

Courtesy: Henri Cuenoid, M.D.
Fibrofatty Plaque if only it were big enough we could characterize the plaque
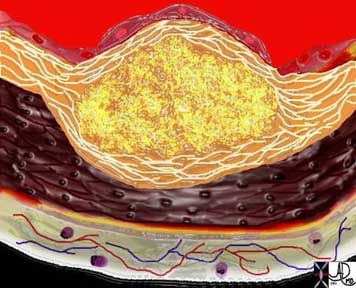
The diagram shows the atherosclerotic lesion in the subepithelial layer of the intima which is bulging both toward the media and toward the lumen. There is a central core of fat and necrotic debris, surrounded by fibrous elements which give the plaque its hardness to the feel. The accumulation of fibrous tissue heralds an advanced atherosclerotic lesion.
Ashley Davidoff, M.D.

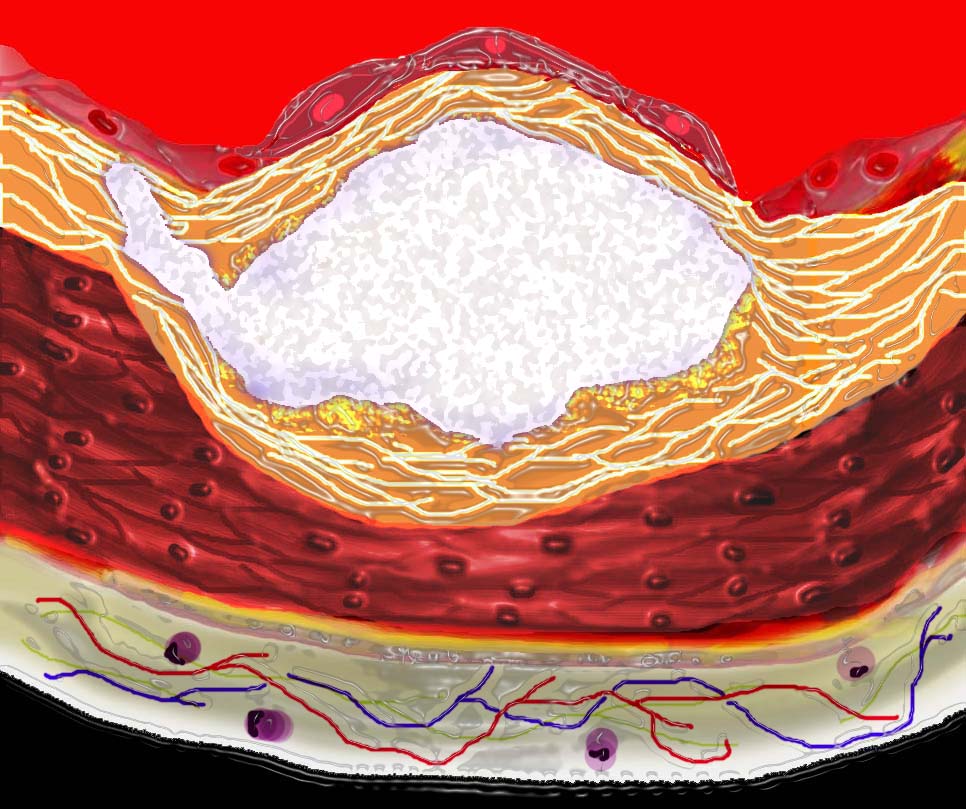
This diagram shows denudation of the endothelial layer with exposure and rupture of the contents of the atherosclerotic plaque in volcanic fashion into the lumen. This event is catastrophic and can result in acute thrombosis and may even be a fatal event.
Ashley Davidoff, M.D.(aorta-Philips-041)
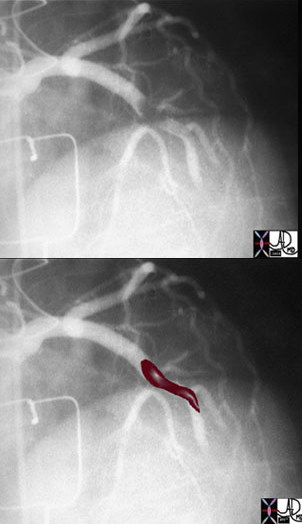
The above image of this cardiac catheterizatishows a coned down left anterior oblique (LAO) projection of the LAD in a patient with acute thrombosis of the left anterior descending artery. In the lower image, the thrombus in the artery is overlaid in maroon.
Calcification – Advantages and Disadvantages in CT
- Density makes it easy to see
- Calcium score
- Risk Stratification
- Limits visualization of the lumen
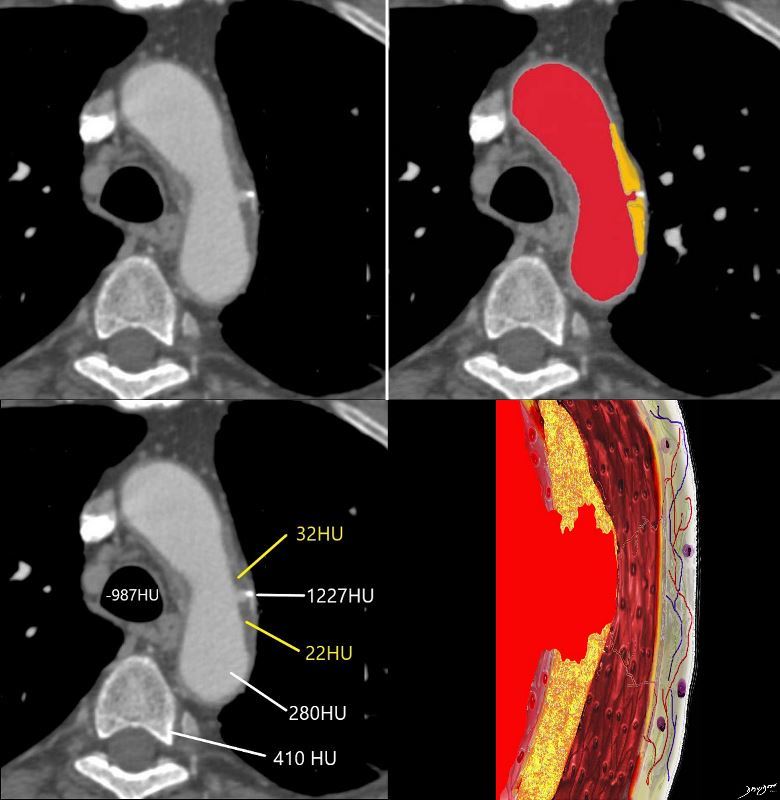
Progressive dystrophic calcification results in increase in the volume of the plaque. It may grow toward the external surfaceof the artery, in which case it has no hemodynamic significance or toward the lumen in which case it progressively impinges on the lumen
Ashley Davidoff
thecommonvein.net
This process is the same process that occurs in the coronary arteries – a vessel with a similar makeup of the wall undergoes the atherosclerotic process and fatty degeneration . The natural history and complications of this disease in the aorta – ie potential to dissect and rupture theoretically should happen in the coronary artery and other arteries
What we have yet to discover I believe, is that this may also happen in any of the medium sized arteries including the cotronary arteries and if so would broaden our understanding on the variability of clinical presentations and natural history of the disease
The densities of the atherosclerotic process which at this time are measured in a relatively crude way are however important. The fibrofatty plaque measures in the 20HU unit range, is well below soft tissue range which should be in the 50-70 range. The calcified plaque at 1227HU is distinctly different from cortical bone which is only 410 HU
Ashley Davidoff thecommonvein.net