
-
“ Clinical Applications of Coronary CT Computed Angiography:”.
- Wednesday, April 27, 2022 Zoom meeting
-
Introduction
- Good morning
- Honor
- Thanks
- Ravin –
- Go back along way
-
- Nail on the Head
- Two of the disciplines that have inspired me and made my career so rewarding
- Heart
-
- remarkable anatomy physiology
- Has intrigue adventure drama and romance
- Unlike the brain that just sits and thinks
- the heart moves -it has rhythm it has sound
- Shakespeare mentions it more than 1200 times
- We celebrate it and what it means to people every year on Valentine’s day
- My Teachers Go back a long way
- Ongoing pursuit to find the underlying principles that govern complexity
- Parts
- Size
- Shape
- Position
- Character
- Time
- The Common Vein
- Whichever technology is able to fulfill these elements wins the prize
- And I believe it is CT(at least for the diagnosis of CAD) and and I hope to convince you too
- Ongoing pursuit to find the underlying principles that govern complexity
-
- CT scan and I also go back a long way
- were born just 6 years apart
- Nail on the Head
-
- It was advent of CT and its application that inspired me to
- hang up my triple headed Tycos

Ashley Davidoff thecommonvein.net Davidoff art #CXR #stethoscope heart0012-

Acknowledgement Philips Medical Systems
At the time the perception of radiology was that
Working in a Dark Room
Subjectivity Dominated
But even in that world it gave birth to people like Dotter, Seldinger and Judkins
However it was my introduction to CT that sold Radiology to me
Nietsche – German philosopher
Believer in Perspectivism
Mother in Law Rosalie Fisher – Physicist
Looking at the the Pixel/Voxel from Many Angles
8 centimeters of coverage, with the entire heart covered in two scans The rotation speed is 0.27 seconds (total .54 seconds with 120 kw of power.
Now available 640 rows and in .27 secs we scan the whole heart in one rotation
Ashley Davidoff thecommonvein.net
Gave numbers to the pixels
(just like the the 0 and 1 of computer science)
Enabled Objectivity – Ability to Accurately Measure
Applying the Segmental Approach to Complex Structures
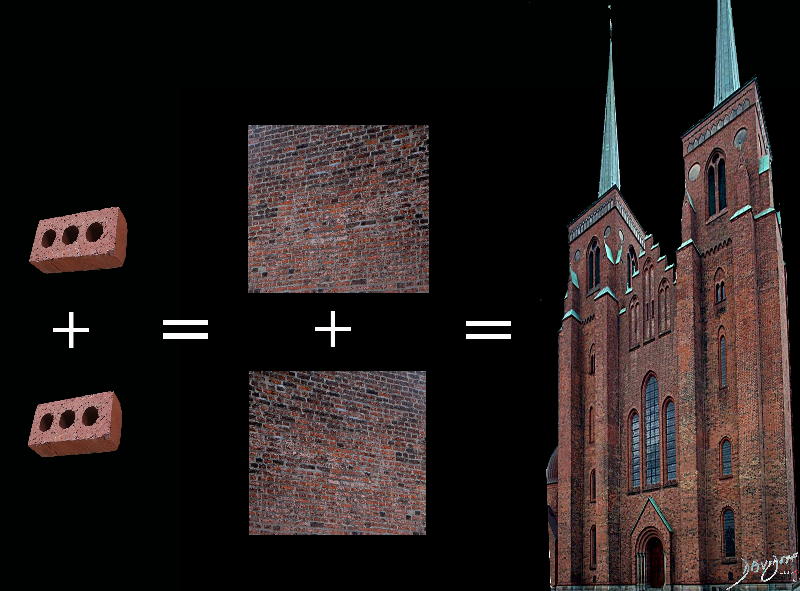
It is Nothing by Itself However the Whole is Only as Strong as the Weakest Brick
By Ashley Davidoff MD TCV-0039 TheCommonVein.net
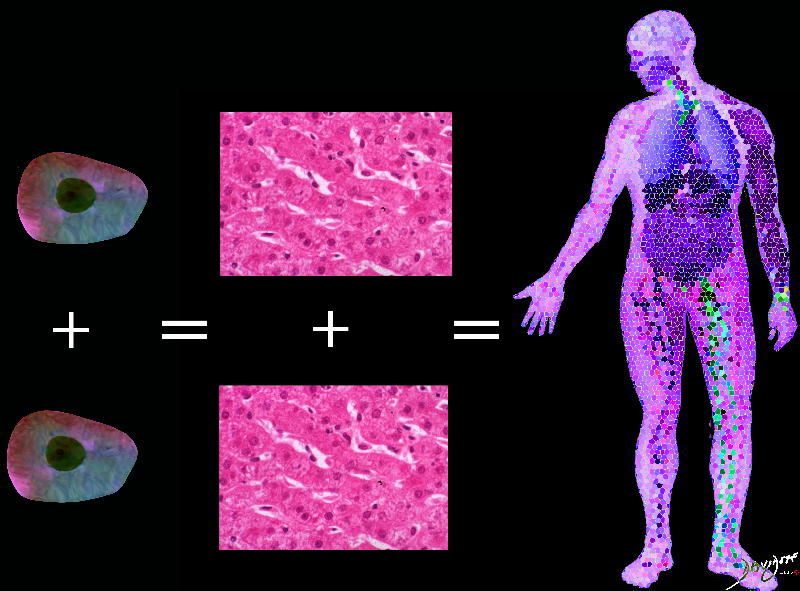
TCV-0040 TheCommonVein.net
So for example looking at these liver cells
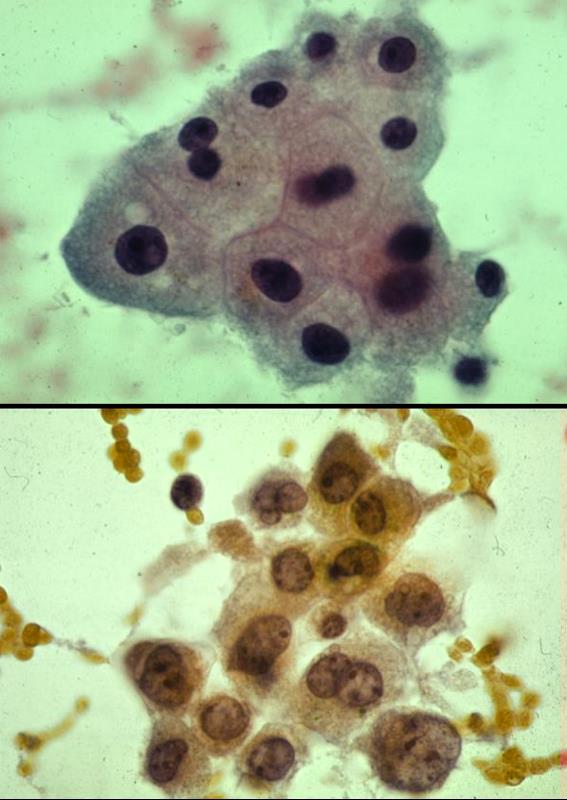
Cell Size 10 to 100 µm
And most of the time in clinical practice we use subjectivity

Ashley Davidoff MD
thecommonvein.net
#subjectivity#Davidoff art #principles#character #diagnosis
character-0003
and on that basis we give the structure under evaluation
In the world of digital technology the cell = the pixel/voxel = about 1mm
The pixel has a number embedded within it
Once we have data in pixel form we can manipulate the data and this is the strength of digital acquisition
Ashley Davidoff MD
thecommonvein.net
This methodology is therefore able to provide objectivity, enabled by better measurement provided by better tools (computer algorithms)
Ashley Davidoff MD
thecommonvein.net
- CT scan
- because of the nature of its acquisition
- it has the element of objectivity
Familiar to all is the Hounsfield Number relating to the density

Ashley Davidoff MD thecommonvein.net
Blooming Artifact

The small calcified plaque in the top left image is an artistic version of the reality – calcified plaque that does not impinge on the lumen. The top right image is a CT in the ideal world recreated within the grid of pixels (voxels in 3D) The calcified plaque (white arrow) which shares a voxel space with the blood in the lumen) remains distinct and true to its size, demonstrating true lack of impingement on the lumen
The bottom row in gray scale shows what happens in a CT scan. The bottom left image shows what the CT would look like ie impingement by the plaque on the lumen. The bottom right explains the blooming artifact. The calcium of very high density (about 500HU) shares the voxel space with the blood which is soft tissue density (about 50 HU) and so the net density is about 450 HU. The voxel does not therefore reflect a true density and the lesion therefore appears to impinge on the lumen when, in actuality it does not. This is called the blooming artifact
Ashley Davidoff MD thecommonvein.net
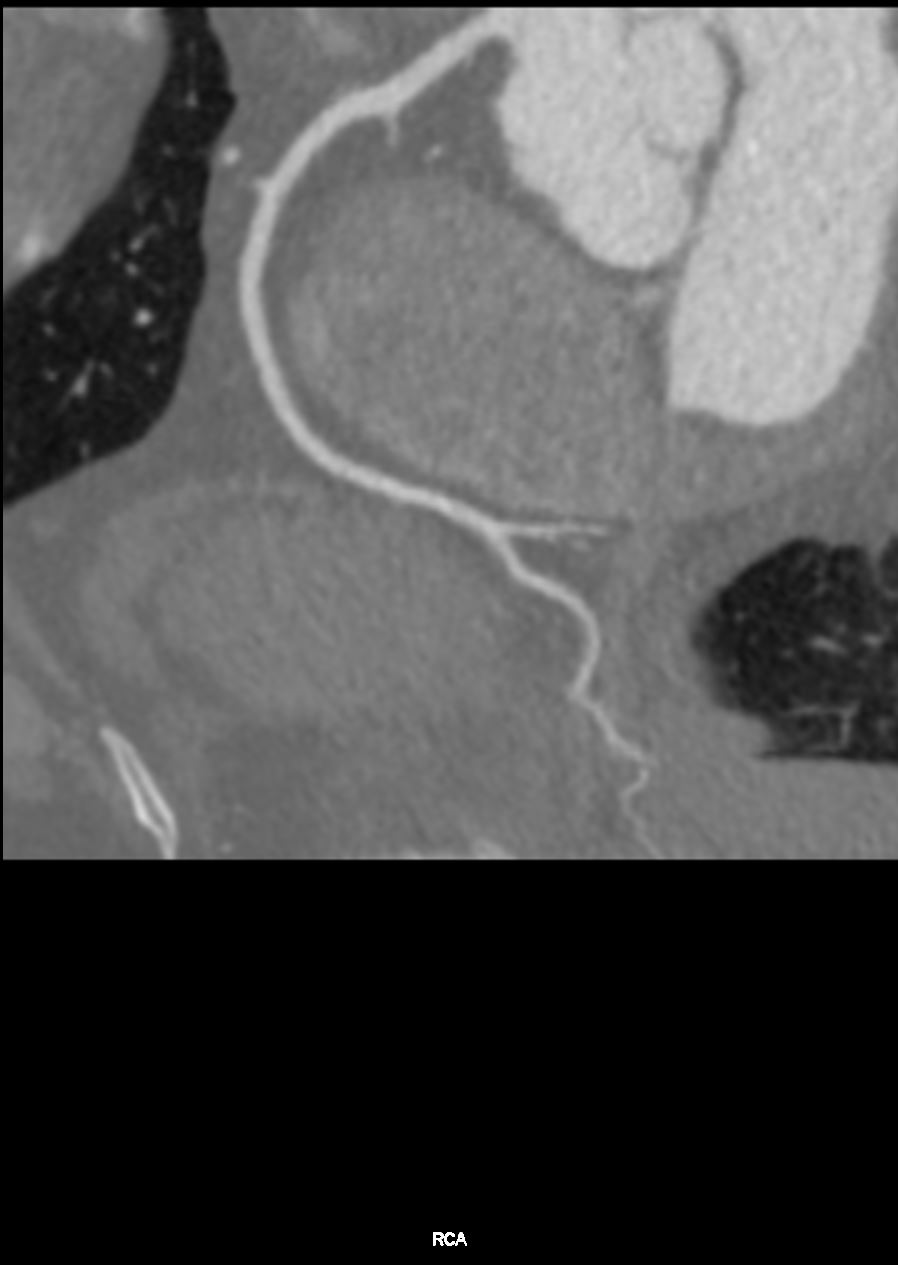
At the Vessel Level
- Coronary Artery
- diameter 3-4mm
- wall thickness ranges from 0.55 to 1.0 m
- intima and adventitia.2mm – .3mm
- … and the vessels is moving

Ashley Davidoff MD thecommonvein.net
Subjectivity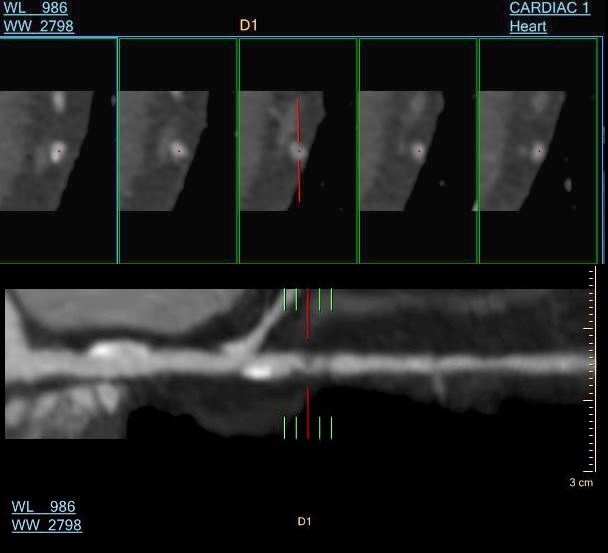
Consensus in the Trials
- ACCURACY, Core-64 multicenter Study, CONFIRM Study, PROMISE Study, SCOT Heart Study Summary
- revealed that we had a tool with high sensitivity and low specificity
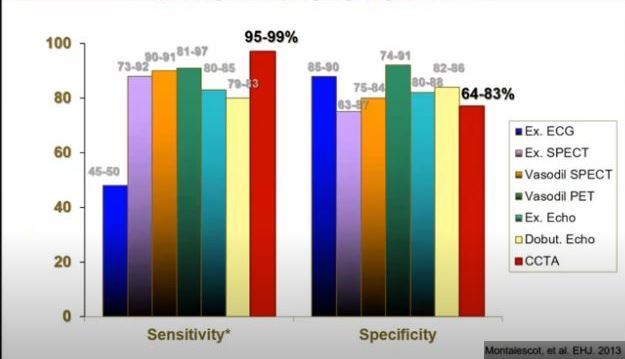
Montalescol et al
EHJ 2013
- However over over the last 10 years or so we have developed new tools that are able to enhance and better use the information within the voxels which are
- readily applied because of the innate and sound basis of the digital acquisition of the information
- Advances include
-
- improved resolution
- reduced radiation
- faster times of acquisition
- computational algorithms that are able to
- infer function from structure (FFR CT )
- methodology to characterize the tissues in the arterial wall
-
using the digital information inside the voxels
The New Tools – “Game Changers”, “Paradigm Shift”
- Faster Acquisition –
- 256 to 320- 640 detectors
- 640-slice CT scanner can image the entire heart in less than one third of a second
- 256 to 320- 640 detectors
-
- 640 slice CT scanner uses 80% less radiation
- Computerized Algorithms and AI
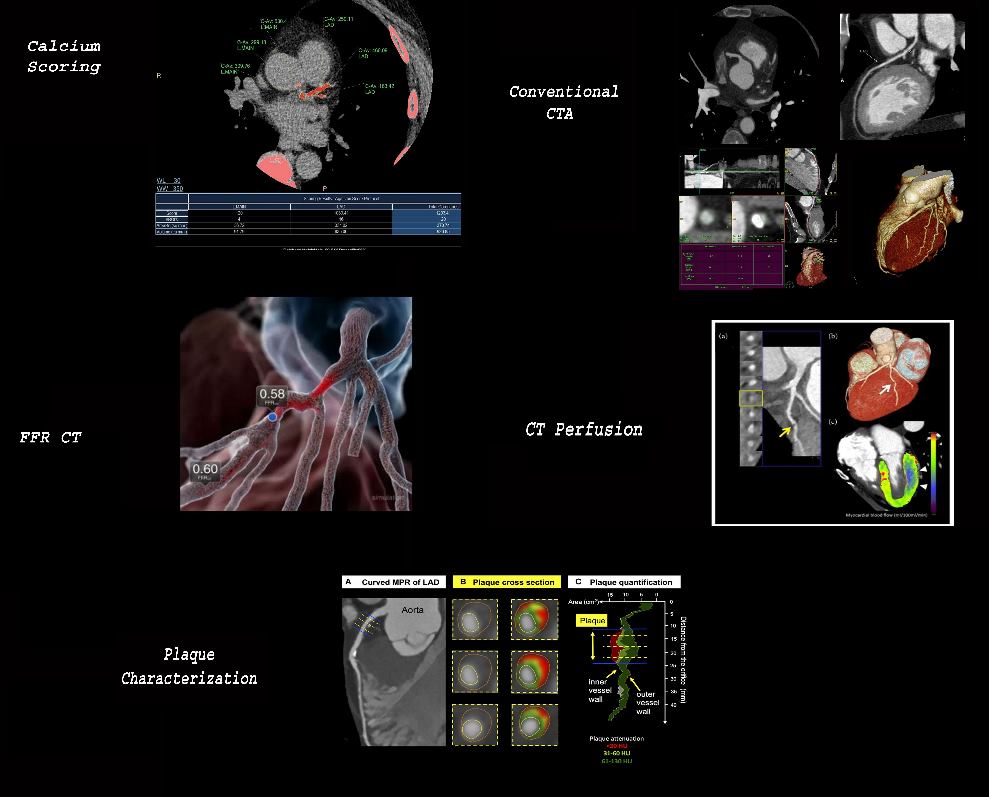
One Stop Shop – Calcium score, Coronary CTA, FFR CT, CT Perfusion, and Tissue Characterization
Calcium Score and Coronary CTA
- Acceptance and Recommendations by the Societies
- Class 1 recommendations
- 2016 Britain
- 2019 Europe
- ESC guideline
- 2021 US
- Class 1 recommendation
- patients with stable and acute chest pain
- (Narula J, et al 2021 Expert Consensus Document)
- Class 1 recommendation
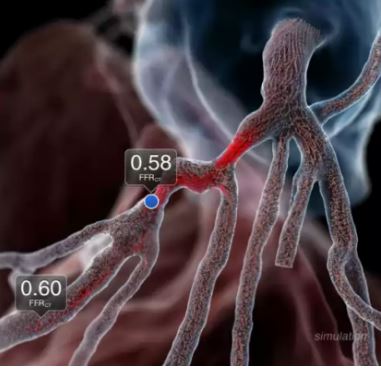
Fractional flow reserve derived from CT – FFR CT
- Normal = 1.0
- Abnormal <0.75-0.80
- generally considered to be associated with myocardial ischemia
Diagnostic and Interventional Cardiology
https://www.dicardiology.com/article/study-demonstrates-accuracy-noninvasive-ct-ffr-evaluating-cad-patients
CT Perfusion
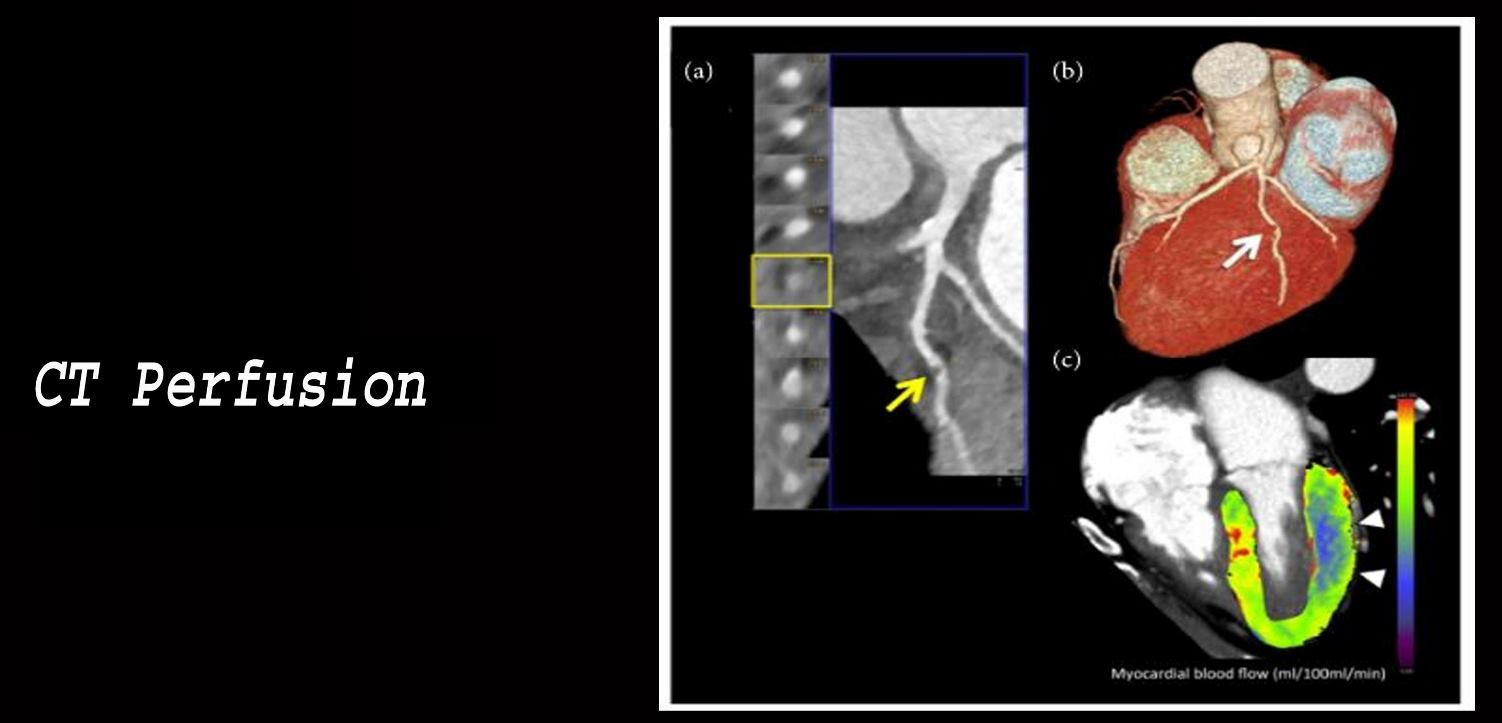
- CT Perfusion
- Core 320 Study Summary
- core 320 study Pub Med Link Full Text
- PERFECTION Study
- PERFECTION Study CTp vs FFR CT (Pub Med)
- Core 320 Study Summary
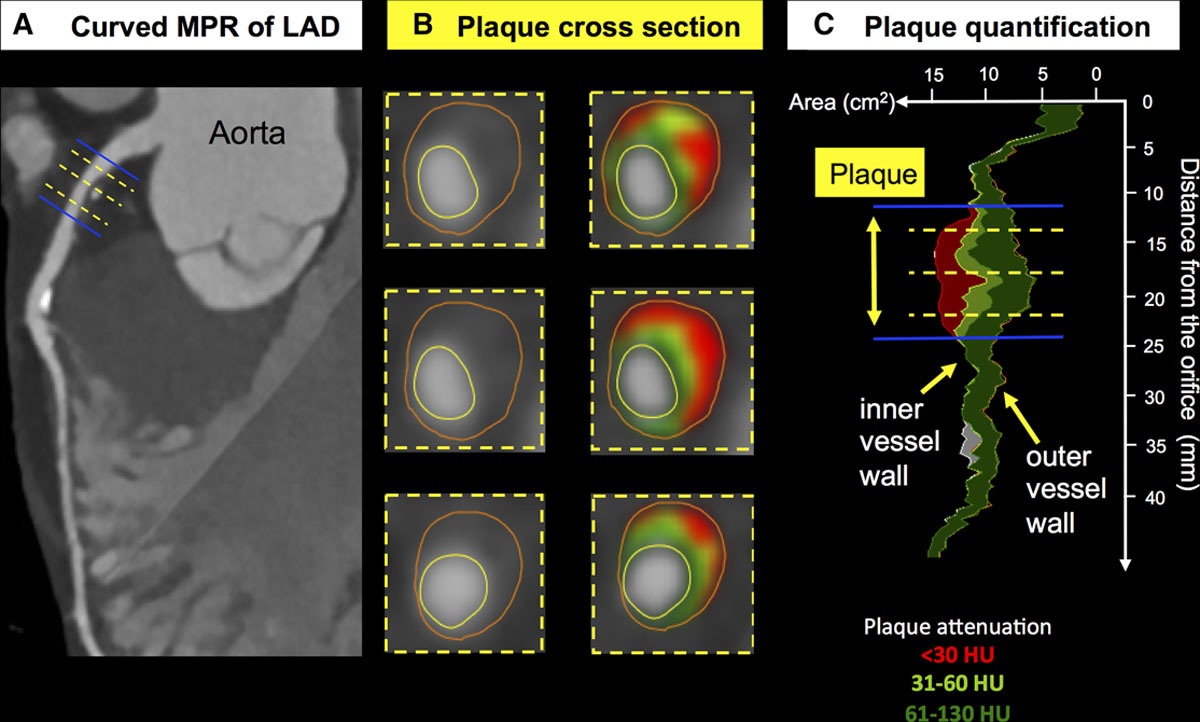
Plaque Characterization
 Bittner D et al Coronary Computed Tomography Angiography–Specific Definitions of High-Risk Plaque Features Improve Detection of Acute Coronary Syndrome
Bittner D et al Coronary Computed Tomography Angiography–Specific Definitions of High-Risk Plaque Features Improve Detection of Acute Coronary Syndrome
Results From the ROMICAT II Trial
Circulation Cardiovascular Imaging Vol 11 No.8 Coronary
-
- Abdelraman et al JACC 2020
- What we have learned is that we should approach
- Chest Pain – like we approach
- OA
- ie as a mostly a chronic illness
- We must approach Acute MI for its sneak attack methodologies
- high suspicion for a hidden enemy
- like pathological fracture
Understanding of atherosclerosis
History of Atherosclerosis
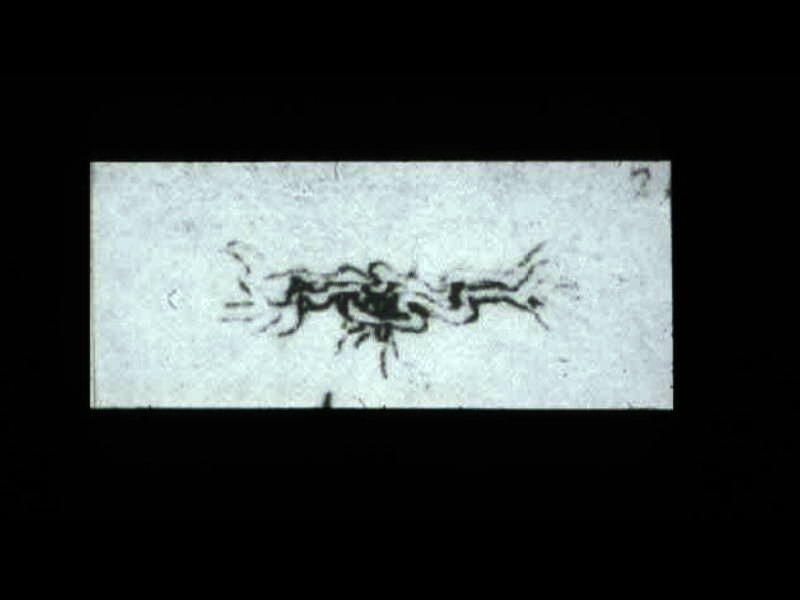
This is a drawing of the “meseraic vessels” – presumably the celiac axis. Da Vinci was able to interview and perform an autopsy on a centenarian. He describes the desiccated and tortuos state of the vessels of this patient accurately depicting the atherosclerotic process. He describes the narrowed lumen and the consequences of poor blood flow.The translation of da Vinci’s text accompanying this one inch image is remarkably insightful and pioneering. (see atherosclerosis hisrorical da Vinci) 13045b
“….acquire so thick a covering that it contracts the passage of the blood .”
“I have found there stones in the vessels”
“The tunics of the vessels behave in man as in oranges, in which the peel thickens and the pulp diminishes the older they become. And if you say that it is the thickened blood which does not flow through the vessels, this is not true, for the blood does not thicken in the vessels because it continually dies and is renewed.”
Ashley Davidoff MD
32628c
#aorta #normal intima#intima

Courtesy: Henri Cuenoid, M.D.
Atherosclerosis

Ashley Davidoff MD
thecommonvein.net
Ashley Davidoff MD
thecommonvein.net
The Fatty Plaque with thin cap and neovascularity is a land mine waiting to explode
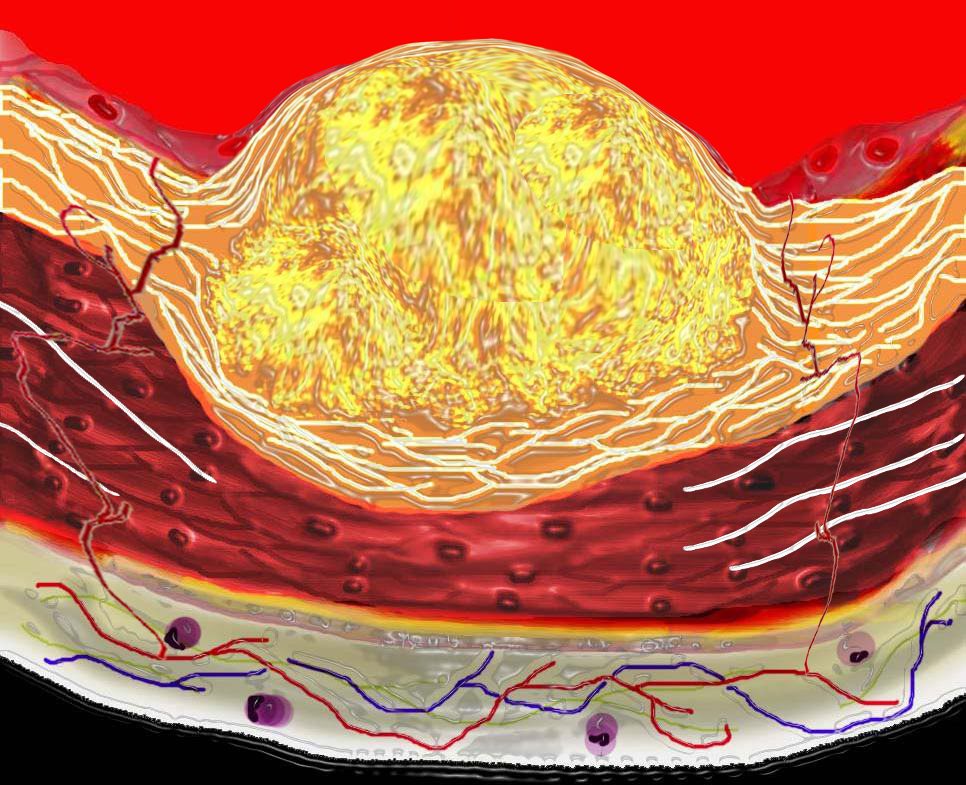
The Vulnerable Plaque

This diagram shows denudation of the endothelial layer with exposure and rupture of the contents of the atherosclerotic plaque in volcanic fashion into the lumen. This event is catastrophic and can result in acute thrombosis and may even be a fatal event. 33801d Courtesy Ashley Davidoff MD. code heart artery atherosclerosis atheroma vulnerable plaque drawing Davidoff art
Ashley Davidoff
thecommonvein.net
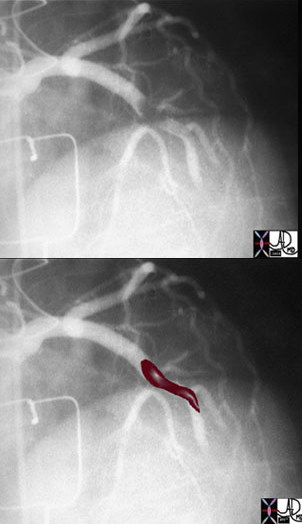
The above image of this cardiac catheterization shows a coned down left anterior oblique (LAO) projection of the LAD in a patient with acute thrombosis of the left anterior descending artery. In the lower image, the thrombus in the artery is overlaid in maroon.
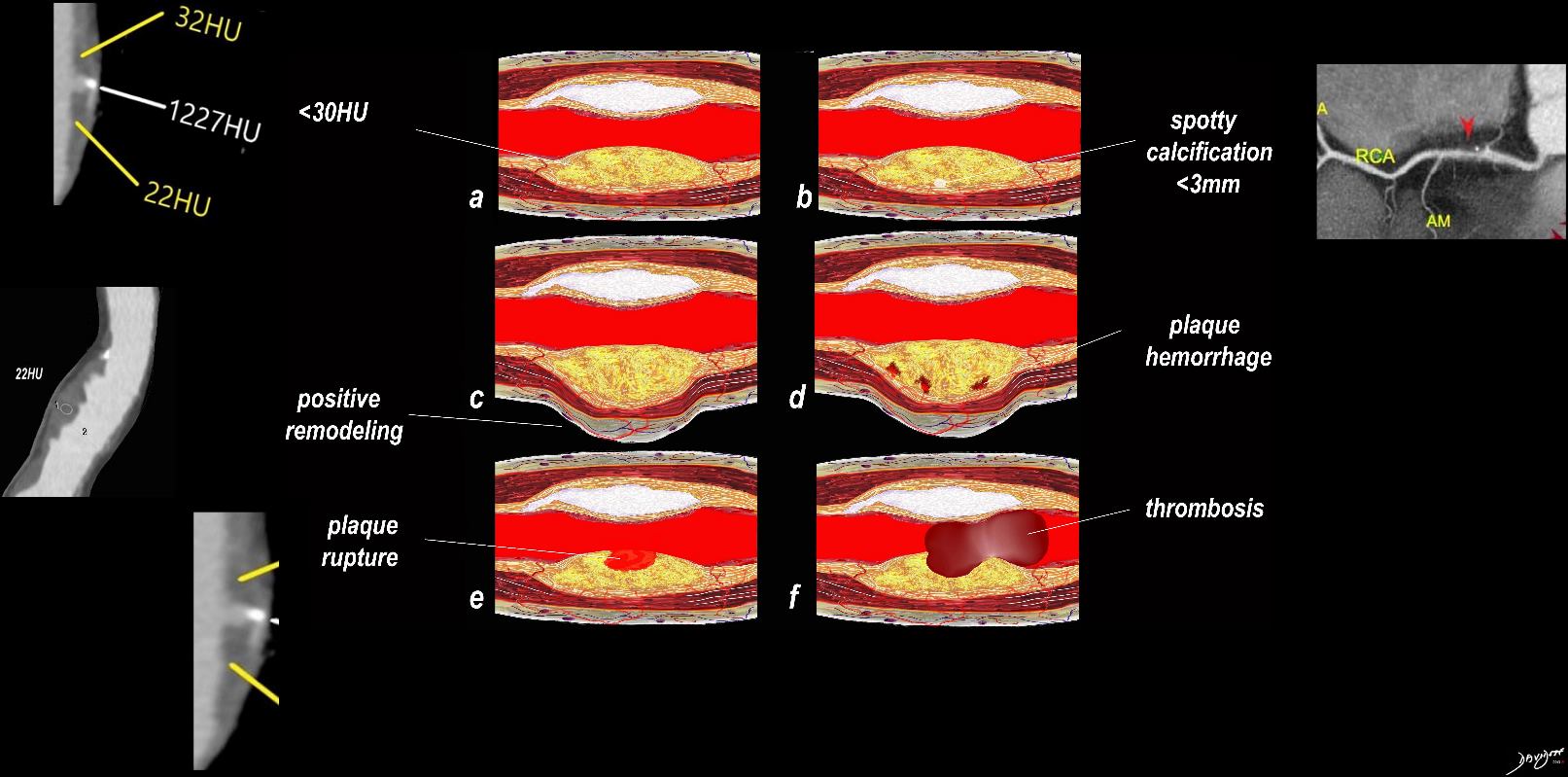
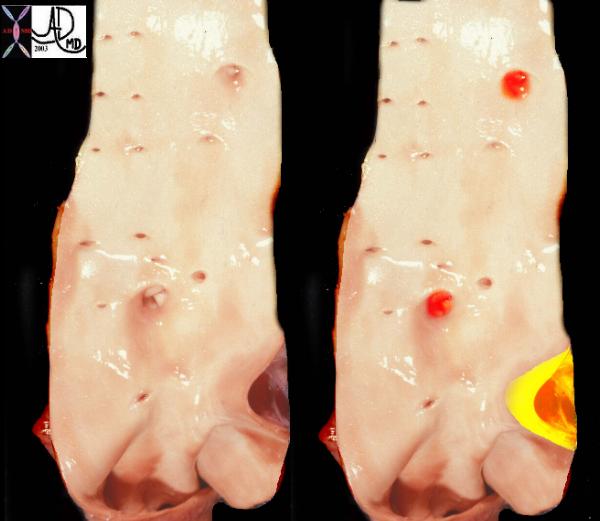
This image consists of (a) a longitudinal section through the coronary artery showing calcified plaque (white) and a fibrofatty plaque (yellow) with about a 50% stenosis. Vulnerability is considered with features of a thin fibrous cap, and a density of less than 30HU. The associated CT shows a low density plaque measuring between 22 and 32HU. Image b shows a focal spotty calcification within the fibrofatty plaque and an associated CT confirm a punctate calcification within the plaque which is another sign of the vulnerable plaque. Image c shows positive remodeling of the wall defines as an outer vessel diameter that is 10% larger than the diameter of the vessel just proximal and distal to the disease. Image d shows intraplaque hemorrhage due to the neovascularity of the vasa vasorum, image e shows plaque ulceration and image e shows thrombosis.
Ashley Davidoff thecommonvein.net
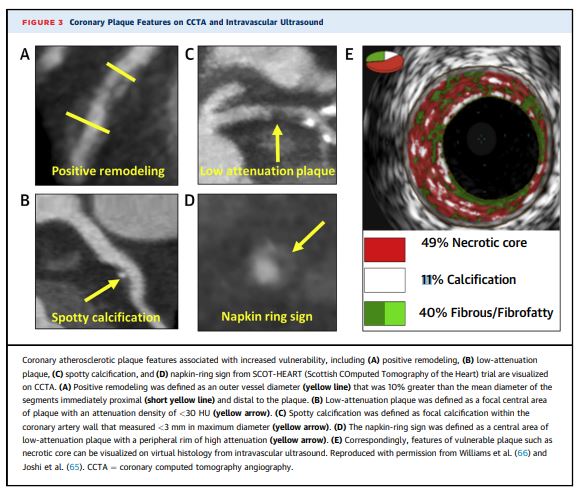
CT and Vulnerable Plaque – IVUS
Abdelrahman et JACC 2020
Patient with Psoriasis, Atherosclerotic Disease Before and After Biologic Therapy

Abdelrahman et JACC 2020
Conclusion and Summary
-
I saw it for myself in Washington DC
-
It is definitely on their minds
-
Saw the writing on the walls (floor) of the
-
National Airport
-
Between Concourse B and C
Digital Make Up of the Coronary Artery

Ashley Davidoff MD
thecommonvein.net
Mosaic on the floor of the Ronald Reagan National Airport in Washington
Concern for Lipid Infiltration into the Vessels
Concern for the Vulnerable
Focus to Treat and Help the Vulnerable Before it was too Late

Ashley Davidoff MD
thecommonvein.net
Mosaic on the floor of the Ronald Reagan National Airport in Washington
Advancing Computerised Evaluation of Flow Dynamics
Remembering the Role of Shear Stress

Ashley Davidoff MD
thecommonvein.net
Mosaic on the floor of the Ronald Reagan National Airport in Washington
Concern for Shortfalls of Energy Delivery
Attention to Myocardial Perfusion

Ashley Davidoff MD
thecommonvein.net
Mosaic on the floor of the Ronald Reagan National Airport in Washington
Approaching a Problem from Many Angles to get to the Truth

Looking at the Element in Hand from as MAny Angles in Order to Come to the Truth
Ashley Davidoff MD
thecommonvein.net
Mosaic on the floor of the Ronald Reagan National Airport in Washington
-
- Evaluation of stable chest pain often
- requires diagnostic testing with the
- goals of
- detecting coronary artery disease (CAD) and
- non obstructive
- obstructive
- assessing the risk of a
- future major adverse cardiovascular event (MACE),
- death,
- myocardial infarction, or
- unstable angina
- future major adverse cardiovascular event (MACE),
- detecting coronary artery disease (CAD) and
- Evaluation of stable chest pain often
-
Background and History
- Ravin
- My Teachers
- History of CT
- Coronary CTA – History
- Evaluation of Structure Why do we see things
- Contrast Resolution
- Spatial resolution
- Temporal Resolution
- History of CTA of the coronary arteries
- CT Anatomy
- Embryology
- History of Atherosclerosis
- Atherosclerosis
- Image Quality
- What is easy for us
- What is hard for us
- Blooming Artifact
- Penetrating Heavy Calcium
- Wall Characterization
- Artifacts
- Partial Volume Artifact
- Beam Hardening
- What is new?
- What is hard for us
- see web image 258 Anatomic imaging is very sensitive as to who may have a CV event down the line Functional image not so much or who may nothave an event
-
Indications
-
First Line Study (Narula J, et al 2021 Expert Consensus Document)
- Chest pain no known CAD presenting with
- Stable Typical Pain
- Atypical Chest Pain
- thought to represent a possible anginal equivalent
- Chest Pain with known CAD presenting with
- Stable Typical Pain
- Atypical Chest Pain
- thought to represent a possible anginal equivalent
- Unclear or inconclusive stress test results.
- When considering evaluation for revascularization strategies
-
- ISCHEMIA Trial
-
- Selected asymptomatic high risk individuals
- Rarely appropriate
- very low risk symptomatic patients, e.g., <40 years of age with non-cardiac symptoms (chest wall pain, pleuritic chest
pain) - low- and intermediate risk asymptomatic patients
- very low risk symptomatic patients, e.g., <40 years of age with non-cardiac symptoms (chest wall pain, pleuritic chest
-
- Risk Stratification
- A strong family history of early heart disease.
- Multiple other risk factors for coronary artery disease (hypertension, diabetes, cholesterol abnormality, smoking)
- Ruling out significant luminal stenoses in stable patients with suspected coronary stenoses, but intermediate pretest likelihood of disease
- most useful in patients with a low-to-intermediate likelihood of CAD
- patients with left bundle branch block of unknown etiology
- patients with new onset heart failure
- Confounding Cath
- Interesting and important associations in syndromes
- polyarteritis (89H)
- congenital coronary artery disease
- congenital heart disease
- Anomalous coronary origins
- aneurysms
- Plaque characterisation
-
Contraindications
- Renal
- Excessive Coronary Calcification
- Relative
- patient’s heart rate,
- body weight, or
- ability to perform a breath-hold,
- contrast or problems with
- vascular access (which may make invasive angiography more prone to complication)–
-
Advantages
- high negative predictive value
- Provides high-definition 3-D images of the arteries feeding the heart and blockages at the earliest stages when they can be treated most effectively
- Most accurate noninvasive diagnostic test for coronary artery disease
- Measures both calcified and noncalcified plaques. Noncalcified plaques are more prone to rupture and cause heart attacks than calcified plaques. By assessing both types of plaque, coronary CTA analyzes your risk for a heart attack.
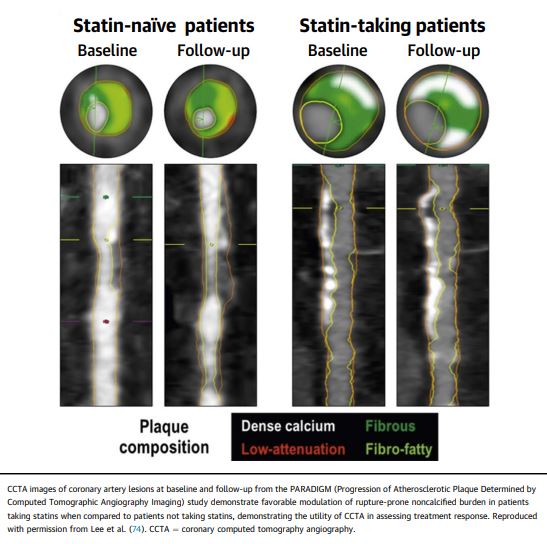
- Monitor the effectiveness of therapy since noncalcified plaques may shrink with effective treatment
- cross-sectional nature permits visualization not only of the contrast-enhanced coronary artery lumen, but also of the vessel wall (if image quality is adequate). In this way, atherosclerotic plaque can become visible, which is undetectable in the invasive coronary angiogram
-
Disadvantages
- lacking in
- specificity ie lot of false positives
- positive predictive accuracy, ie lot of false positives
- which has led to the development of value added CTA strategies like fractional flow reserve derived from CT and CT perfusion.
- Radiation
- Goal median <5milliSieverts (15 5-10 years ago)
- NM 10-15 milliSieverst
- Limited temporal resolution can reduce image quality, especially if heart rates are above 60 beats per minute (bpm)
- Since data acquired over several heartbeats are necessary to acquire a complete data set, coronary CTA is not reliably possible in patients with arrhythmias (scanner design concepts with ≥256 slices may help overcome this limitation).
- analysis was limited to segments of ≥1.5 mm in diameter.
- Also, there is a tendency to overestimate the degree of stenosis in CT as compared with the invasive angiogram,
- extensive calcifications can render image interpretation impossible.
- In patients with a very low pretest likelihood, the false-positive rate may be too high,
- patients with a very high pretest likelihood, sensitivity may not be sufficiently high.
- patients with a high pretest likelihood of disease, performing an invasive, catheter-based coronary angiogram will often be much more appropriate because it offers the option of immediate treatment.
- lacking in
-
Aim
-
Method
- Patient Preparation and Patient Factors
- Equipment
- Contrast
- Technique
- Gating
- Calcium Score
- When is it too high
- Coronary Evaluation
- Axial
- MPR
- 3D
- Ventricular Evaluation
- LV
- EF
- mass
- LV
- Myocardial Perfusion
- FFR
-
Results
- Evolving technology
- Fractional flow reserve derived from CT
- Lesion specific stenosis
- Calcific plaque limits
- CT perfusion.
- Global
- Tissue Characterization
- Fractional flow reserve derived from CT
- CAD RADS
- Linking reporting to Management Situations
- 1-5
- 2 Atheroscleosis
-
Conclusion
-
Summary
-
Links and References
- TCV
- TCV
- CTA of the Coronary Arteries
- Cases
- 023H Takotsubo Sarcoidosis and a Police Visit
- 028h 83fF Post MI Post Cath LV Contrast
- 047H Acute MI Left Main Occlusion Batwing CXR
- 067H Calcium score >2000
- 068H LV infero-basal aneurysm
- 072H 49M CAD CHF ground glass01 CONFIRM j.jacc.2011.02.074
- 074H 55F-AVM LAD incidental-finding
- 079H Left Main Calcification CTA Negative Angio
- 080H CTA LAD Disease CAth Negative
- 081H CT Heavy Calcification Lung Cancer Screening Discrepant Cath
- 084H coronary artery LAD and Cx separate origins
- 085H Conal artery to PA fistula (AVM)
- 086H Left Main High Grade Stenosis
- 087H RCA aneurysm in young female
- 088H Septic Shock Perforated Ulcer
- 089H Polyarteritis Nodosa and Coronary Artery Aneurysms
- 090H HOCM and Anomalous Origin of RCA from LCA Sinus
- Literature
- Need to review
- patient Stable CAD PAin in out
- CTA
- patient Stable CAD PAin in out
- Videos
- Gary Huang Cardiology University of Washington Has All the Trials Excellent
- Todd Vilines U of Virginia
- Chest Pain Guidelines has 2 videos
- Abdelrahman KM eta al State of the Art Review of CTA ACC
- Collet et al Implementing Coronary CTA in the Cath Lab
- Bhatt et al The Emerging Role of CTA in Stable Angina With ISCHEMIA
- Ahmadi A,Narula J Assessment of Coronary Disease Independent of Symptoms JACC
- Need to review
- Min, J et al A New Decade of Old Questions Steps Toward Demonstrating Efficacy of Physiologic CAD Evaluation by CT JACC
- Stone K.E. History of Coronary CTA
- Narula J, et al2021 Expert Consensus Document on Coronary CTA Society of Cardiovascular CT
- Kennedy JW. Complications associated with cardiac catheterization and angiography. Cath Cardiovasc Diagn. 1982;8:5-11.
- Vanhoenacker PK, Heijenbrok-Kal MH, Van Heste R, et al. Diagnostic performance of multidetector CT angiography for assessment of coronary artery disease: Meta-analysis. Radiology. 2007;44:419-428.
- Leschka S, Wildermuth S, Boehm T, et al. Noninvasive coronary angiography with 64-section CT: Effect of average heart rate and heart rate variability on image quality. Radiology. 2006;241:378-385.
- Hoffmann MH, Shi H, Manzke R, et al. Noninvasive coronary angiography with 16-detector row CT: Effect of heart rate. Radiology. 2005;234:86-97.
- Herzog C, Arning-Erb M, Zangos S, et al. Multi-detector row CT coronary angiography: Influence of reconstruction technique and heart rate on image quality. Radiology. 2006;238:75-86
- Ghostine S, Caussin C, Daoud B, et al. Non-invasive detection of coronary artery disease in patients with left bundle branch block using 64-slice computed tomography. J Am Coll Cardiol. 2006;48:1929-1934.
- Leber AW, Johnson T, Becker A, et al. Diagnostic accuracy of dual-source multi-slice CT-coronary angiography in patients with an intermediate pretest likelihood for coronary artery disease. Eur Heart J. 2007;28:2354-2360.
- Scheffel H, Alkadhi H, Plass A, et al. Accuracy of dual-source CT coronary angiography: First experience in a high pre-test probability population without heart rate control. Eur Radiol. 2006;16:2739-2747.
- Ropers U, Ropers D, Pflederer T, et al. Influence of heart rate on the diagnostic accuracy of dual-source computed tomography coronary angiography. J Am Coll Cardiol. 2007;50:2393-2398.
- Hendel RC, Patel MR, Kramer CM, et al. ACCF/ ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging. J Am Coll Cardiol. 2006;48:1475-1497.
- Hamon M, Biondi-Zoccai GG, Malagutti P, et al. Diagnostic performance of multislice spiral computed tomography of coronary arteries as compared with conventional invasive coronary angiography: A meta-analysis. J Am Coll Cardiol. 2006;48:1896-1910.
- Shroeder S, Achenbach S, Bengel F, et al. Cardiac computed tomography: Indications, applications, limitations, and training requirements: Report of a Writing Group deployed by the Working Group Nuclear Cardiology and Cardiac CT of the European Society of Cardiology and the European Council of Nuclear Cardiology. Eur Heart J. 2008;In press.
- Meijboom WB, van Mieghem CA, Mollet NR, et al. 64-slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol. 2007;50:1469-1475.
- Andreini D, Pontone G, Pepi M, et al. Diagnostic accuracy of multidetector computed coronary tomography angiography in patients with dilated cardiomyopathy. J Am Coll Cardiol. 2007;49:2044-2050.
- Hoffmann U, Nagurney JT, Moselewski F, et al. Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation. 2006;114:2251-2260. Erratum in: Circulation. 2006;114:e651.
- Meijboom WB, Mollet NR, Van Mieghem CA, et al. 64-slice computed tomography coronary angiography in patients with non-ST elevation acute coronary syndrome. Heart. 2007;93:1386-1392.
- Goldstein JA, Gallagher MJ, O’Neill WW, et al. A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol. 2007;49:863-871.
- Rubinshtein R, Halon DA, Gaspar T, et al. Usefulness of 64-slice cardiac computed tomographic angiography for diagnosing acute coronary syndromes and predicting clinical outcome in emergency department patients with chest pain of uncertain origin. Circulation. 2007;115:1762-1768.
- Hollander JE, Litt HI, Chase M, et al. Computed tomography coronary angiography for rapid disposition of low-risk emergency department patients with chest pain syndromes. Acad Emerg Med. 2007;14:112-116.
- Deibler AR, Kuzo RS, Vöhringer M. Imaging of congenital coronary anomalies with multislice computed tomography. Mayo Clin Proc. 2004;79: 1017-1023.
- Datta J, White CS, Gilkeson RC, et al. Anomalous coronary arteries in adults: Depiction at multi-detector row CT angiography. Radiology. 2005;235:812-818.
- Dodd JD, Ferencik M, Liberthson RR, et al. Congenital anomalies of coronary artery origin in adults: 64-MDCT appearance. AJR Am J Roentgenol. 2007; 188:W138-W146.
- Meijboom WB, Mollet NR, Van Mieghem CA, et al. Pre-operative computed tomography coronary angiography to detect significant coronary artery disease in patients referred for cardiac valve surgery. J Am Coll Cardiol. 2006;48:1658-1665.
- Nieman K, Pattynama PM, Rensing BJ, et al. Evaluation of patients after coronary artery bypass surgery: CT angiographic assessment of grafts and coronary arteries. Radiology. 2003;229:749-756.
- Martuscelli E, Romagnoli A, D’Eliseo A, et al. Evaluation of venous and arterial conduit patency by 16-slice spiral computed tomography. Circulation. 2004;110: 3234-3238.
- Schlosser T, Konorza T, Hunold P, et al. Noninvasive visualization of coronary artery bypass grafts using 16-detector row computed tomography. J Am Coll Cardiol. 2004;44:1224-1229.
- Chiurlia E, Menozzi M, Ratti C, et al. Follow-up of coronary artery bypass graft patency by multislice computed tomography. Am J Cardiol. 2005;95:1094-1097.
- Feuchtner GM, Schachner T, Bonatti J, et al. Diagnostic performance of 64-slice computed tomography in evaluation of coronary artery bypass grafts. AJR Am J Roentgenol. 2007;189:574-580.
- Salm LP, Bax JJ, Jukema JW, et al. Comprehensive assessment of patients after coronary artery bypass grafting by 16-detector-row computed tomography. Am Heart J. 2005;150:775-781.
- Ropers D, Pohle FK, Kuettner A, et al. Diagnostic accuracy of noninvasive coronary angiography in patients after bypass surgery using 64-slice spiral computed tomography with 330-ms gantry rotation. Circulation. 2006;114:2334-2341.
- Meyer TS, Martinoff S, Hadamitzky M, et al. Improved noninvasive assessment of coronary artery bypass grafts with 64-slice computed tomographic angiography in an unselected patient population. J Am Coll Cardiol. 2007;49:946-950.
- Mollet NR, Hoye A, Lemos PA, et al. Value of preprocedure multislice computed tomographic coronary angiography to predict the outcome of percutaneous recanalization of chronic total occlusions. Am J Cardiol. 2005;95:240-243.
- Pflederer T, Ludwig J, Ropers D, et al. Measurement of coronary artery bifurcation angles by multidetector computed tomography. Invest Radiol. 2006;41:793-798.
- Maintz D, Seifarth H, Raupach R, et al. 64-slice multidetector coronary CT angiography: In vitro evaluation of 68 different stents. Eur Radiol. 2006;16:818-826.
- Gilard M, Cornily JC, Pennec PY, et al. Assessment of coronary artery stents by 16 slice computed tomography. Heart. 2006;92:58-61.
- Schuijf JD, Bax JJ, Jukema JW, et al. Feasibility of assessment of coronary stent patency using 16-slice computed tomography. Am J Cardiol. 2004;94:427-430.
- Gaspar T, Halon DA, Lewis BS, et al. Diagnosis of coronary in-stent restenosis with multidetector row spiral computed tomography. J Am Coll Cardiol. 2005;46:1573-1579.
- Gilard M, Cornily JC, Rioufol G, et al. Noninvasive assessment of left main coronary stent patency with 16-slice computed tomography. Am J Cardiol. 2005;95:110-112.
- Van Mieghem CA, Cademartiri F, Mollet NR, et al. Multislice spiral computed tomography for the evaluation of stent patency after left main coronary artery stenting: A comparison with conventional coronary angiography and intravascular ultrasound. Circulation. 2006;114:645-653.
- Rixe J, Achenbach S, Ropers D, et al. Assessment of coronary artery stent restenosis by 64-slice multi-detector computed tomography. Eur Heart J. 2006; 27:2567-2572.
- Oncel D, Oncel G, Karaca M. Coronary stent patency and in-stent restenosis: Determination with 64-section multidetector CT coronary angiography- initial experience. Radiology. 2007; 242:403-409.
- Ehara M, Kawai M, Surmely JF, et al. Diagnostic accuracy of coronary in-stent restsnosis using 64-slice computed tomography.J Am Coll Cardiol.2007; 49:951-959.
- Rist C, von Ziegler F, Nikolaou K, et al. Assessment of coronary artery stent patency and restenosis using 64-slice computed tomography. Acad Radiol.2006;13:1465-1473.
- Cademartiri F, Schuijf JD, Pugliese F, et al. Usefulness of 64-slice multislice computed tomography coronary angiography to assess in-stent restenosis. J Am Coll Cardiol. 2007;49:2204-2210.
- Becker CR, Knez A, Ohnesorge B, et al. Imaging of noncalcified coronary plaques using helical CT with retrospective ECG gating. AJR Am J Roentgenol. 2000;175:423-424.
- Achenbach S, Moselewski F, Ropers D, et al. Detection of calcified and noncalcified coronary atherosclerotic plaque by contrast-enhanced, submillimeter multidetector spiral computed tomography: A segment-based comparison with intravascular ultrasound. Circulation. 2004;109:14-17.
- Leber AW, Knez A, Becker A, et al. Accuracy of multidetector spiral computed tomography in identifying and differentiating the composition of coronary atherosclerotic plaques: A comparative study with intracoronary ultrasound. J Am Coll Cardiol. 2004;43:1241-1247.
- Leber AW, Becker A, Knez A, et al. Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: A comparative study using intravascular ultrasound. J Am Coll Cardiol. 2006;47:672-627.
- Schroeder S, Kopp AF, Baumbach A, et al. Noninvasive detection and evaluation of atherosclerotic coronary plaques with multislice computed tomography. J Am Coll Cardiol. 2001;37:1430-1435.
- Achenbach S, Ropers D, Hoffmann U, et al. Assessment of coronary remodeling in stenotic and nonstenotic coronary atherosclerotic lesions by multidetector spiral computed tomography. J Am Coll Cardiol. 2004;43:842-847.
- Caussin C, Ohanessian A, Ghostine S, et al. Characterization of vulnerable nonstenotic plaque with 16-slice computed tomography compared with intravascular ultrasound. Am J Cardiol. 2004;94:99-100.
- Carrascosa PM, Capuñay CM, Garcia-Merletti P, et al. Characterization of coronary atherosclerotic plaques by multidetector computed tomography. Am J Cardiol. 2006;97:598-602.
- Pohle K, Achenbach S, Macneill B, et al. Characterization of non-calcified coronary atherosclerotic plaque by multi-detector row CT: Comparison to IVUS. Atherosclerosis. 2007;190:174-180.
- Moselewski F, Ropers D, Pohle K, et al. Comparison of measurement of cross-sectional coronary atherosclerotic plaque and vessel areas by 16-slice multi-detector computed tomography versus intra-vascular ultrasound. Am J Cardiol. 2004;94: 1294-1297.
- Hoffmann U, Moselewski F, Nieman K, et al. Noninvasive assessment of plaque morphology and composition in culprit and stable lesions in acute coronary syndrome and stable lesions in stable angina by multidetector computed tomography. J Am Coll Cardiol. 2006;47:1655-1662.
- Motoyama S, Kondo T, Sarai M, et al. Multislice computed tomographic characteristics of coronary lesions in acute coronary syndromes. J Am Coll Cardiol. 2007;50:319-326.
- Schuijf JD, Beck T, Burgstahler C, et al. Differences in plaque composition and distribution in stable coronary artery disease versus acute coronary syndromes; non-invasive evaluation with multi-slice computed tomography. Acute Card Care. 2007;9: 48-53.
- Pundziute G, Schuijf JD, Jukema JW, et al. Prognostic value of multislice computed tomography coronary angiography in patients with known or suspected coronary artery disease. J Am Coll Cardiol. 2007; 49:62-70.
-
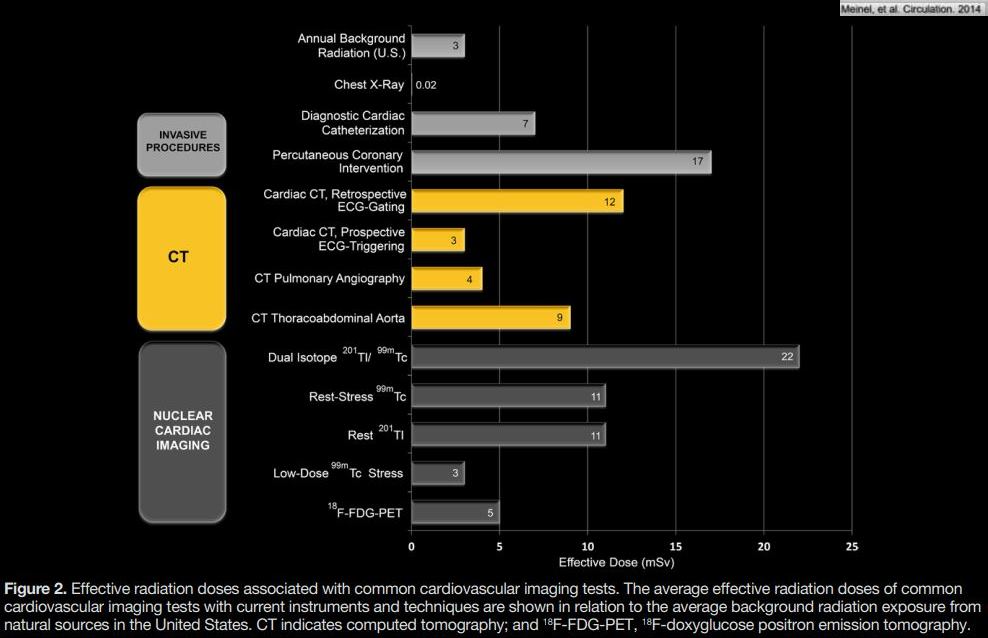
Meinel, F et al Radiation Risks From Cardiovascular Imaging Tests Circulation. 2014;130:442-445 PDF file