
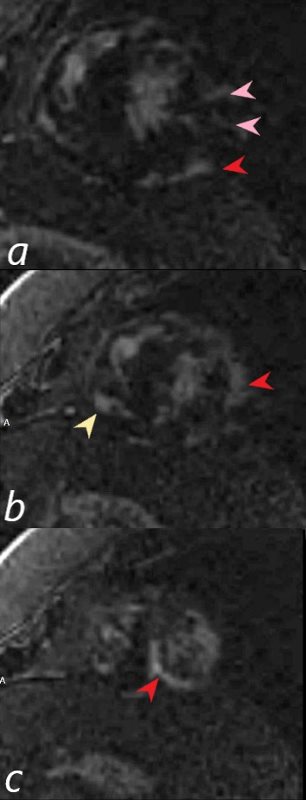
69-year-old male presented with history of cardiomyopathy and atrial fibrillation
There are multicentric foci of LGE in this short axis view taken closer to the apex with linear form in the mid myocardial region (pink arrowheads) and linear and nodular changes of LGE in the subepicardial layers (red arrowheads, a,b,c) Subepicardial changes are also notes in the RV in a (not marked)
The findings on MRI are highly suggestive of sarcoidosis.
There was associated global hypokinesis of the LV with an EF of 40%, and increase in the LV mass of 120gms/ sq m
Ashley Davidoff MD
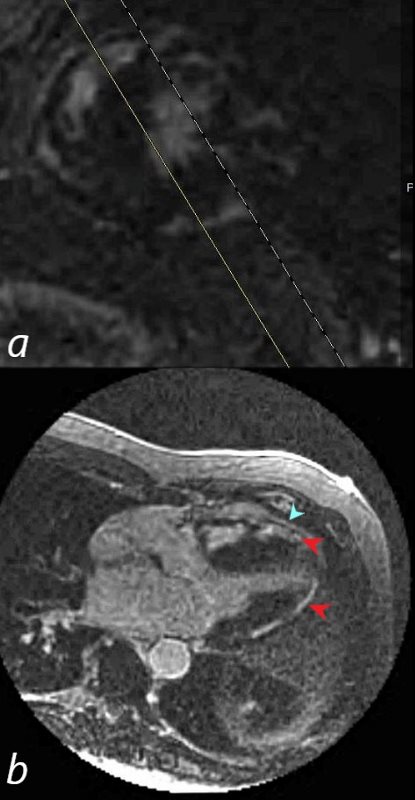
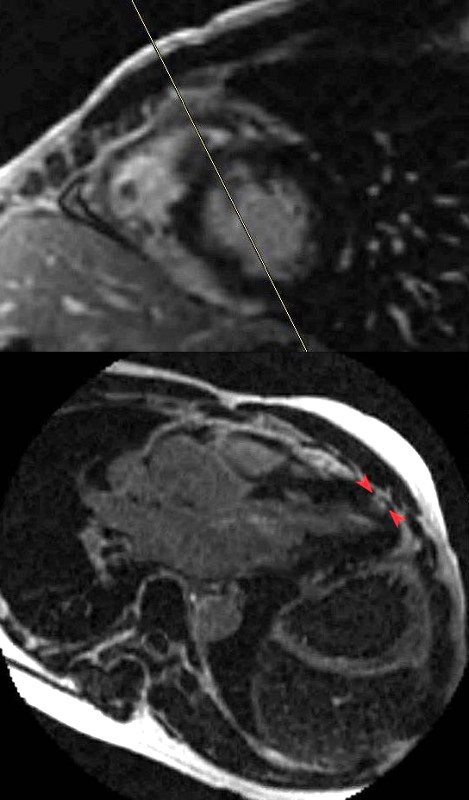
69-year-old male presented with history of cardiomyopathy and atrial fibrillation
In this series the long axis 3 chambered view reveals intense continuous sub epicardial disease (red arrowheads) and pericardial LE (teal blue arrowhead)
Ashley Davidoff MD
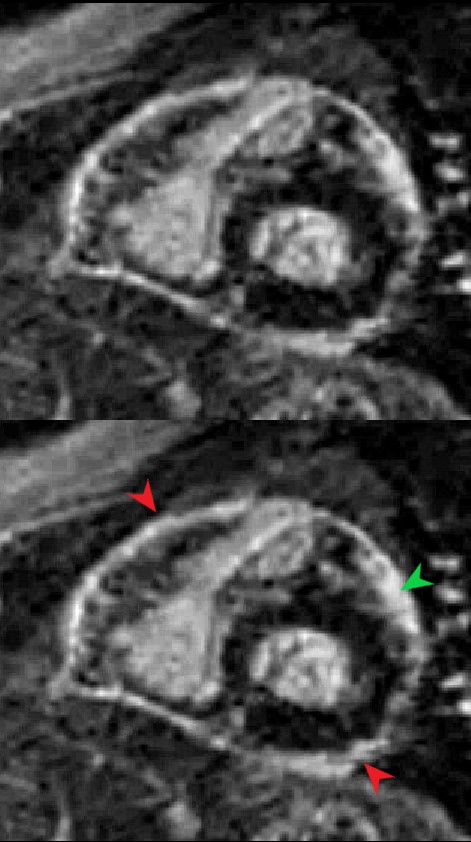
The short axis LGE sequence shows focal diffuse subepicardial LGE (green arrowhead) Extensive pericardial enhancement is also noted (red arrowheads)
Ashley Davidoff MD
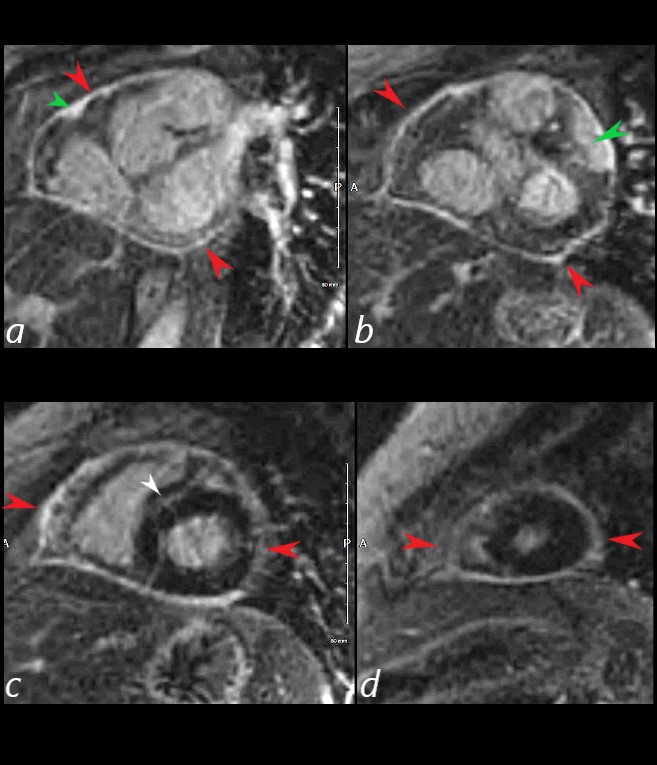
The short axis LGE sequence starting at the base of the heart (a, b) progressing through the body c and apex (d) shows focal LGE in the RVOT(a, green arrowhead) and in the LV (b green arrowhead) extensive pericardial enhancement (a,b,c,d – red arrowheads, and in the septum (white arrowhead c).
Ashley Davidoff MD
57-year-old male with pathology findings consistent with granulomatous hepatitis and non-necrotizing granulomas in inguinal lymph nodes both consistent with sarcoidosis but without pulmonary findings. Lymphadenopathy is also present in the axillae and groins without involvement of the mediastinum
• Associated cardiovascular findings include findings consistent with hypertrophic cardiomyopathy with:
o Diabetes and Hypertension
o CXR showing LVE
o Abnormal stress test with concerning regions in RCA territory inferiorly
o Moderate LVH on echo with normal EF (68%) normal LA, RA PAP and RV function. LV mass was 127g/sq. m
o Focal nodular LGE in the anterior apical region in mid myocardial/subendocardial region and in the inferior mid myocardial wall medially
o Subsequently developed episodes of paroxysmal ventricular tachycardia with EP ablation and placement of a defibrillator (ICD)
o LH and RH catheterization performed 6 years after initial studies showed elevation of PC WP of 25 mmHg, mean RA pressure of 16 mmHg, mean PAP of 34 mmHg no CAD
o Subsequent CT showed mildly enlarged LA and RA with mild TR
o 6 years after initial presentation he had symptoms of biventricular failure with increasing dyspnea and pedal edema culminating in an acute episode of monomorphic VT episode, ectopic atrial flutter/fibrillation, and left bundle branch aberrancy requiring amiodarone and cardioversion. Underwent upgrade to biventricular upgrade to his ICD
Ashley Davidoff MD

34-year-old male who was diagnosed with pulmonary sarcoidosis 1 year before, presents with progressive dyspnea over 6 months, previously able to run 5 miles per day and currently limited to walking short distances. Clinical evaluation revealed that he was in complete heart block with a heart rate of 35 /min. EKG showed a rate of 40 with AV dissociation with alternating junctional and ventricular escape rhythms.
CXR showed upper lobe predominance interstitial changes, slightly more prominent on the right side. There was evidence of CHF with enlargement of the LA (widening of the carinal angle) and cephalization of the vessels
An echocardiogram was normal with normal ejection fraction.
MRI revealed normal cardiac function, mild left atrial enlargement, and diffuse almost circumferential subendocardial enhancement of the LV,(red arrowheads) most prominent in the lateral wall. There was also a linear focus in the mid myocardium in the anterior region medially near the septum (green arrowheads)
A dual lead pacemaker was placed and follow up CXR showed improved CHF an persistent interstitial findings dominant in the upper lobes consistent with sarcoidosis.
Follow up CXR 7 years later showed a normal CXR. The pacemaker had been removed and the interstitial process had resolved
Ashley Davidoff MD