
both great arteries arise 50% or more from the right ventricle (RV).
-

Diagram of the Embryological origins and Consequences of Conotruncal Malformations in a D Loop
embryology bilateral conus DORV growth resorption normal mitral to aortic continuity transposition D transposition double outlet right ventricle
Ashley Davidoff art copyright 2019
06394c01L.800s
TheCommonVein.net
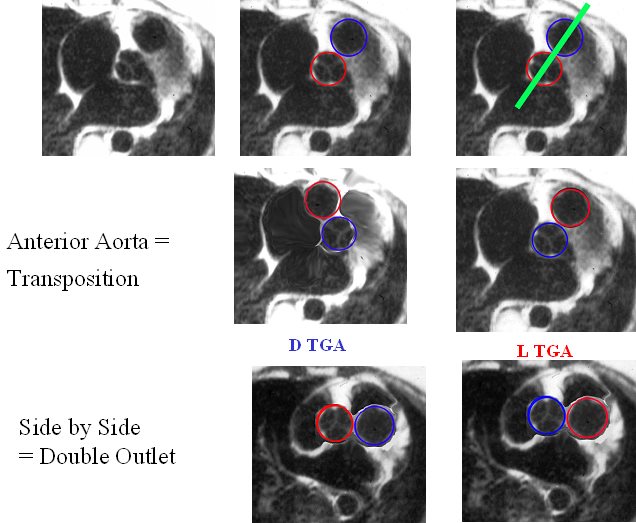
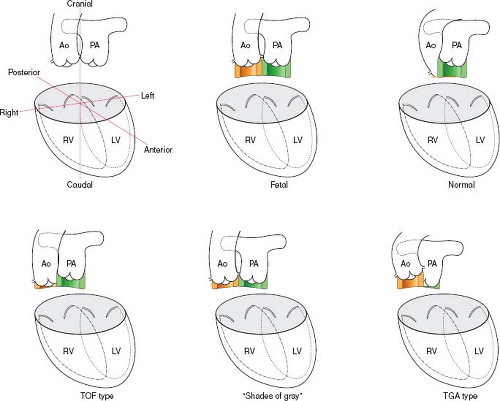
The image reflects the relationship of the aorta and pulmonary arteries in the normal patient, in DTGA, LTGA and DORV. In the normal patient with D loop the aorta (Ao) is posterior and to the right, and the pulmonary artery (PA) is anterior and to the right. In the patient with DTGA, the Ao is anterior and to the right and the PA is posterior and to the left. In an L loop the Ao is anterior and to the left and the PA is posterior and to the right. In double outlet right ventricle (DORV) the great vessels lie side by side and in DORV with a D loop the aorta is to the right and with an L loop the aorta is to the left
86778 01639 01639d02 01639d04 01639f03.jpg Anterior aorta = Transposition
Ashley Davidoff MD
TheCommonVein.net

At this stage the heart is close to totally septating but before this happens the left ventricle and aorta have to connect in order to create a systemic circulation that is separate from the pulmonary circulation. The aorta lies to right of the pulmonary artery and still has a subaortic conus. In order to connect with the left ventricle and mitral valve, the subaortic conus has to resorb. Mr Aorta has a his eyes set on Ms Mitral Valve
Ashley Davidoff MD TheCommonVein.net
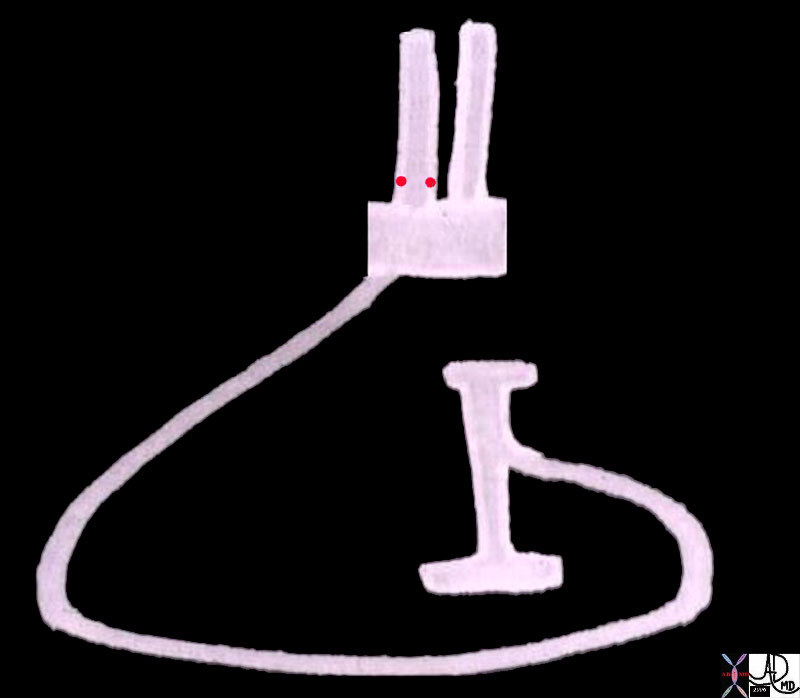
DORV is an arrested phase of development when both great vessels are above the RVand both still have a conus. The vessels lie side by side.
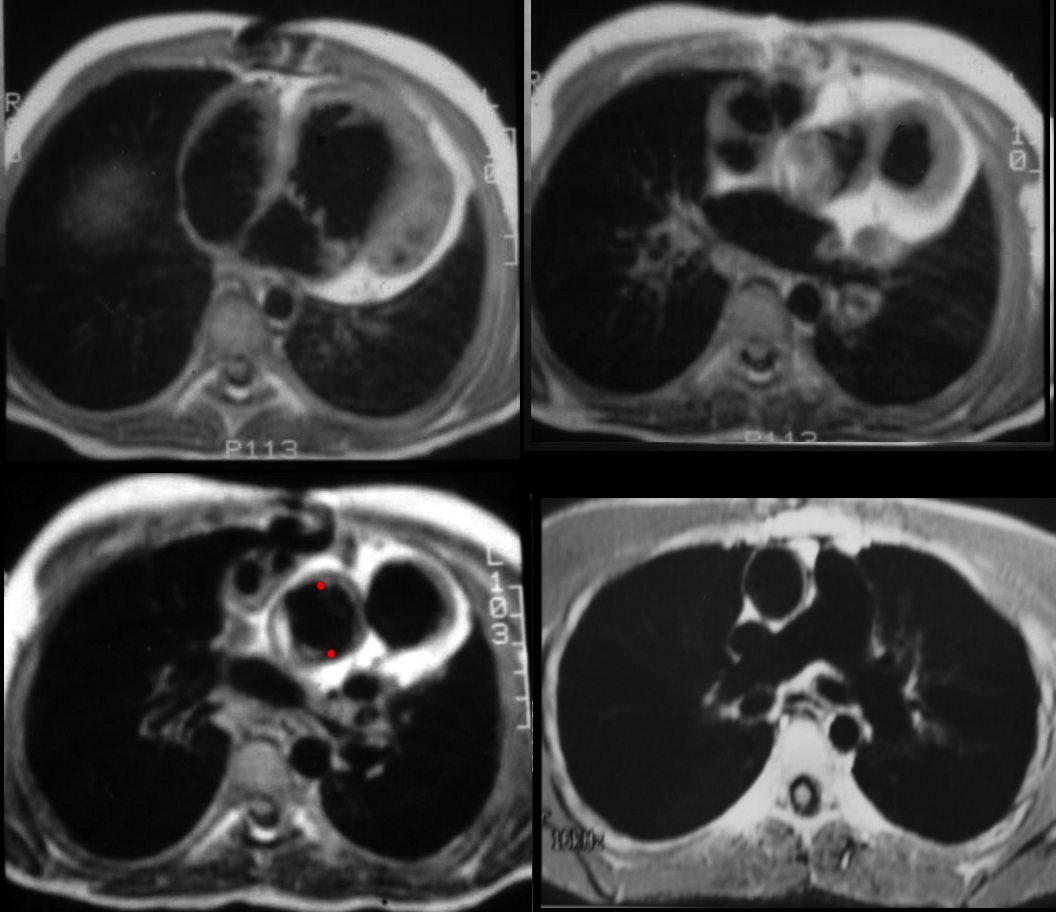
The axial CT of a 9 year old male reveals a findings characteristic of DORV with both great vessels lying side by side with bilateral conus (bottom images). The aorta was to the right and pulmonary artery to the left reflecting a D loop . There was a subpulmonary VSD and hence the diagnosis is Taussig Bing anomaly.
07207e01c01 heart cardiac aorta pulmonary artery RVOT conotruncal malformation DORV Taussig Bing position connection relation embryology CTscan Davidoff MD 28994 28995 28996 28997 28998 28999 MRI Ashley Davidoff MD TheCommonVein.net
|
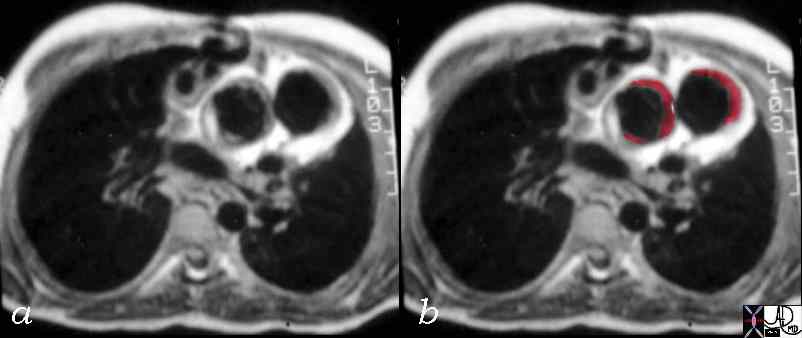
Bilateral Conus Side by Side vessels Taussig Bing Anomaly |
| 07207c02 bilateral conus cardiac heart CHD DORV bilateral infundibula double outlet right ventricle double outlet RV Taussig Bing MRIscan Davidoff MD |
|
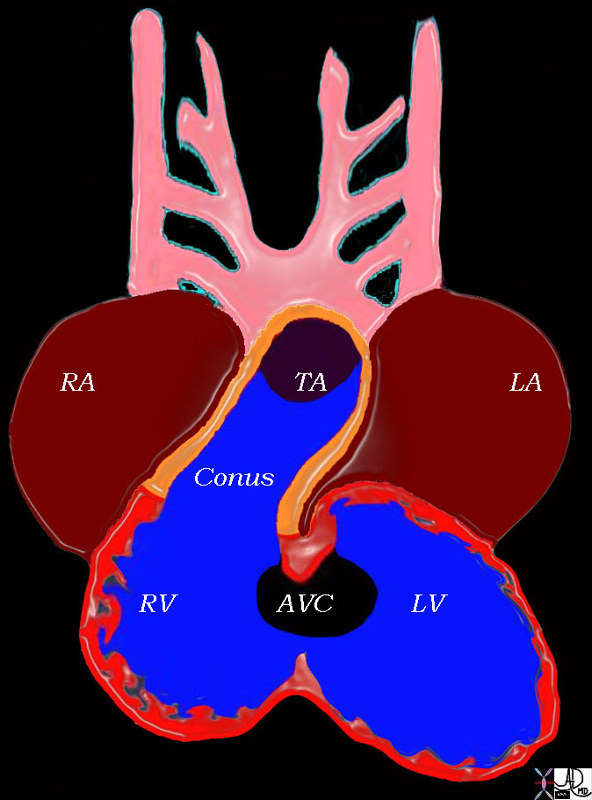
Early Development Bilateral Conus Truncus Arteriosus Arises off the RV
|
| 06362b01 heart cardiac bilateral conus outflow tract infundibulum aorta pulmonary artery D-loop RV LV conoventricular defect bilateral conus atrioventricular endocardial cushion mitral valve anatomy embryology subaortic conus subpulmonary conus fibrous continuity MV Courtesy Ashley Davidoff Davidoff drawing |
|
Early Development Bilateral Conus Truncus Arteriosus Arises off the RV |
| 01492b04L heart cardiac right atrium left atrium right venricle left ventricle atrioventricular canal conus arteriosus truncus arteriosus aortic arches RA LA RV LV AVC embryology Davidoff drawing Davidoff MD |
Variations
- a – similar to tetralogy of Fallot
- near-normal length of conus beneath the pulmonary valve and minimal conus beneath the aortic valve. The aorta is closer to the LV and VSD closer aorta so aorta gets oxygenated blood
- b – bilateral conus
- equal bilateral conus, Taussig Bing
- c – similar to TGA
- conus mostly under the aortic valve but has a small amount of conus under the pulmonary valve so pulmonary valve and PA is closer to VSD and so PA gets oxygenated blood and Ao gets deoxygenated blood
- d – many “shades of gray,” –
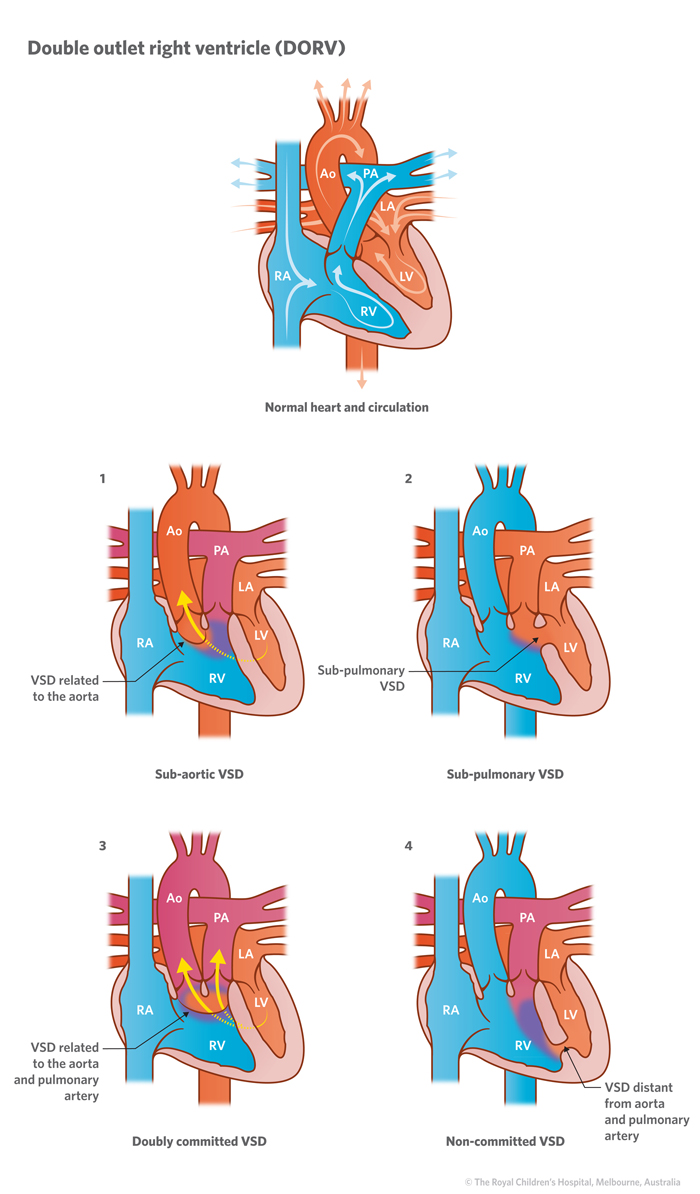
The upper left diagram (1) shows an abnormality similar to Tetralogy of Fallot, but without obstruction to flow to the lungs. Repair involves placement of a patch within the right ventricle to direct LV flow to the aorta.
In the type called the ‘Taussig Bing’ anomaly (top right diagram 2) blood from the LV passes through the VSD to the Pulmonary Artery, whilst blood from the RV tends to be directed mainly to the Aorta. This is similar in many ways to Transposition with a VSD and It may be treated with an ‘Arterial Switch’ operation along with a patch within the right ventricle to direct flow to the arterial valve adjacent to the VSD.
The illustration labelled ‘Doubly Committed VSD’ (3) shows a rare variant which may be suitable for repair in a similar way to the first type. The fourth diagram shows a ‘Non Committed VSD’ (4) in which the VSD is distant from both arteries and blood ‘mixes’ in the right ventricle. This is sometimes suitable for repair but in other cases a Fontan procedure may be considered. Double-Outlet Right Ventricle Gail E. Wright et al thoracic key.com
The upper left diagram (1) shows an abnormality similar to Tetralogy of Fallot, but without obstruction to flow to the lungs. Repair involves placement of a patch within the right ventricle to direct LV flow to the aorta.
In the type called the ‘Taussig Bing’ anomaly (top right diagram 2) blood from the LV passes through the VSD to the Pulmonary Artery, whilst blood from the RV tends to be directed mainly to the Aorta. This is similar in many ways to Transposition with a VSD and It may be treated with an ‘Arterial Switch’ operation along with a patch within the right ventricle to direct flow to the arterial valve adjacent to the VSD.
The illustration labelled ‘Doubly Committed VSD’ (3) shows a rare variant which may be suitable for repair in a similar way to the first type. The fourth diagram shows a ‘Non Committed VSD’ (4) in which the VSD is distant from both arteries and blood ‘mixes’ in the right ventricle. This is sometimes suitable for repair but in other cases a Fontan procedure may be considered.
Royal Children’s Hospital in Melbourne
From Slide Player
The axial CT of a 9 year old male reveals a findings characteristic of DORV with both great vessels lying side by side with bilateral conus (bottom images). The aorta was to the right and pulmonary artery to the left reflecting a D loop . There was a subpulmonary VSD and hence the diagnosis is Taussig Bing anomaly.
07207e01c01 heart cardiac aorta pulmonary artery RVOT conotruncal malformation DORV Taussig Bing position connection relation embryology CTscan Davidoff MD 28994 28995 28996 28997 28998 28999 MRI Ashley Davidoff MD TheCommonVein.net
Tetralogy Type – Subaortic VSD – partial resorption of conus
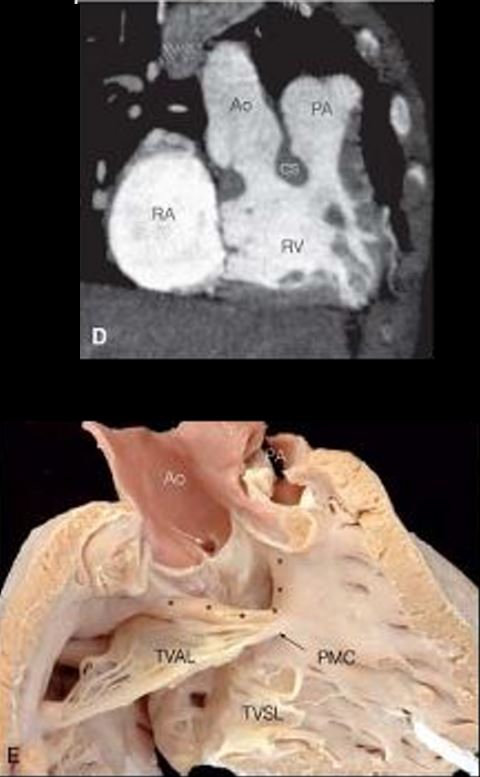
Computed tomography angiogram, oblique image: CT angiography demonstrates both great arteries arising from the right ventricle, with conal septum separating the aorta and the pulmonary artery. RA, right atrium; Ao, aorta; PA, pulmonary artery; CS, conal septum; RV, right ventricle. E: Pathologic specimen: The VSD is bounded by the underside of the aortic valve and cradled in the arms of the septomarginal trabeculations. The pulmonary artery is walled off by infundibular muscle. Asterisks, borders of the VSD; white arrow, coronary artery orifice; black arrow, PMC, papillary muscle of the conus; Ao, aorta; PA, pulmonary artery; TVAL, tricuspid valve anterior leaflet; TVSL, tricuspid valve septal leaflet; D courtesy of Frandics Chan, MD, PhD, Stanford University; E courtesy of Diane Spicer, BS, University of Florida.)
Courtesy Double-Outlet Right Ventricle Gail E. Wright et al thoracic key.com
TGA type with Subpulmonary VSD
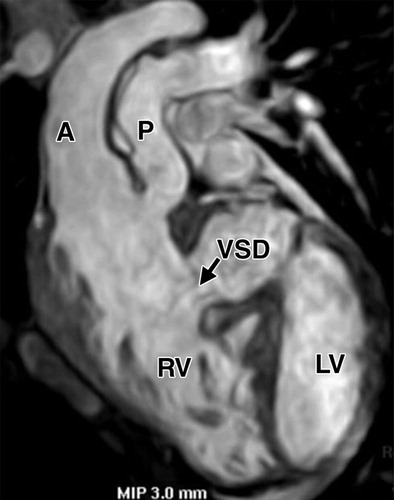
(Frank L et al Cardiovascular MR Imaging of Conotruncal Anomalies Radiographics)
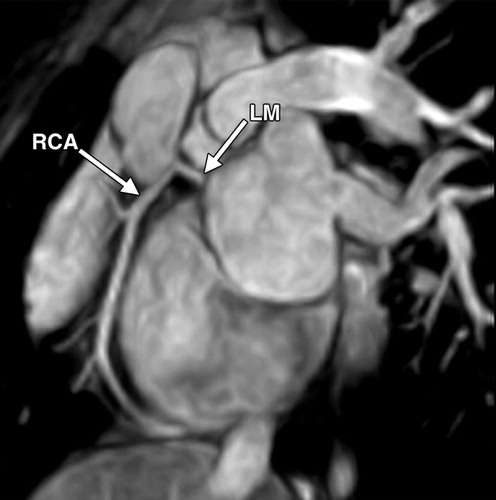
(b) Oblique sagittal image from the same acquisition as a shows a common origin of the left main (LM) and right (RCA) coronary arteries
(Frank L et al Cardiovascular MR Imaging of Conotruncal Anomalies Radiographics)
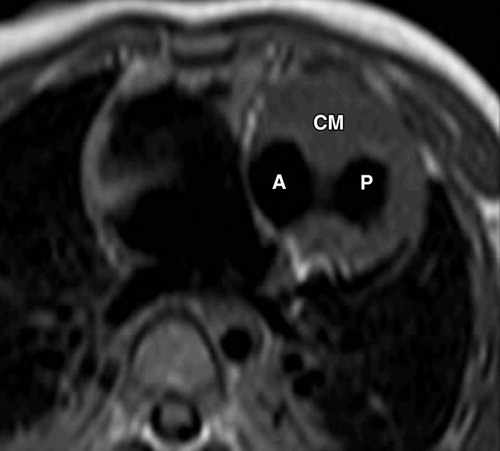
(Frank L et al Cardiovascular MR Imaging of Conotruncal Anomalies Radiographics)

Prenatal ultrasound demonstration of scoliosis, absence of one rib, a radial club hand, congenital heart defects and absent stomach in a fetus with VACTERL association
March 2012Taiwanese Journal of Obstetrics and Gynecology 51(1):139-42
References
Double-Outlet Right Ventricle Gail E. Wright et al Chapter Thoracic Key.com
- TCV
- Conotruncal Abnormalities
- Embryology
- Anatomy of the Right Ventricle
- Double Outlet Right Ventricle
- Double Outlet Left Ventricle
- Tetralogy of Fallot
- Transposition of the Great Vessels
- Truncus Arteriosus