non-invasive cardiology – BMJ 2004; 329:1386-1389
Spodick DH. Acute pericarditis: Current concepts and practice. JAMA 2003; 289:1150-1153
Zaret BL , Wackers, FJ Nuclear Cardiology – First of Two Parts – NEJM 1993; 329:775-783
Zaret BL , Wackers, FJ Nuclear Cardiology – Second of Two Parts – NEJM 1993; 329:855-863
Web References
eMedicine Acute Coronary Syndrome Drew E Fenton, MD
eMedicine Aortic Dissection John Wiesenfarth, MD, MS, FACEP, FAAEM
eMedicine Angina Pectoris Jamshid Alaeddini, MD, FACC
eMedicine GERD P Marco Fisichella, MD
eMedicine Herpes Zoster Richard S Krause MD
eMedicine Myocardial Infarction Drew E Fenton, MD
eMedicine Pneumothorax Fahad M Alhameed, MD, AmBIM, FCCP, FRCPC eMedicine Pulmonary Embolism Sat Sharma, MD, FRCPC
eMedicine Pulmonary Hypertension, Idiopathic Ronald J Oudiz, MD
e Medicine Pleurodynia Irina Petrache, MD
e Medicine Pneumonia Bacterial Sat Sharma, MD, FRCPC
eMedicine Pneumonia Viral Sat Sharma, MD, Sat Sharma, MD, FRCPC
MCQ
- A 60 year old man with a history of hypertension and diabetes presents to the emergency room with sudden onset of substernal chest pain associated with shortness of breath and diaphoresis. What is the
most appropriate next step?
- a) Obtain a twelve lead electrocardiogram
- b) Obtain a CT scan of the chest
- c) Arrange an outpatient appointment with the patient’s primary care physician
- d) Reassure the patient that he suffers from gastroesophageal reflux and discharge him home
- e) Excecise Test immediately
answer a
- A tall and thin 20 year old college student presents to the emergency room after he developed sudden onset of right sided chest pain associated with shortness of breath. What is the most likely diagnosis?
- a) acute coronary syndrome
- b) pneumonia
- c) gastroesophageal reflux disease
- d) spontaneous pneumothorax
- e) myocardial infarction with ST elevation
answer d
- Which of the following are considered risk factors for the developpement of a pulmonary embolus?
- a)Prolonged travel
- b)Recent surgery
- c)Underlying malignancy
- d) hypercoaguable state
- e)All of the above
answer e
- A 70 year old female with a history of poorly controlled hypertension presents to the emergency
room with sudden onset of 8/10 chest pain radiating to her back. She feels unwell and short of breath. Which of the following findings is suggestive of acute aortic dissection?
- a)Similar blood pressure measurements in both arms
- b) A new diastolic murmur on cardiac auscultation
- c)An infiltrate on the chest radiograph
- d)Fever
- e) Gastroesophageal Reflux
Answer b
5) A 68 year old male presents to the emergency room with a 40 minute history of chest pain and is found to have ST segment elevation on his twelve lead electrocardiogram. Immediate measures of oxygen administartion and an intravenous line have been started. What is the most appropriate next step in managing the patient?
- a)Admit the patient and organize a barium swallow to rule out gastroesophageal spasm
- b)Admit the patient and arrange for urgent cardiac catheterization
- c)Check a urine toxicology screen
- d)Treat with antibiotics
- e) Cardiac echo to evaluate left ventricular wall motion
Answer b
- Which of the following is not associated with pericarditis?
- a)Uremia
- b)Recent myocardial infarction
- c)Recent upper respiratory infection
- d) Viral Infection
- e)Recent orthopedic surgery
Answer e
- What is the treatment for pericarditis?
- a)thrombolytic therapy
- b)Heparin
- c)NSAID
- d)Antibiotic therapy
- e) Pericardiocentesis
Answer c
- Which of the following can lead to myocardial ischemia or infarction?
- a)ruptured coronary plaque
- b)aortic dissection
- c)coronary vasospasm
- d) coronary thrombosis
- e)all of the above
Answer e
- A 49 year old female with a history of hypertension presents to the emergency room with severe chest pain radiating to her scapula. She is found to have an aortic dissection involving her ascending aorta on a transthoracic aorta performed urgently. Which is the most appropriate treatment?
- a)beta blocker therapy to control her blood pressure
- b)cardiac catheterization
- c)aspirin
- d)urgent surgery
- e) aortic stent of the descending aorta to prevent retrograde extension
Answer d
- Which of the following conditions can be associated with pulmonary hypertension?
- a) obstructive sleep apnea
- b) chronic obstructive pulmonary disease
- c) congestive heart failure
- d) congenital heart disease
- e) all of the above
Answer e
- Which of the following tools is not useful to diagnose pulmonary hypertension?
- a) transthoracic echocardiogram
- b) right sided cardiac catheterization
- c) pulmonary function tests
- d) chest CT scan
- e) Swan-Ganz catheter
Answer c
- Which of the following tests is most specific in diagnosing a pulmonary emboli?
- a)Chest CT angiogram
- b)D-dimer
- c)Cardiac enzymes
- d)Chest Xray
- e) Cardiac echo
Answer a
- True or false:
All patients with chest pain due to a pulmonary emboli will benefit from thrombolytic therapy.
Answer False
- Which of the following statements about pneumonia is untrue:
- a)Patients usually present with shortness of breath, cough and fever
- b)Pain is usually pleuritic in nature
- c)An infiltrate can be appreciated on a chest Xray
- d) Can be caused by a virus or a bacteria
- e)A transthoracic echocardiogram is essential for the diagnosis
Answer e
- Which of the following can contribute to gastroesophageal reflux?
- a) Gravid condition
- b) Obesity
- c) Consumption of a rich, fatty meal
- d) Hiatus Hernia
- e) All of the above
Answer e
- What is the best method to diagnose gastroesophageal reflux disease?
- a)history suggestive of gastroesophageal reflux
- b)endoscopy
- c)barium swallow
- d)abdominal X-Ray
- e) Abdominal CT scan
Answer a
- Which is not considered part of the therapy of gastroesophageal reflux?
- a)proton pump inhibitor
- b)avoiding heavy meals at night
- c)weight reduction
- d)aspirin therapy
- e) elevation of the head of the bed
Answer d
- An 18 year old male with a recent upper respiratory tract infection presents to his primary care physician’s office with chest pain that worsens upon lying down. A twelve lead electrocardiogram reveals diffuse ST segment elevations. What is the most likely cause of the patient’s pain?
- a)costochondritis
- b)rib facture
- c)pericarditis
- d)STEMI (myocardial infarction)
- e) angina
Answer c
- An 80 year old male with a history of tobacco use and lung cancer presents with acute onset of sharp right sided chest pain. His pain worsens upon coughing and upon taking a deep breath. His physical examination is unremarkable. What is the most likely diagnosis?
- a)pathological rib fracture
- b)acute coronary syndrome
- c)pneumothorax
- d)gastroesophageal reflux disease
- e) New STEMI
Answer a
- A 24 year old male is brought to the emergency room with chest pain after being involved in a motor vehicle accident. Which from the following is the least likely cause of his pain?
- a)myocardial contusion
- b)pericarditis
- c)aortic traumatic dissection
- d)pneumothorax
- e) sternal fracture
Answer b