
Ashley Davidoff
TheCommonVein.net 45309b06
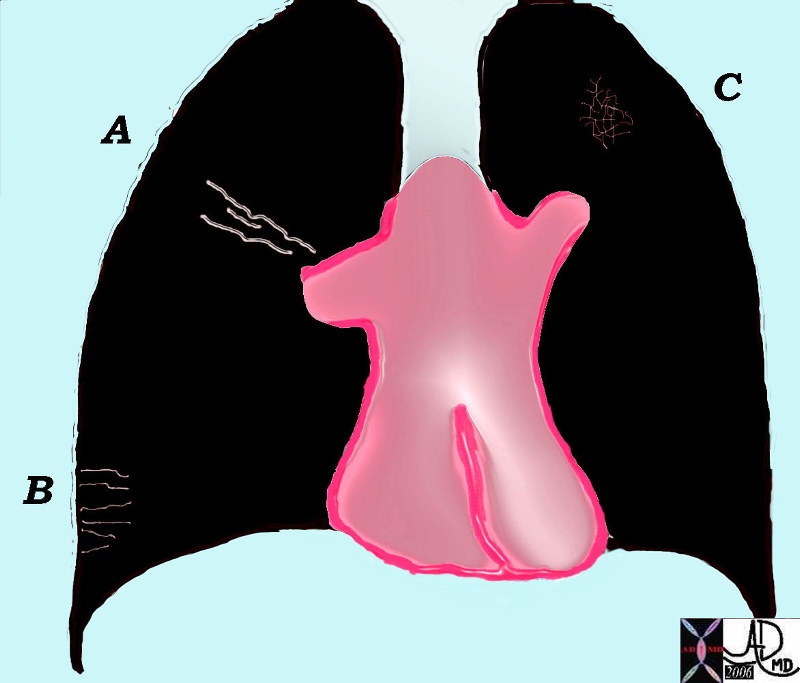
The Secondary Lobule
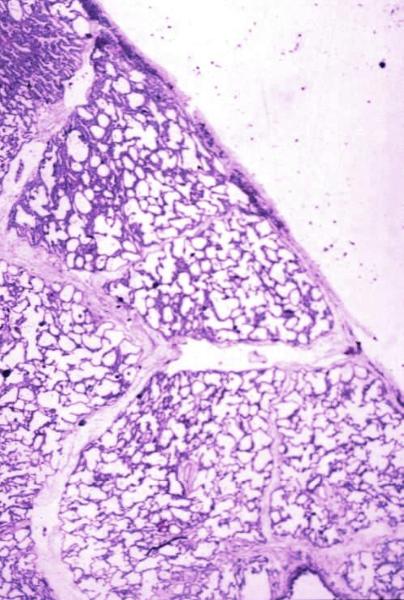
Normal lung histology
This image is a panoramic view of the lung showing secondary lobules and interlobular septa. Within the interalveolar septae, one sees small venules and lymphatics.Courtesy Armando Fraire MD. 32649b
code lung pulmonary alveoli alveolus secondary lobule interlobular septa vein lymphatic histology
interstitium interstitial
32649b
Interstitial Edema
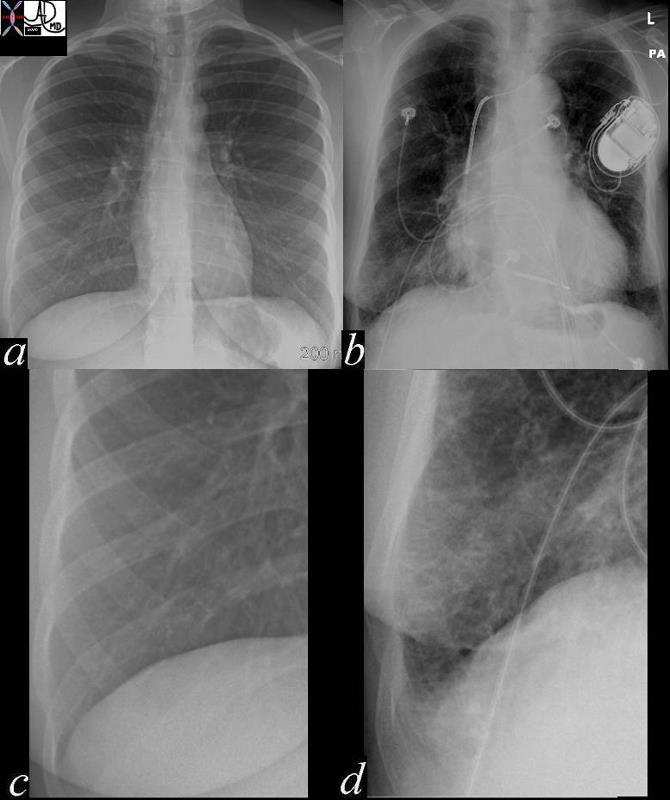
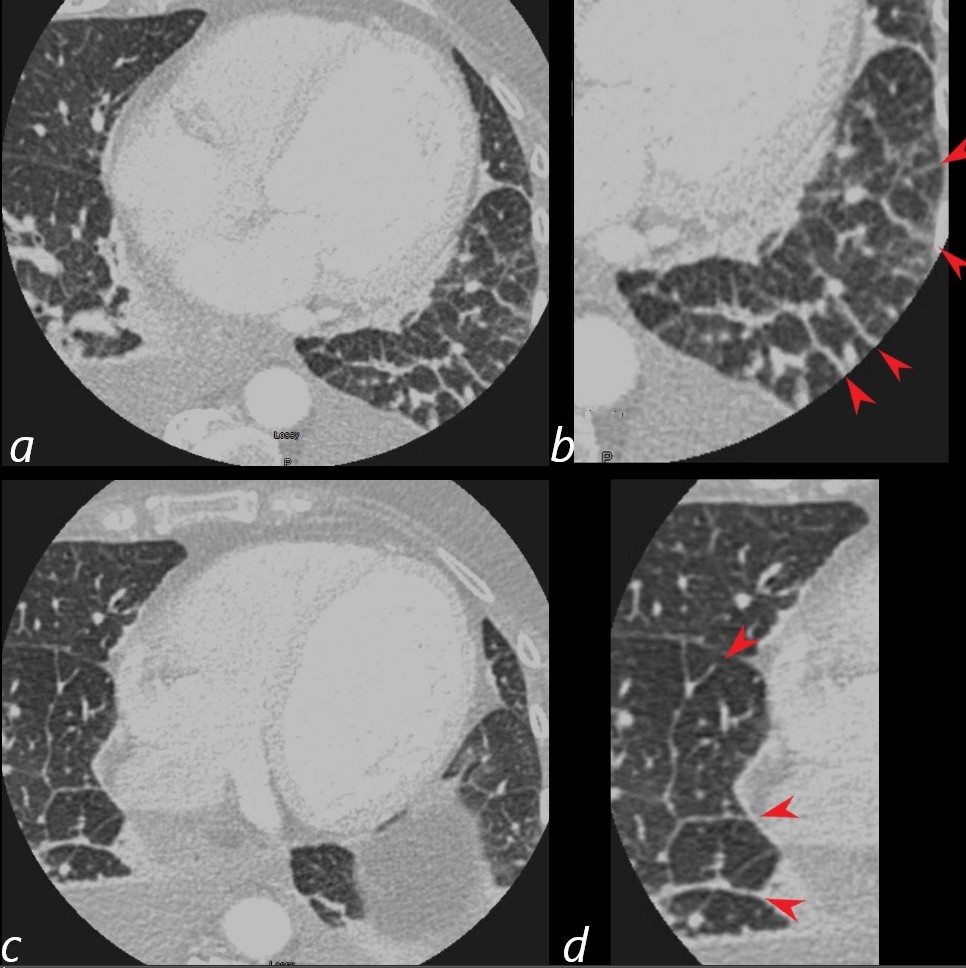
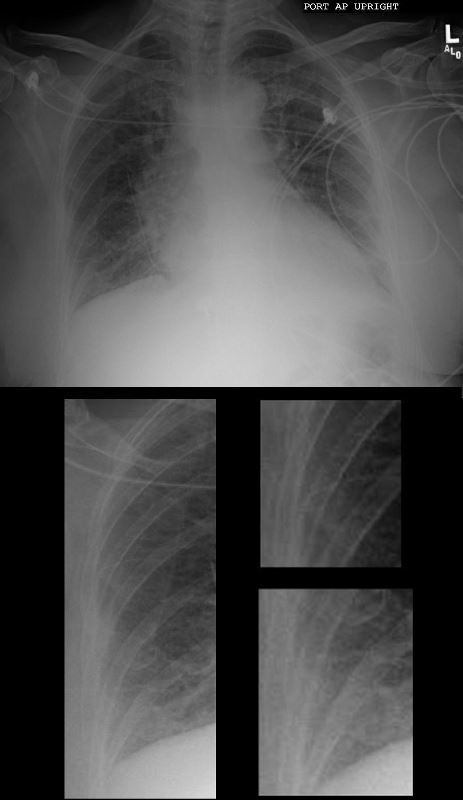
In these images. and c are normal and b and d represent thickened interlobular septa in a patient with congestive heart failure. These are the well known Kerley lines, often spoken about but rarely seen. They are identified as thin horizontal lines usually seen in the costophrenic angles, not being longer than 2 cms in length and touching the pleural surface.
42545c01.800 Ashley Davidoff MD
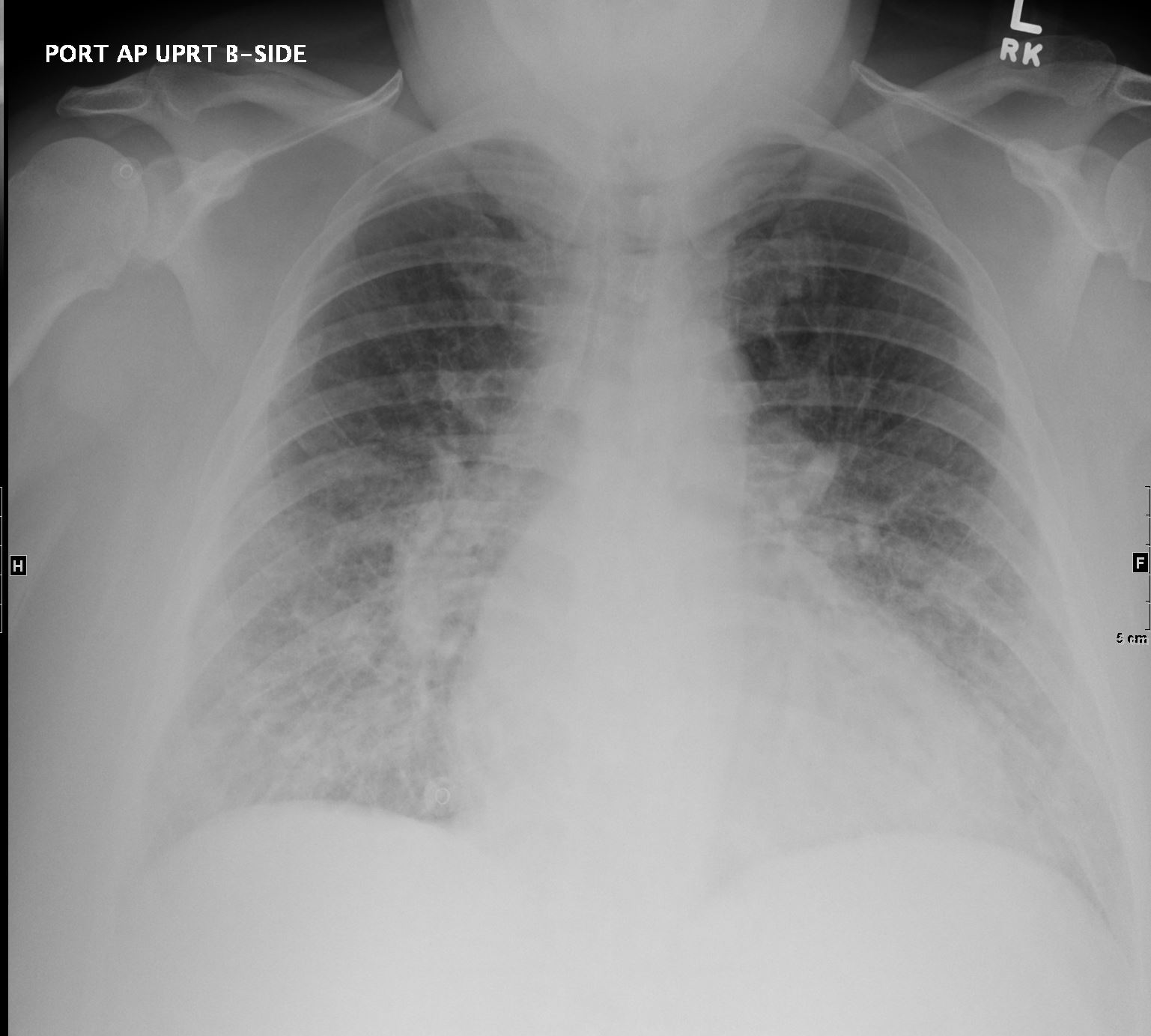
Portable CXR shows cardiomegaly with interstitial edema indicating moderate CHF
Ashley Davidoff
TheCommonVein.net
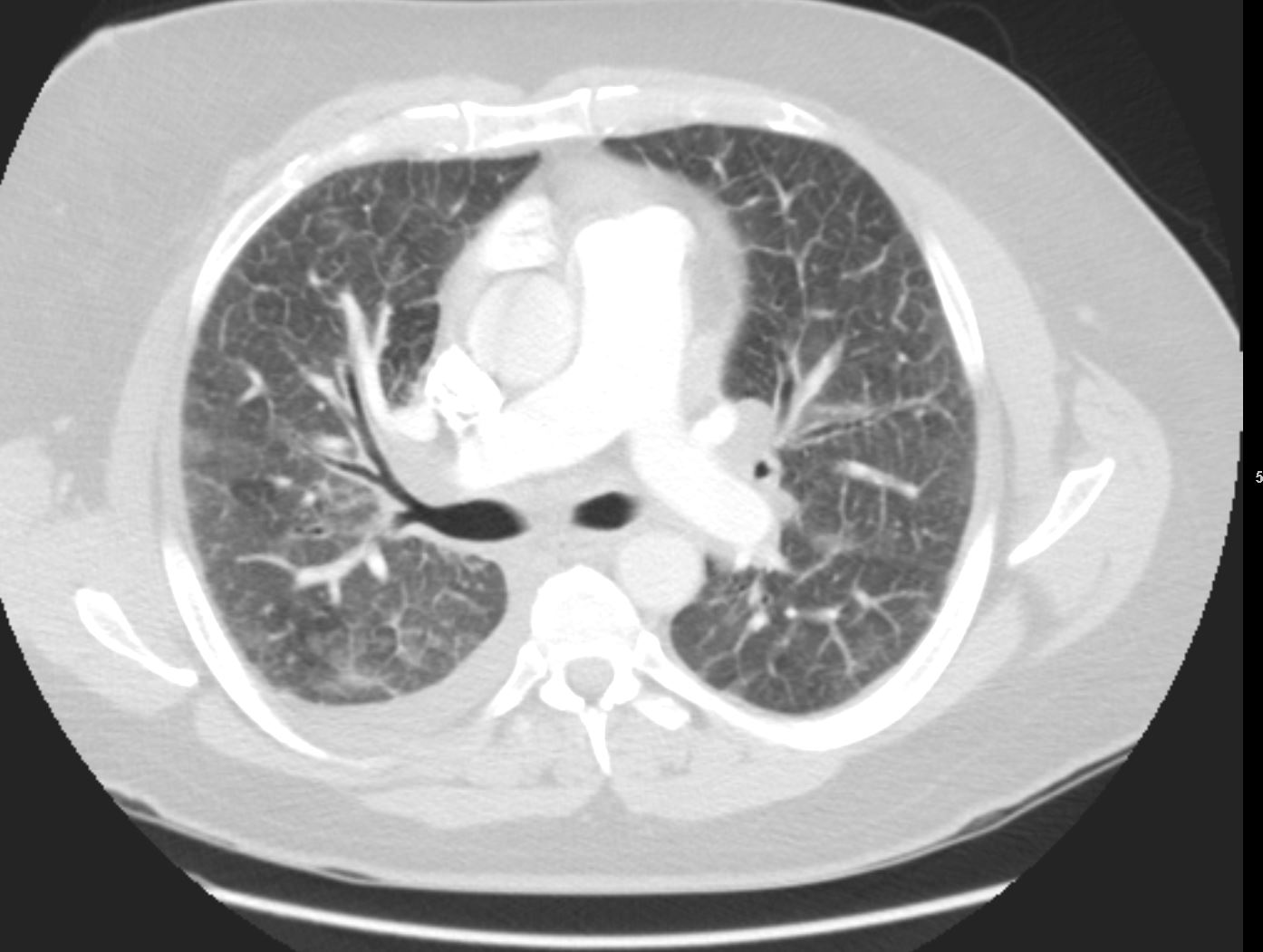
CT scan through the chest at the level of the MPA shows peri bronchial thickening, ground glass changes dominant in the RLL, extensive interlobular septal thickening and Kerley B lines
Ashley Davidoff
TheCommonVein.net

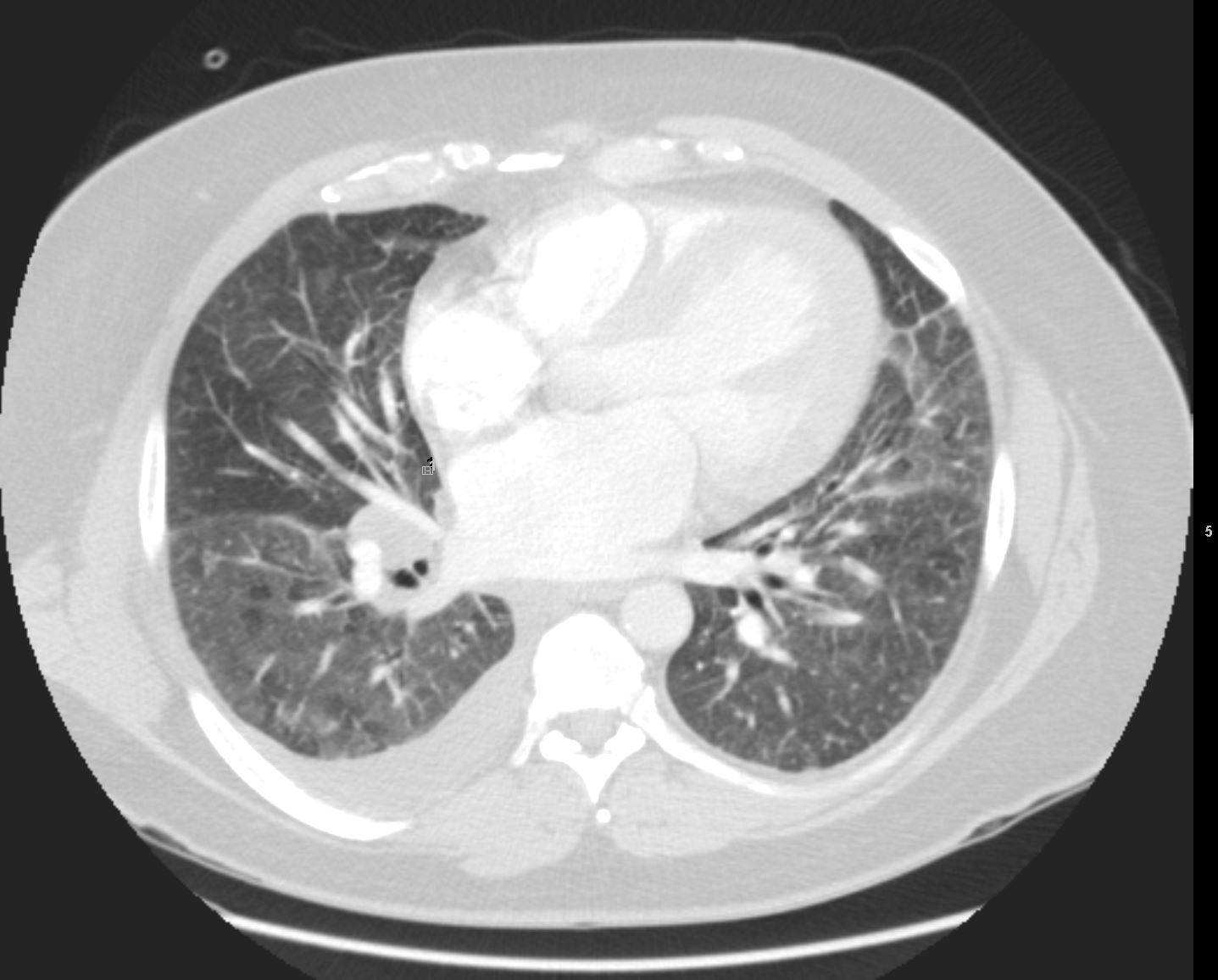
CT scan through the chest at the level of the RVOT shows, ground glass changes dominant in the middle lobe, extensive interlobular septal thickening and Kerley B lines
Ashley Davidoff
TheCommonVein.net
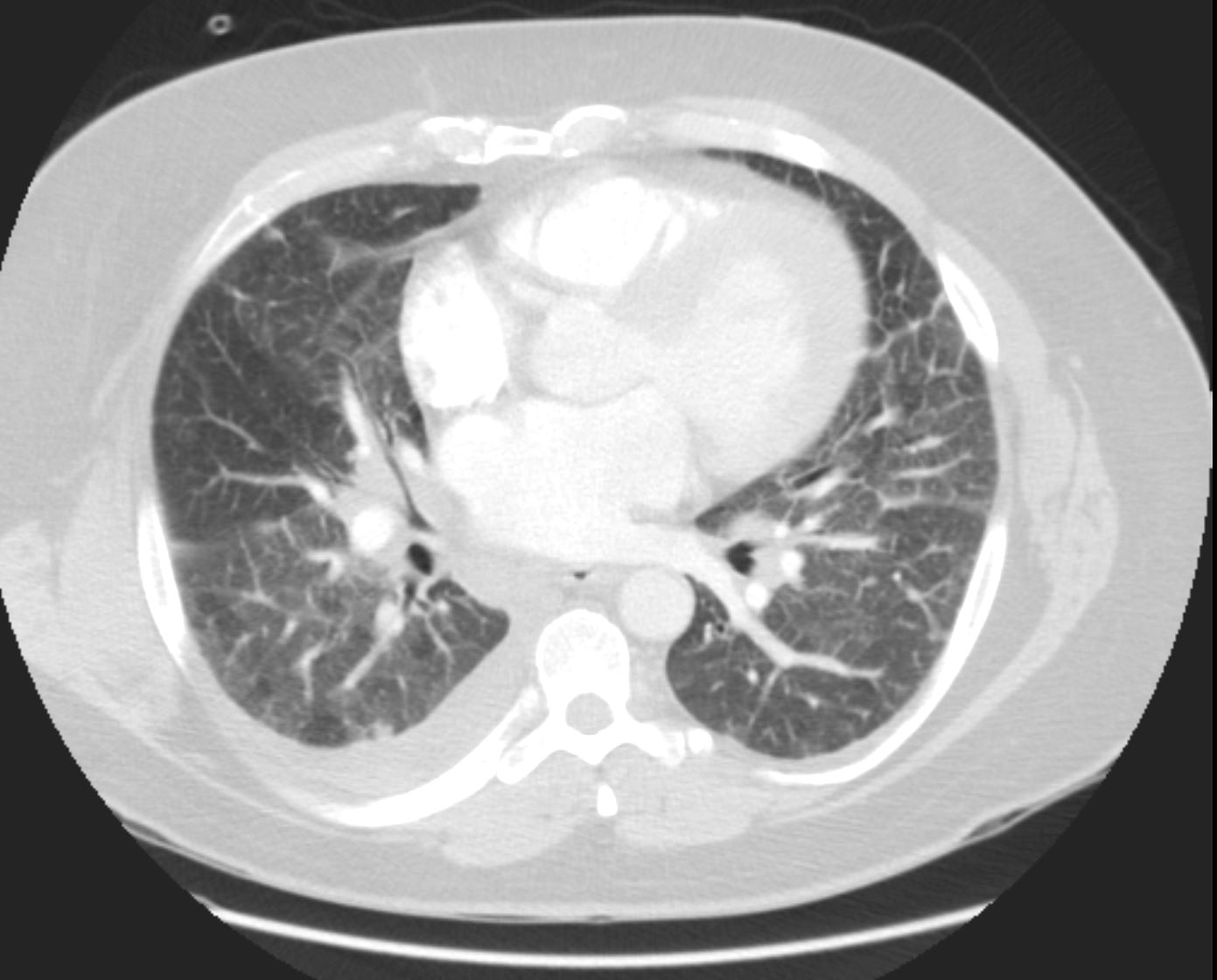
CT scan through the chest at the level of the left atrium shows, ground glass changes dominant in the lower lobes, extensive interlobular septal thickening, Kerley B lines, and mosaic perfusion abnormalities
Ashley Davidoff
TheCommonVein.net
CT scan through the chest at the level of the left atrium shows, ground glass changes dominant in the lower lobes, extensive interlobular septal thickening, Kerley B lines, and mosaic perfusion abnormalities
Ashley Davidoff
TheCommonVein.net
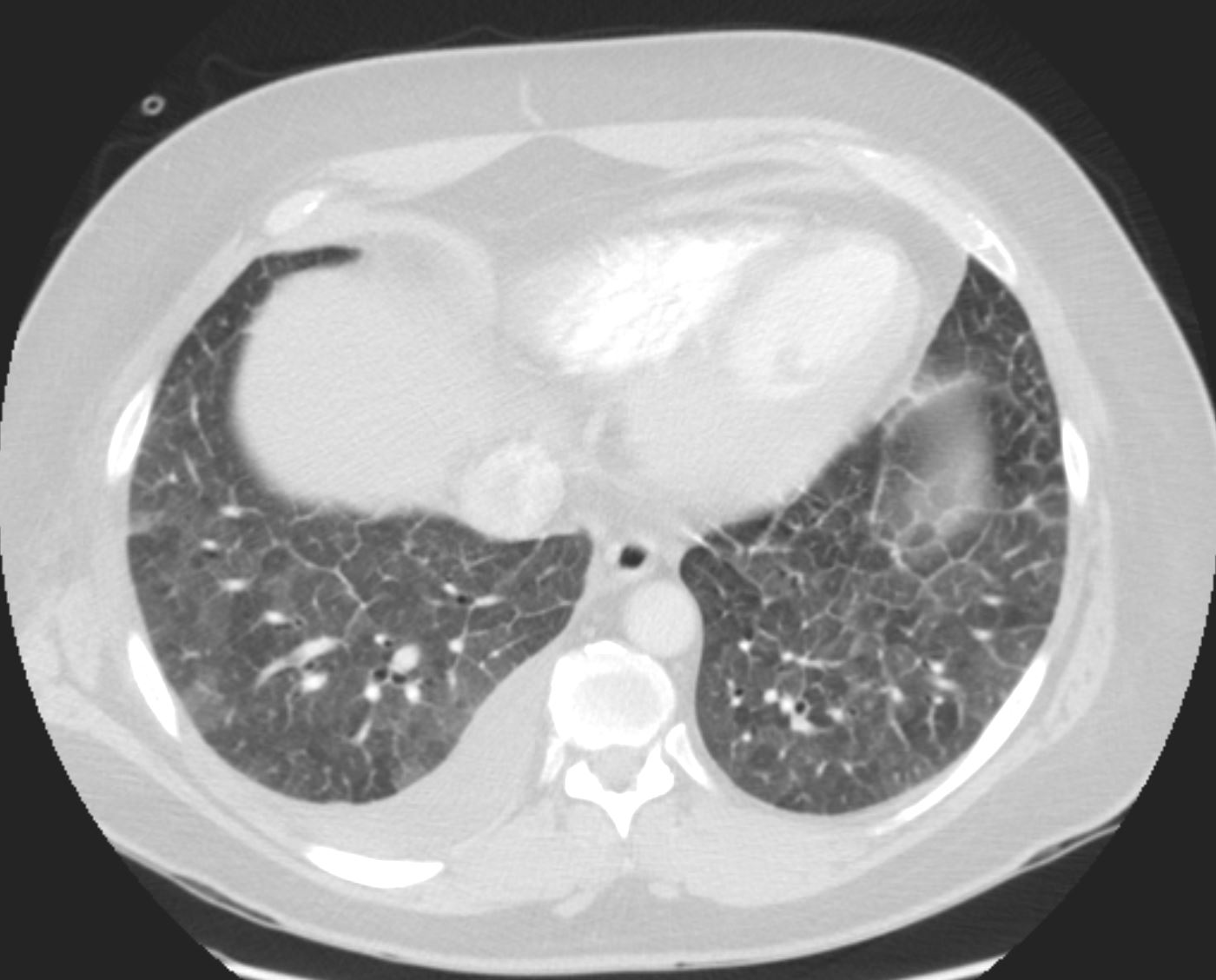
CT scan through the chest at the level of the left atrium shows, ground glass changes dominant in the lower lobes, extensive interlobular septal thickening, Kerley B lines, and mosaic perfusion abnormalities
Ashley Davidoff
TheCommonVein.net
Another Case of CHF
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Lung windows confirmed the presence of prominent interlobular septa and LAE with bilateral complex effusions.
Ashley Davidoff MD
Another Case of CHF
50-year-old male with CAD and CHF
The CXR showed LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left

CHF, INTERSTITIAL EDEMA KERLEY A and B
Ashley Davidoff MD
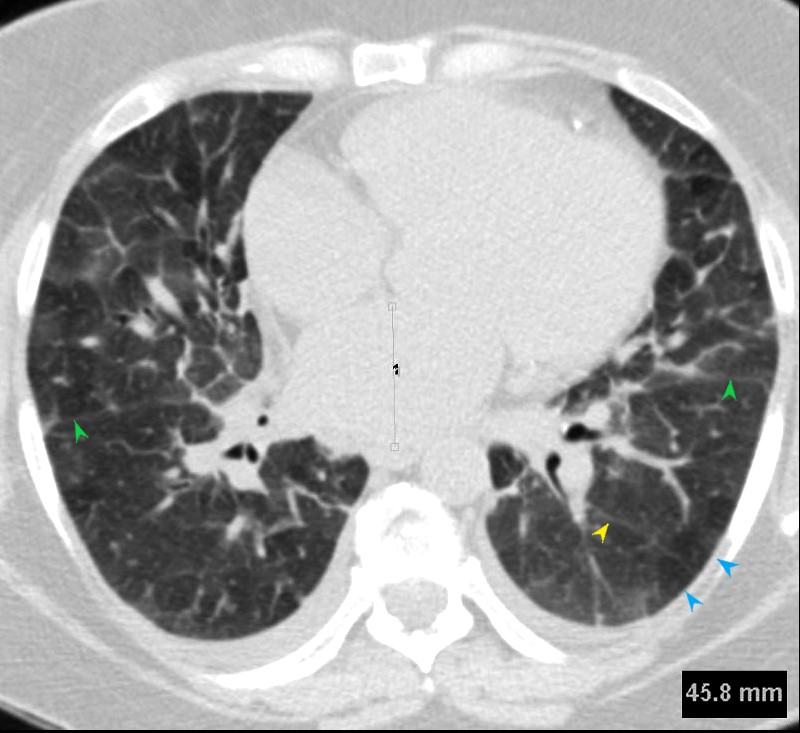
Fissures are indicated by the green arrows)
CHF, INTERSTITIAL EDEMA KERLEY A and B
Ashley Davidoff MD
Ashley Davidoff MD

Ashley Davidoff MD
50-year-old male with CAD and CHF
The CXR shows LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left
Ashley Davidoff MD

50-year-old male with CAD and CHF
The CXR shows LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left
Ashley Davidoff MD

CHF, INTERSTITIAL EDEMA KERLEY A and B
50-year-old male with CAD and CHF
The CXR shows LA enlargement with widening of the carina, and findings consistent with interstitial edema characterized by interstitial fuzziness, Kerley B lines and peribronchial cuffing
The CT shows a LA that is enlarged (4.4cms), heavy LAD calcification, diffuse ground glass changes with regions of sparing. thickening of the interlobular septa, Kerley A and Kerley B lines, and small bilateral effusions, right slightly greater than the left
Ashley Davidoff MD
Non Compaction Heart Failure and Pacemaker
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Ashley Davidoff MD

74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Ashley Davidoff MD
Kerley A Lines
Kerley lines including Kerley A and Kerley B Lines
- 2-6 cm long oblique lines
- <1 mm thick
- course towards the hila.
- thickening of the interlobular septa with
- lymphatic connections between the
- perivenous and
- bronchoarterial lymphatics
- chest Xray and CT
- cross normal vascular markings
- extend
- to the hilum from
- the upper lobes.

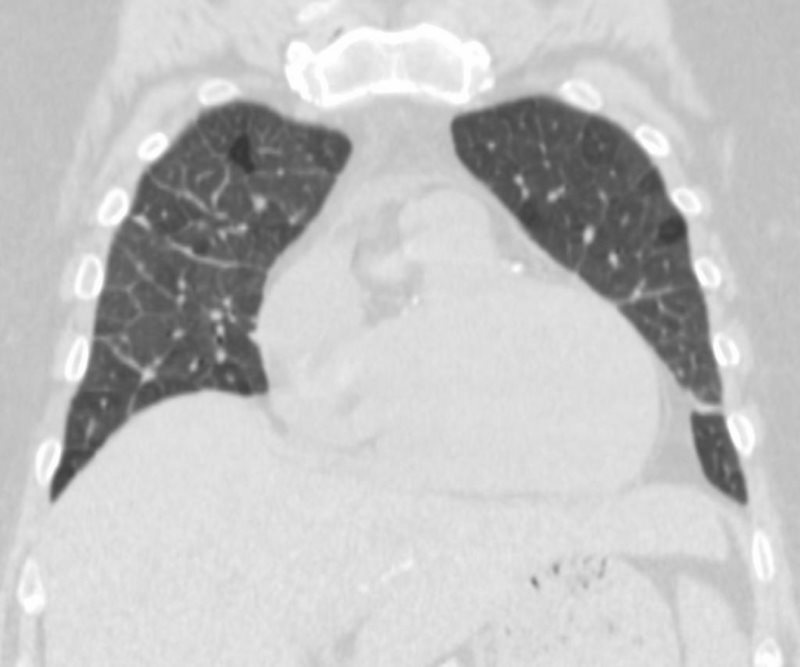
CT scan in the coronal plane through the chest at the level of the RV shows Kerley A lines
Ashley Davidoff
TheCommonVein.net
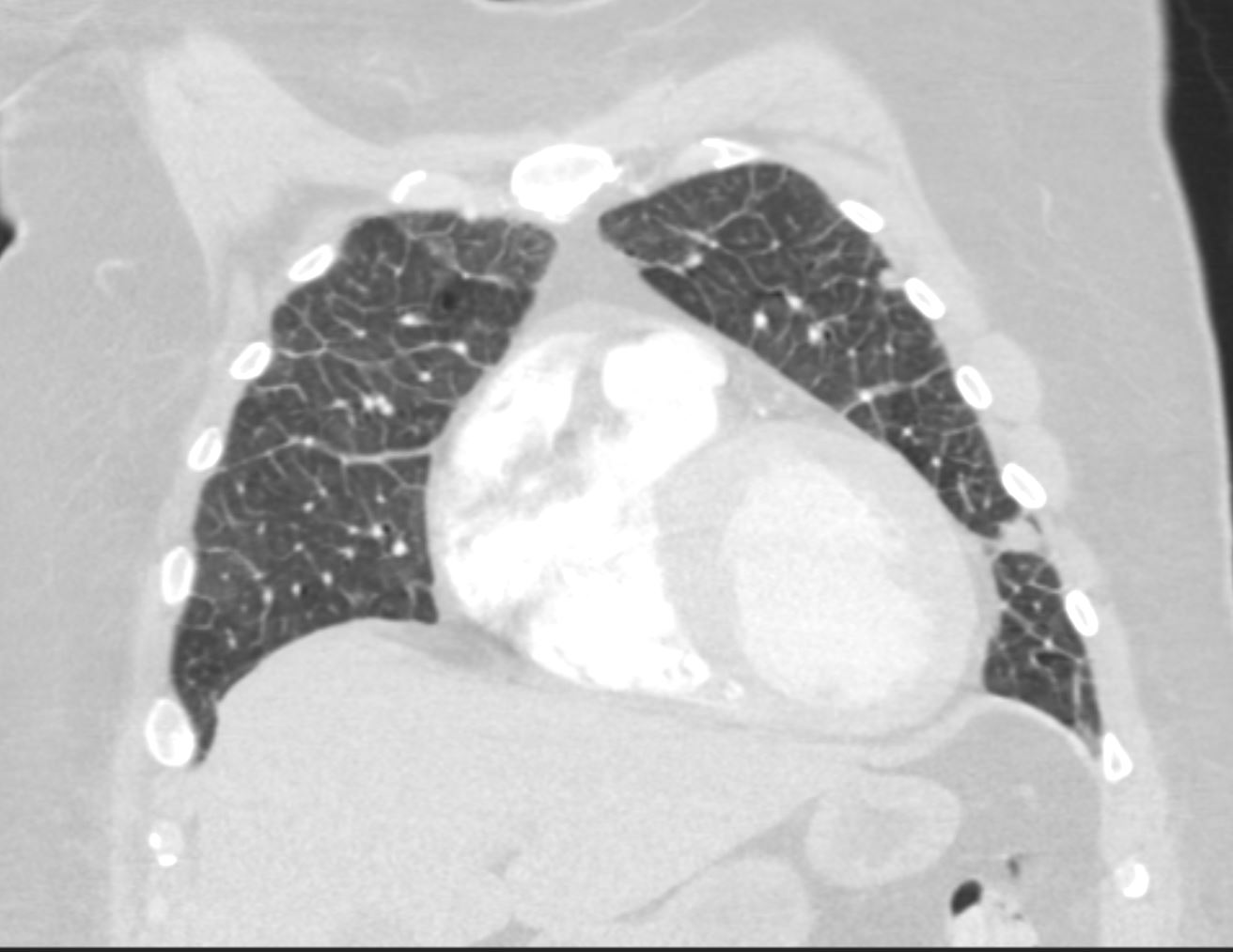
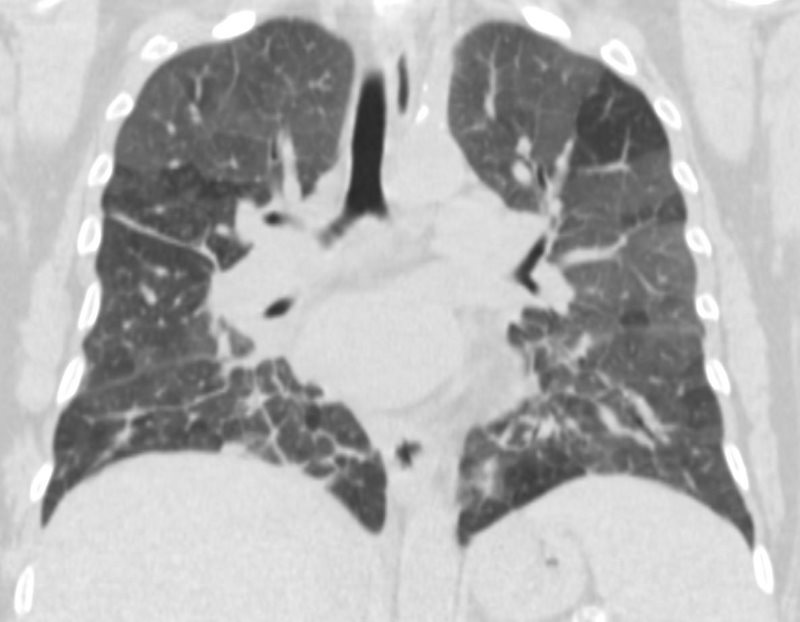
CT scan in the coronal plane through the chest at the level of the RV shows Kerley A and Kerley B lines
Ashley Davidoff
TheCommonVein.net
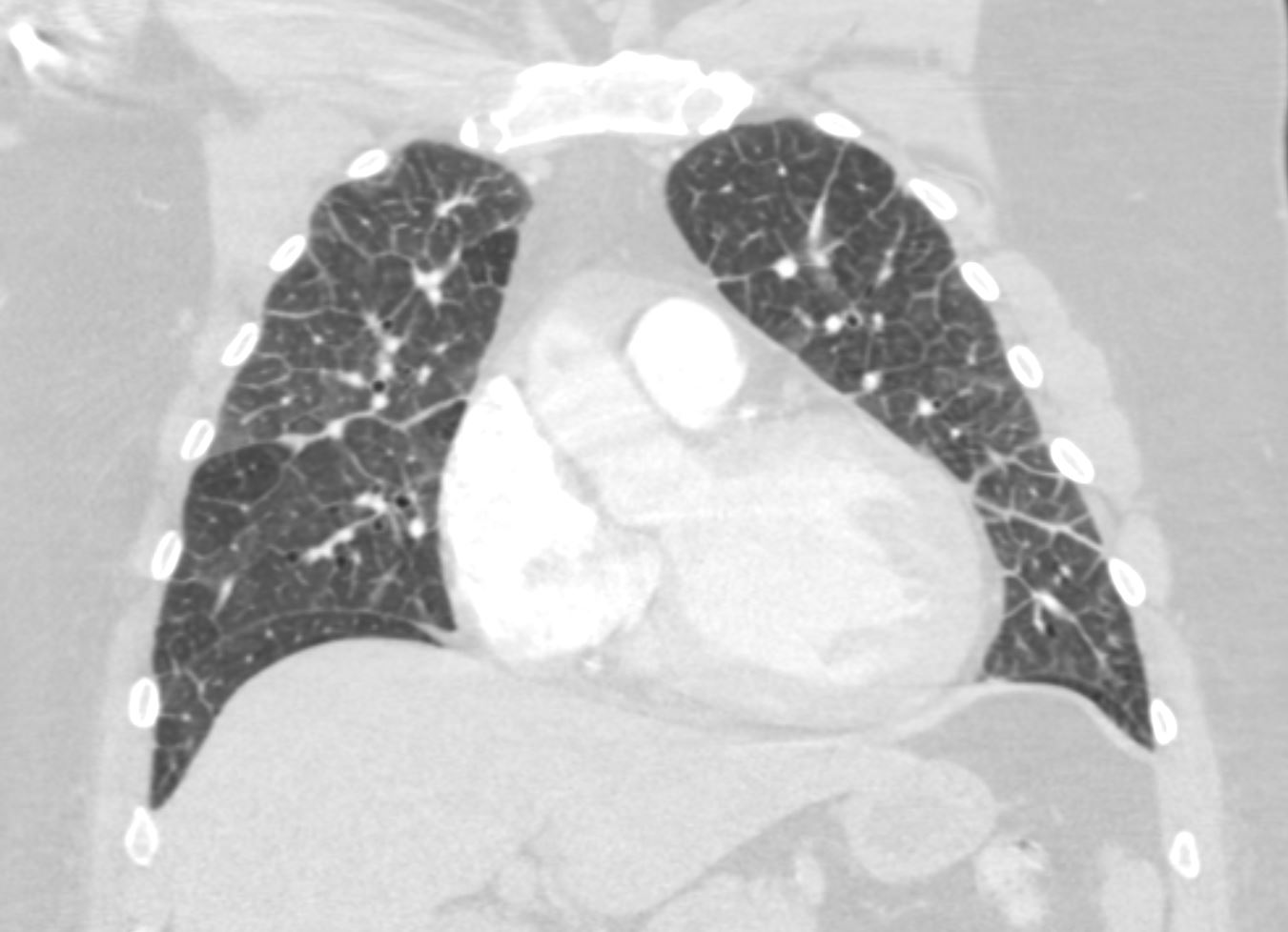
CT scan in the coronal plane through the chest at the level of the LV shows Kerley A lines and Kerley B lines with mild ground glass changes in the right upper lobe
Ashley Davidoff
TheCommonVein.net

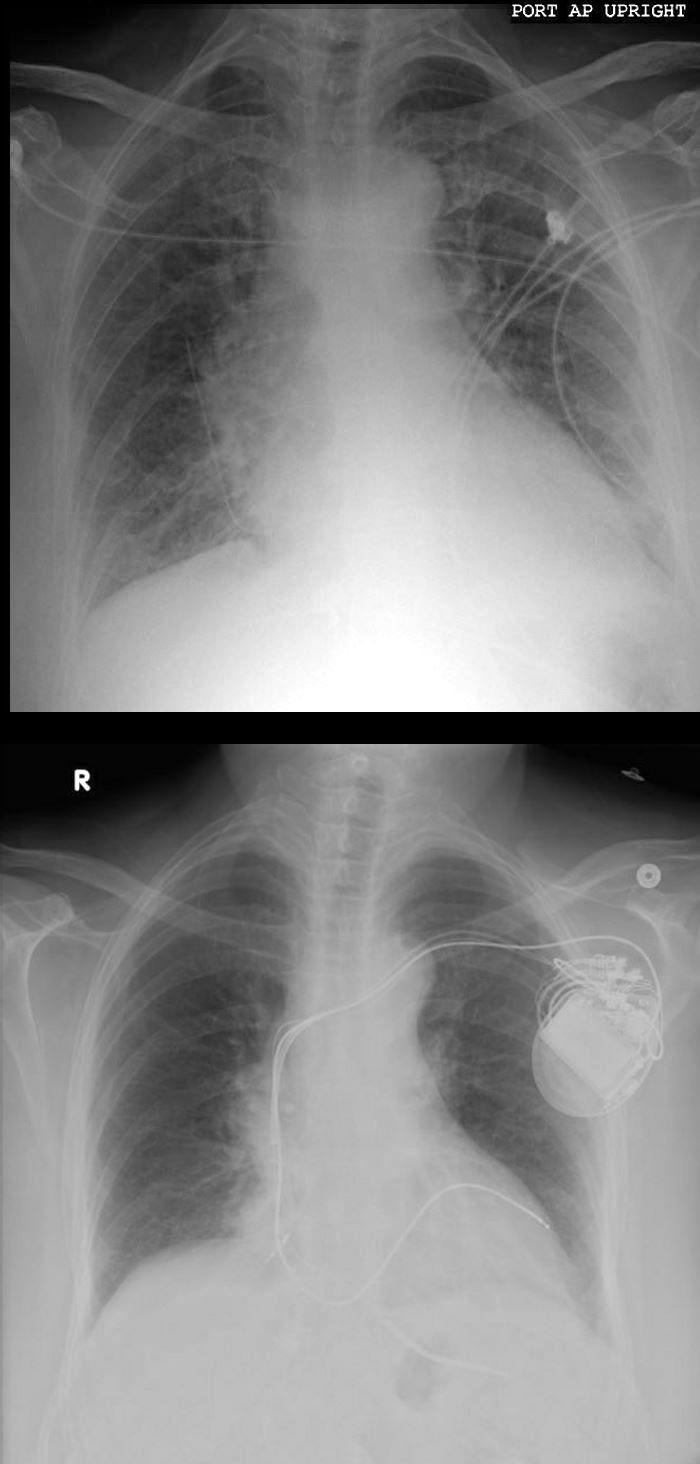
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Lung windows confirmed the presence of prominent interlobular septa and LAE with bilateral complex effusions.
Ashley Davidoff MD

74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Prior to implantation of a dual lead pacemaker she had a gated cardiac CT to define the venous anatomy.
The scout film shows an enlarged left atrium and suggestion of LV enlargement.
Lung windows confirmed the presence of prominent interlobular septa and LAE.
Axial soft tissue windows shows LAE with A_P dimension of 4.7cms (upper limits of normal is 4cms)
Ashley Davidoff MD
74-year-old female presents in CHF and an echo showing reduced EF (35%) and non-compaction.
Initial CXR shows findings consistent with interstitial edema, (redistribution, fuzzy borders of the vessels and descending RPA) Kerley B lines, and left atrial enlargement.
Volume measurements showed an end diastolic volume of 217mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Following placement of biventricular pacemaker CXR showed resolution of the heart failure, but persistence of the LAE.
Ashley Davidoff MD
In these images. and c are normal and b and d represent thickened interlobular septa in a patient with congestive heart failure. These are the well known Kerley lines, often spoken about but rarely seen. They are identified as thin horizontal lines usually seen in the costophrenic angles, not being longer than 2 cms in length and touching the pleural surface.
42545c01.800 Ashley Davidoff MD

74-year-old female presents in CHF and an echo showing reduced EF (35%) and non compaction.
Volume measurements based on the gated cardiac CT showed an end diastolic volume of 217 mls, an end systolic volume of 159ccs, a stroke volume of 58ccs with a resulting ejection fraction of 26%.
Ashley Davidoff MD
Kerley A Lines
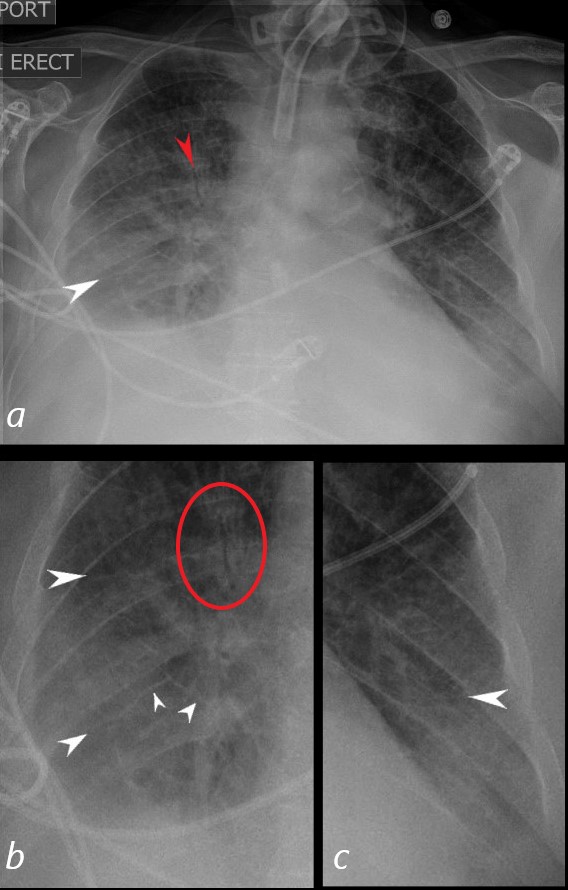
62-year-old male in the ICU with a tracheostomy with acute respiratory distress.
CXR shows acute alveolar edema with an air bronchogram in the right upper lobe (red arrow, a), and red circle, b)with Kerley A lines extending from the periphery to the hila and mediastinum (white arrows)
Ashley Davidoff MD
Kerley Lines L Base  Kerley Lines L Base
Kerley Lines L Base
Non Cardiogenic Kerley Lines

S/P RIGHT UPPER LOBECTOMY
S/P RIGHT UPPER LOBECTOMY
References and Links
TCV