
Hypertrophic Cardiomyopathy
Copyright 2020
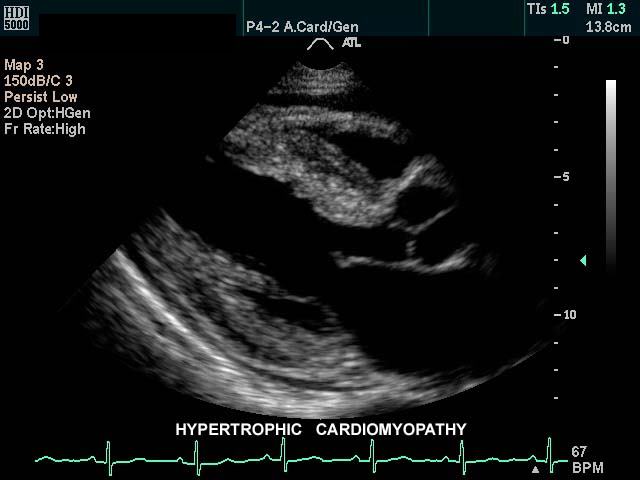
Hypertrophic cardiomyopathy (HCM) is the leading cause of sudden death (from arrhythmias) in infants, teenagers, and young adults.
Asymmetric Hypertrophic Cardiomyopathy (most common)
This gray scale echo of the heart shows the left ventricle, anterior (light pink) and posterior leaflets of the mitral valve, the aortic valve (dark pink), and the base of the aorta. There is a focal thickening of the ventricular septum (green) in the left ventricular outflow tract just proximal to the aortic valve. The region is also slightly more echogenic than the remaining myocardium (maroon). This case demonstrates a case of asymmetric septal hypertrophy or muscular subaortic stenosis.
Courtesy Philips Medical Systems 33134 33134c04.8s
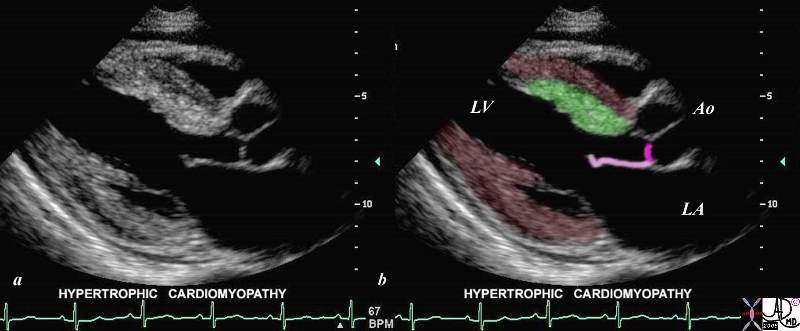
This gray scale echo of the heart shows the left ventricle, anterior (light pink) and posterior leaflets of the mitral valve, the aortic valve (dark pink), and the base of the aorta. There is a focal thickening of the ventricular septum (green) in the left ventricular outflow tract just proximal to the aortic valve. The region is also slightly more echogenic than the remaining myocardium (maroon). This case demonstrates a case of asymmetric septal hypertrophy or muscular subaortic stenosis.
Courtesy Philips Medical Systems 33134 33134c04.8s
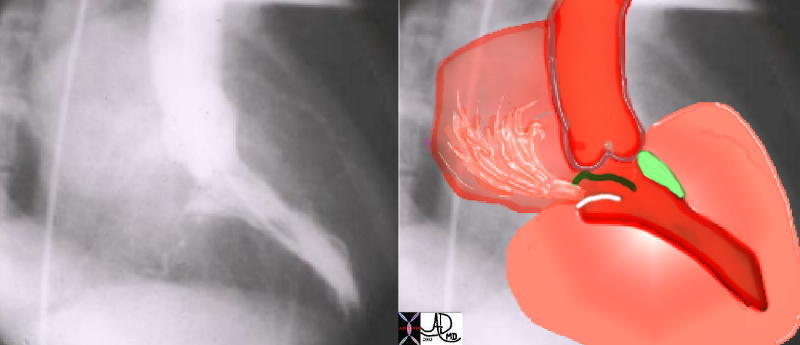
This angiogram in RAO projection shows a hypercontractile left ventricle that has a ballet shoe appearance, with mitral regurgitation filling the left atrium. The drawing shows the significant LVH small cavity of the LV, the area of subaortic muscle bundle (green) and the mitral regurgitation caused by the systolic anterior motion of the mitral valve.
Courtesy Ashley Davidoff 34805 cardiac heart MV interventricular septum LVH IHSS SAM MR imaging radiology angiography disease overlay
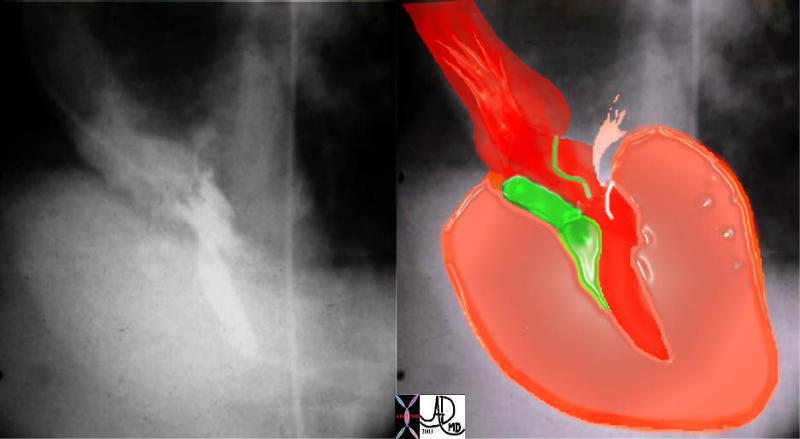
Courtesy Ashley DAvidoff MD 34806 cardiac heart MV interventriclar septum LVH IHSS SAM MR imaging radiology angiography disease overlay

This gray scale echo of the heart shows the left ventricle, anterior and posterior leaflets of the mitral valve, the aortic valve and the base of the aorta. There is a focal thickening of the ventricular septum in the left ventricular outflow tract just proximal to the aortic valve. The region is also slightly more echogenic than the remaining myocardium. This case demonstrates a case of asymmetric septal hypertrophy or muscular subaortic stenosis. Courtesy Philips Medical Systems 33135 code cardiac heart echo LV septum thick LVOT narrow echogenic ASH IHSS imaging cardiac echo
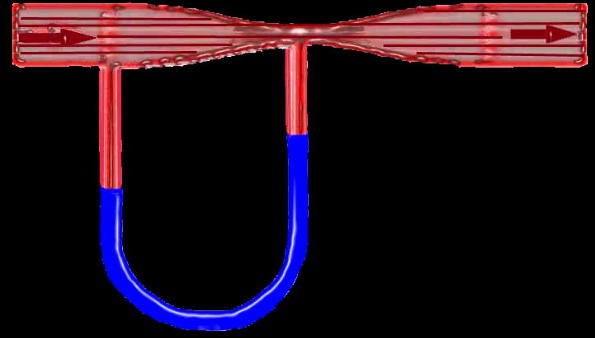
Flow in this tube is demonstrated by the arrows going from right to left through a narrowing in the tube (red) demonstrating a vacuum or suction effect caused by the sudden acceleration of the fluid as it goes through the narrowing or stenosis. This is seen in the U shaped monometer with the fluid level in blue being relatively higher at the site of the stenosis in relation to the pressure more upstream. The suction phenomenon is known as the Venturi effect is seen in IHSS where the narrowing of the LVOT causes a vacuum effect on the anterior leaflet of the MV resulting in mitral regurgitation. The Venturi effect is also utilised in the functioning of carburettors in fuel driven engines.
34807b05 code heart cardiac SAM IHSS pressure drop vacuum suction acceleration stenosis Venturi effect tube principles
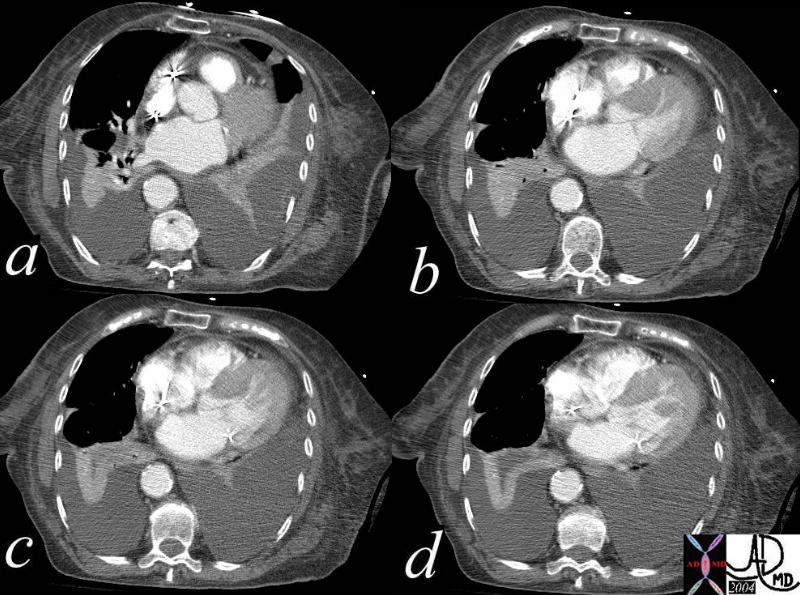
This series of axial CTscans show asymmetric thickening of the ventricular septum in this patient with known diagnosis of IHSS (idiopathic hypertrophic subaortic stenosis) and known systolic anterior motion of the mitral valve. The CT was performed one day after an RV perforation following placement of a pacemaker. Note also the left atrial enlargement, thickening of the RVOT, bilateral pleural effusions with passive compressive atelectasis. Courtesy Ashley Davidoff MD 39203c code CVS heart LV myocardium thickness asymmetric hypertrophy RS lung pleura effusion atelectasis imaging radiology CTscan
Concentric Hypertrophy
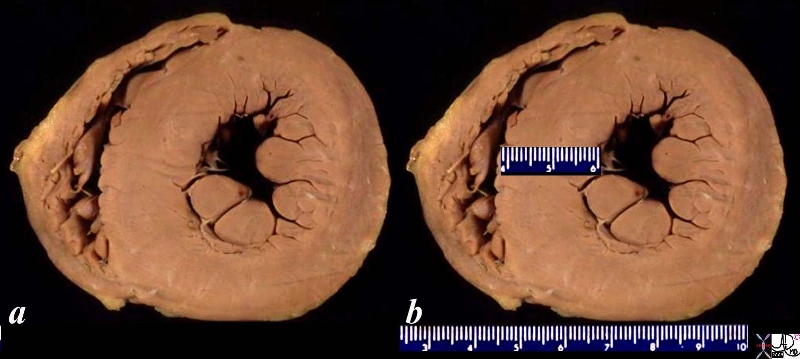
08028b06 heart cardiac LV left ventricle papillary muscles RV right ventricle LVH left ventricular hypertrophy thickened LV concentric hypertrophy interventricular septum thickened enlarged gross pathology Courtesy Ashley Davidoff MD
Ashley Davidoff MD
Ashley Davidoff MD
Apical Hypertrophic Cardiomyopathy Yamaguchi Syndrome
“Ace of Spades”
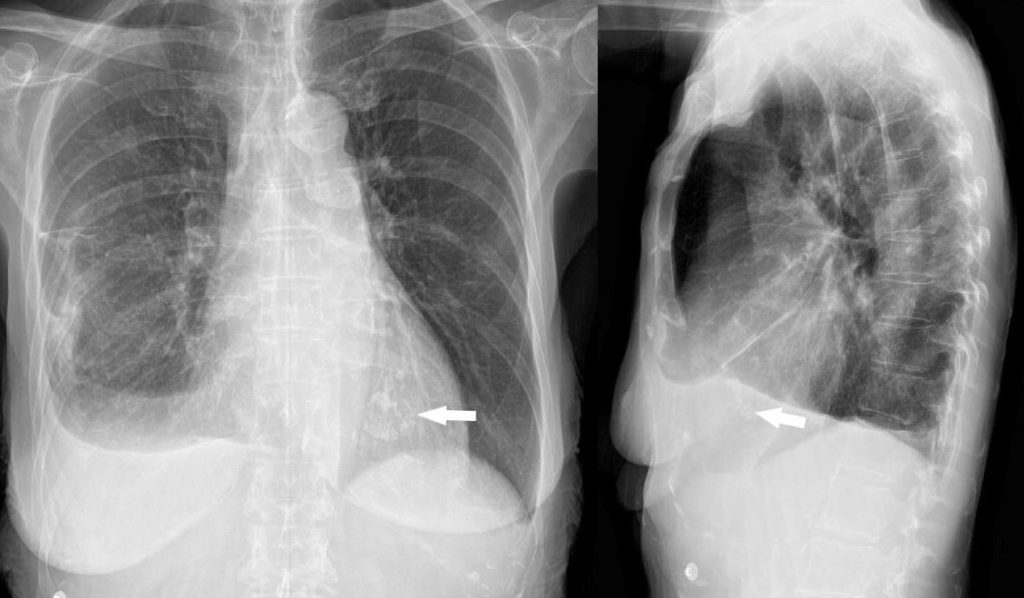
The chest X-ray in PA and lateral projections shows a cluster of calcifications in the region of the left ventricular apex (arrows). The patient is a 73 year old female with apical hypertrophic disease . She has a history of diastolic heart failure, pulmonary hypertension, CREST syndrome, esophageal stricture, COPD and chronic renal failure
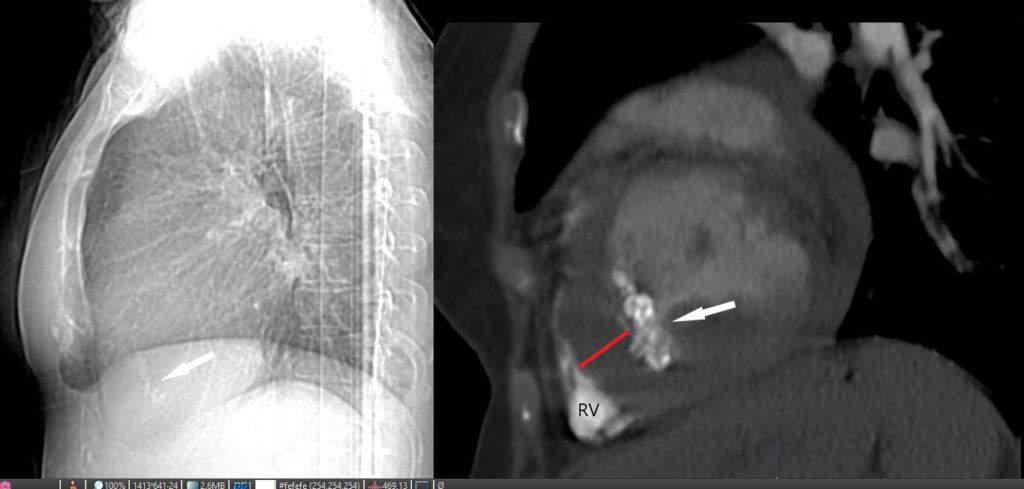
The left image is a lateral view of the chest, and the arrow points to the intracardiac calcification. The image on the right is a CT scan of a sagittal view of the left ventricle showing LV apical hypertrophy (red line), mass-like calcification in the LV cavity (white arrow) and contrast in the right ventricle.
The patient is a 73 year old female with apical hypertrophic disease. She has a history of diastolic heart failure, pulmonary hypertension, CREST, esophageal stricture, COPD and chronic renal failure

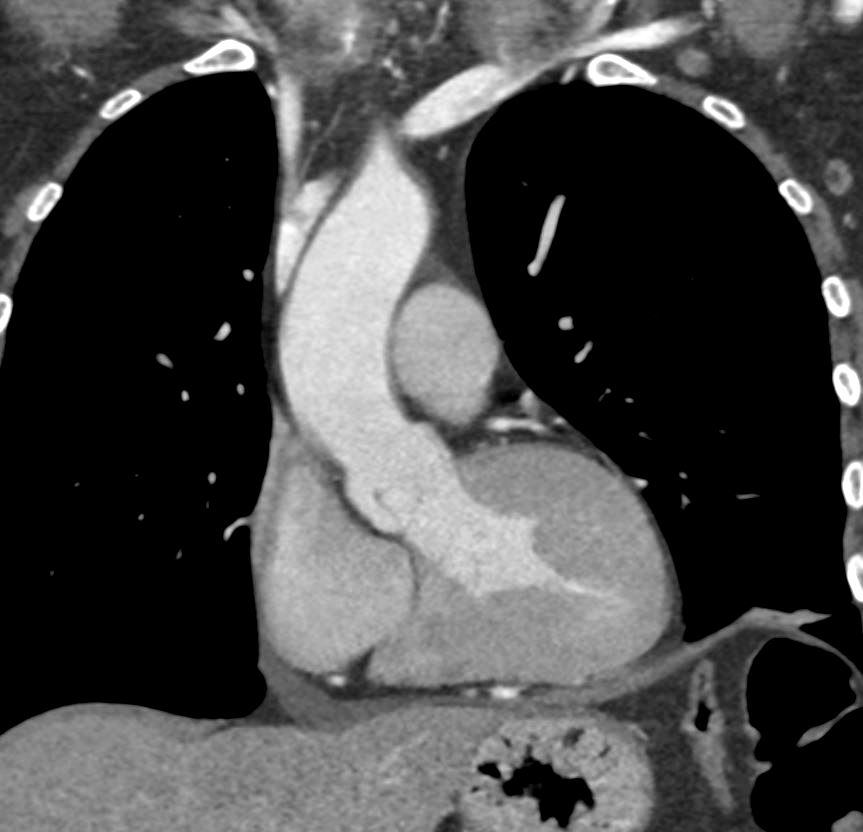
The CT axial images shows native image on the left . Markers on the right image, show left ventricular (LV) apical hypertrophy (red line) calcified mass in the apex (white arrow) LV cavity with contrast (red dot) and pericardial effusion (pink arrow)
The patient is a 73-year-old female with apical hypertrophic disease. She has a history of diastolic heart failure, pulmonary hypertension, CREST, esophageal stricture, COPD and chronic renal failure
heart0069b02 Ashley Davidoff MD
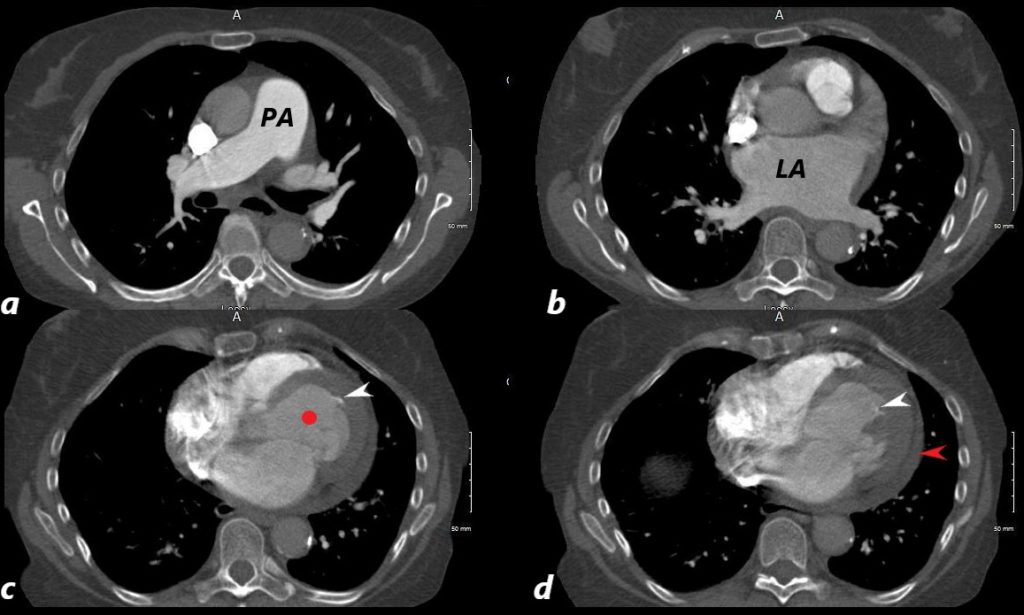
The CT axial images shows an enlarged pulmonary artery (PA) indicating pulmonary hypertension, and I an enlarged left atrium (LAE, b) , a small left ventricular (LV) cavity (red circle , c) calcified foci in the LV (c and d white arrows, and a small pericardial effusion (red arrow d)
The patient is a 73-year-old female with apical hypertrophic disease. She has a history of diastolic heart failure, pulmonary hypertension, CREST, esophageal stricture, COPD and chronic renal failure
Ashley Davidoff MD
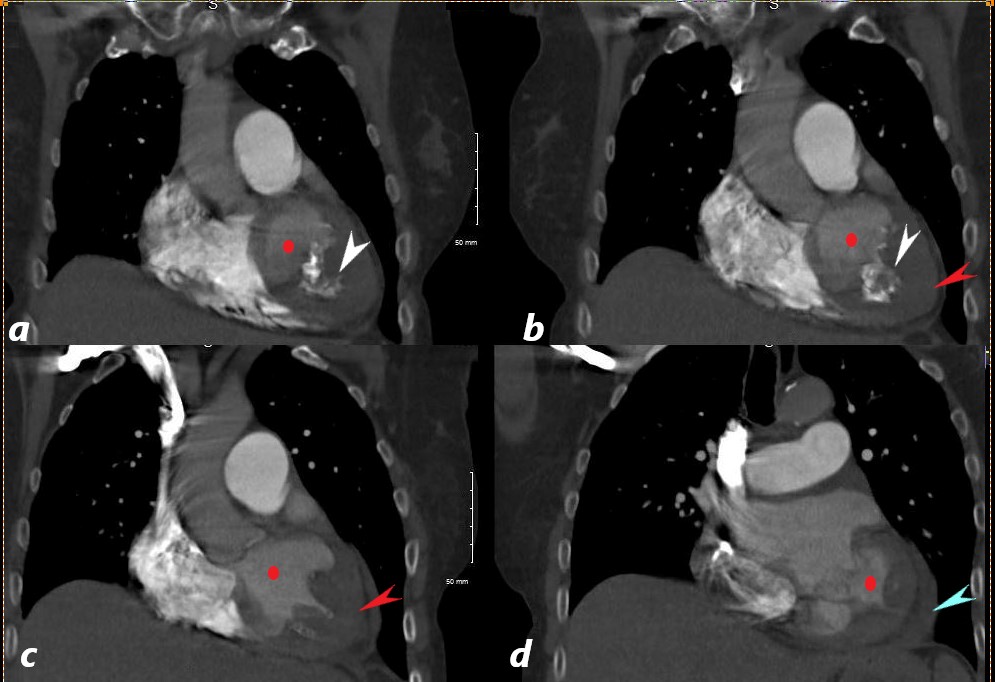
The CT coronally reconstructed images show a small left ventricular (LV) cavity (red circle ,a,b,c,d) intracavitary calcification (white arrow a,b), apical LV hypertrophy (LVH, red arrows b, and c) and a small pericardial effusion (blue arrow, d)
The patient is a 73-year-old female with apical hypertrophic disease. She has a history of diastolic heart failure, pulmonary hypertension, CREST, esophageal stricture, COPD and chronic renal failure
Ashley Davidoff MD

The barium swallow shows a mass filling defect in the distal esophagus (white arrowheads) and a stricture in the distal esophagus (red arrow). At endoscopy a bezoar was identified associated with a benign stricture.
The patient is a 73-year-old female with apical hypertrophic disease. She has a history of diastolic heart failure, pulmonary hypertension, CREST, esophageal stricture, COPD and chronic renal failure
Ashley Davidoff MD
Fabry Disease
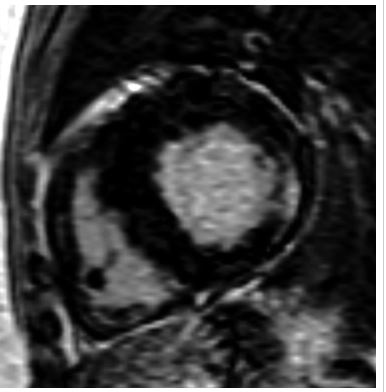
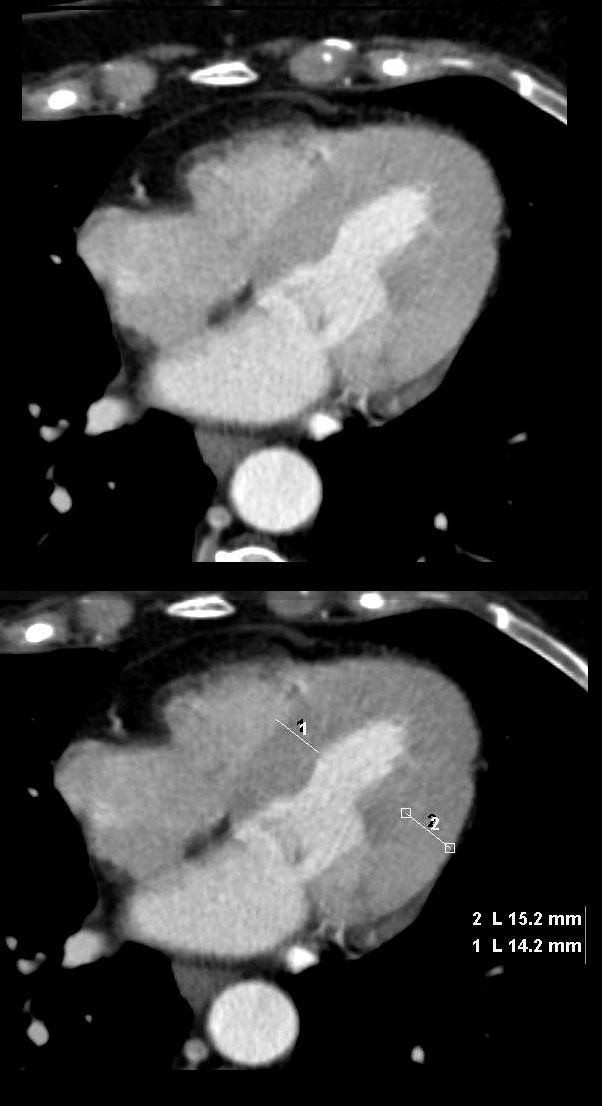
“Delayed enhanced images of 64-year-old heterozygotic woman with Fabry’s disease–related cardiac hypertrophy. Minimal thinning of basal segment of left ventricular inferolateral wall is associated with thick mesocardial striae of delayed enhancement shown on short-axis delayed enhanced images.”
De Cobelli et al Delayed-Enhanced Cardiac MRI for Differentiation of Fabry’s Disease from Symmetric Hypertrophic Cardiomyopathy
AJR Volume 192, Issue 3 2009

“40-year-old man with Fabry’s disease–related hypertrophy. Long-axis delayed enhanced images show typical pattern of delayed enhancement: thick striae involving inferolateral wall of basal segment of left ventricle in mesocardial distribution. Note sparing of subendocardial layer.
De Cobelli et al Delayed-Enhanced Cardiac MRI for Differentiation of Fabry’s Disease from Symmetric Hypertrophic Cardiomyopathy”
AJR Volume 192, Issue 3 2009
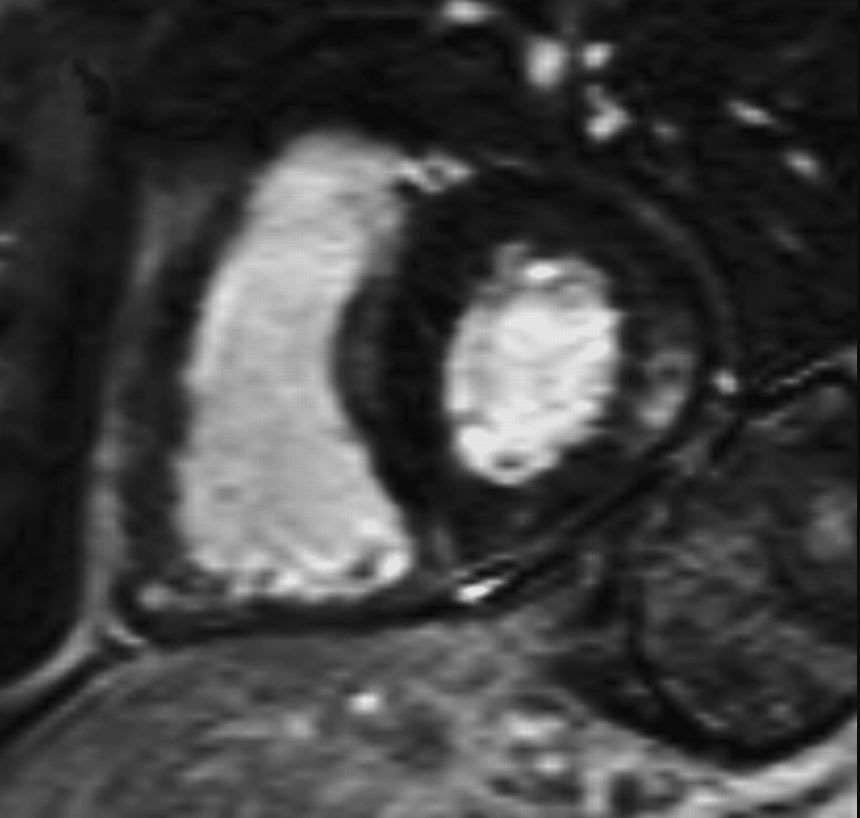
“40-year-old man with Fabry’s disease–related hypertrophy. Short -axis delayed enhanced images show typical pattern of delayed enhancement: thick striae involving inferolateral wall of basal segment of left ventricle in mesocardial distribution. Note sparing of subendocardial layer.”
De Cobelli et al Delayed-Enhanced Cardiac MRI for Differentiation of Fabry’s Disease from Symmetric Hypertrophic Cardiomyopathy”
AJR Volume 192, Issue 3 2009
References and Links
- TCV