
Ganesh Athappan MD Ashley Davidoff MD

The right atrium forms the right border of the heart as it lies in the chest with the IVC (Inferior Vena Cava) and the SVC (Superior Vena Cava) entering near its most lateral border. Davidoff MD 06644 06.8s
The right atrium, one of the two upper chambers of the heart, receives deoxygenated blood from the superior and inferior vena cavae and the coronary sinus, and pumps it into the right ventricle through the tricuspid valve.
The infrastructure of the heart is a cross resulting conceptually in a box with four chambers. The upper chambers are the receiving chambers and the lower chambers are the pumping chambers. Between the two atria is the interatrial septum, and between the two ventricles is the interventricular septum.
This diagram shows perfect symmetry. The heart although having the same infrastructure has a beautiful asymmetric symmetry, similar to the painting of a Girl Before the Mirror by Picasso.
Ashley Davidoff MD
Structurally it is thin walled muscular sac separated from the RV by the tricuspid valve.
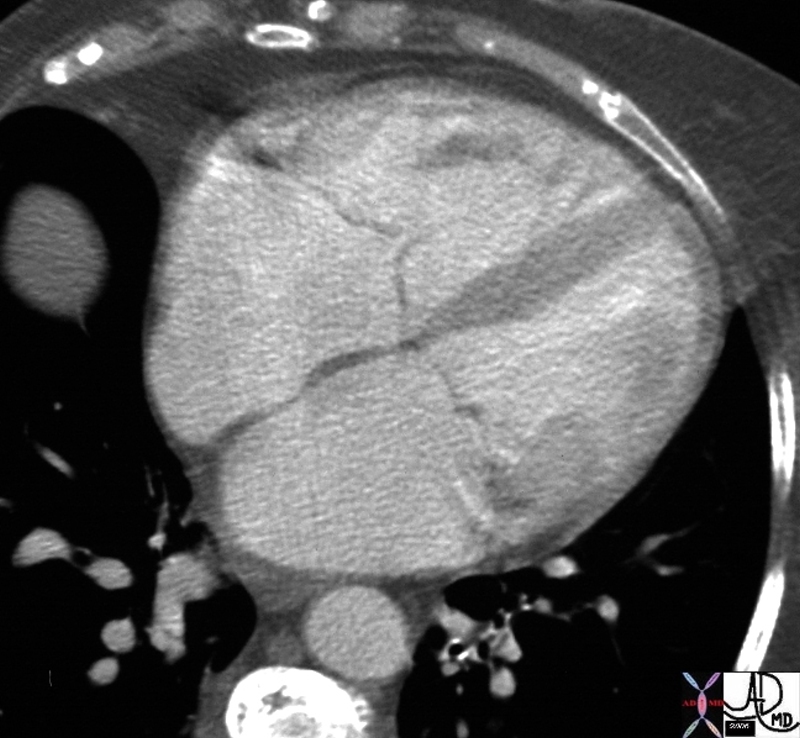
This axial image of the heart is through the mitral (right ) and tricuspid valve (left) right atrium and left atrium (right) which are normal and about the same size. The left ventricle with the papillary muscles and the right ventricle with its papillary muscle are well seen. Note the right sided structures tend to be anterior and left sided structures tend to be posterior. Note also that the right atrium and the left atrium are about the same size and shape in this view with flat walls.
Ashley Davidoff MD 27531d01.8s
TheCommonVein.net
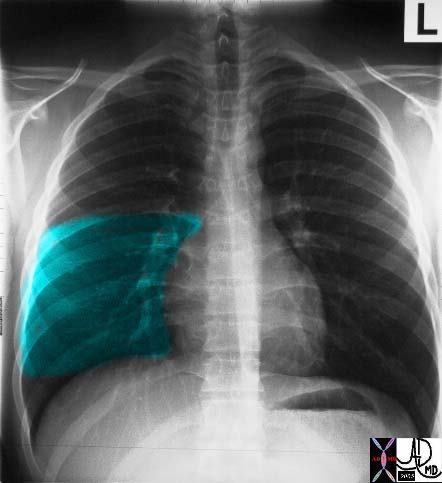
This P-A view of the chest reveals the position of the normal right middle lobe. Note how much smaller the right middle lobe is compared to the RLL. In this view it is roughly rectangular in shape. code chest code lungs code heart fx normal imaging radiology CXR plain film medical students chest RML
Courtesy Ashley Davidoff MD. 30397b03
Functionally it acts as a conduit for blood from the systemic venous circulation and directing it to the RV. It receives venous blood from the SVC and IVC and early in the cycle the blood is transferred passively and later in the cycle there is active contraction that enables the topping up of the right ventricle via the tricuspid valve into the RV.
Structural considerations
The right atrium has three basic parts: the appendage, the vestibule, and the venous component.
Viewed from outside the dominant portion is the anterolaterally located triangular appendage 2, which unlike that of the left is large and enjoys a wide junction with the venous component. This junction is marked by a fat filled groove externally termed the terminal groove or sulcus terminalis which internally corresponds to the terminal crest or crista terminalis 2.
With a black triangle for a nose and a white spot for the eye, Snoopy’s face becomes real – you almost want to pet the beagle like face.
Ashley Davidoff MD 32084

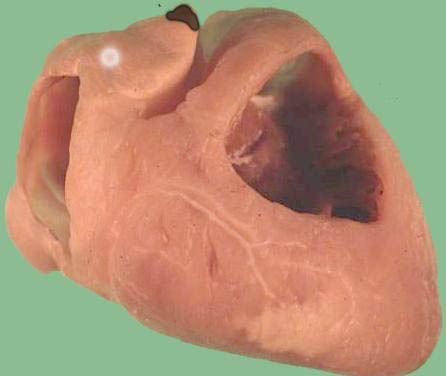
The atrial appendages wrap around the great vessels. The right atrial appendage has a triangular configuration and the left atrial appendage is thinner and has got finger like projections on its inferior surface
key words
heart cardiac RA RAA right atrium right atrial appendage LA LAA left atrium left atrial appendage shape anatomy normal gross anatomy post mortem specimen
Courtesy Ashley Davidoff copyright 2019 06411.8

Ct scan through the heart at the level of the left atrium shows a normal broad right atrial appendage cupping, or enfolding the great vessels and positioned at right angles to the left atrium.
Courtesy Ashley Davidoff MD 2019
33750.6.

CT scan through the heart at the level of the left atrium shows a normal narrow atrial appendage, with an irregular shaped border, cupping, or enfolding the great vessels and positioned, slightly posterior to the right atrial appendage.
Courtesy Ashley Davidoff MD 2019
34772.6
The sinus node lies in this groove close to the superior cavoatrial junction 2.
The vestibule is represented by a smooth muscular rim surrounding the tricuspid orifice.
The venous component as the name implies receives the caval veins and coronary sinuses. It is also smooth.
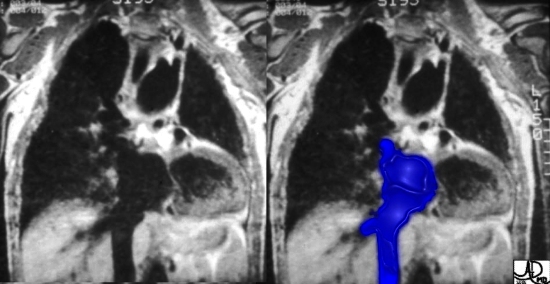
The right atrium can be best defined from a structural point of view as that chamber that receives the IVC. In this case of tricuspid atresia, the enlarged IVC empties into the enlarged right atrium, which has no egress into the right atrium because the tricuspid valve has not formed. Instead the blood goes via an atrial septal defect into the left atrium, and then into the left ventricle.
Courtesy Davidoff MD
32086

In this anatomic specimen the SVC and IVC are well seen and their lateral relationship to the right atrium is appreciated. They are embryological remnants of the sinus venosus and their similarity and conjoined structural origin and functionality can be well appreciated in this image. Davidoff MD
Key Words
heart cardiac RA right atrium thebesian valves coronary sinus Eustachian valve sulcus terminalis fossa ovalis foramen ovale septum secundum superior limbic band IVC inferior vena cava anatomy normal gross anatomy post mortem specimen
Courtesy Ashley Davidoff MD 2019 01707.6
Viewed from within one can see the following structures:
Eustachian valve 2 : Fibromuscular tissue that inserts medially into the sinus septum and serves to guard the entrance of the IVC. In some cases it may be large and pose an obstacle to catheter passed from the IVC. The free border of the Eustachian valve forms the tendon of Todaro, one of the borders of the triangle of Koch that contains the AV node2.
Triangle of Koch 2 is demarcated by the tendon of Todaro posteriorly, the tricuspid valve anteriorly, the coronary sinus inferiorly and the central fibrous body at the apex. The central fibrous body is the land mark for penetration of the bundle of His 2.
Thebesian Valve : A crescentic flap that guards the orifice of the coronary sinus.
Size of the Right Atrium
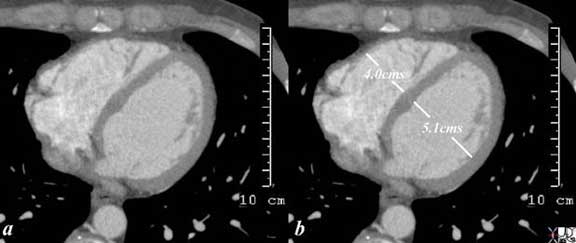
The linear measurements for the normal right atrium are a short axis of 3.5 cms and a long axis of 5.5cms. Since it has the same volume as the left atrium it should be about the same size but comparison is not that easy for a few reasons, including the different orientations of the chambers as well as the fact that they often lie in different planes making comparison at a single level difficult.. The long axis of the right atrium is mostly in an A-P direction,whereas the long axis of the left atrium is mostly in a transverse direction. They also lie only a slightly different axial plane so theat theright strium (like most right sided structures
Normally, right and left atria are the same size.

Normal Right Atrium and Left Atrium |
| This axial image of the heart is through the mitral (right ) and tricuspid valve (left) right atrium and left atrium (right) which are normal and about the same size. The left ventricle with the papillary muscles and the right ventricle with its papillary muscle are well seen. Note the right sided structures tend to be anterior and left sided structures tend to be posterior. Note also that the right atrium and the left atrium are about the same size and shape in this view with flat walls.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 27531d01.8s |
|
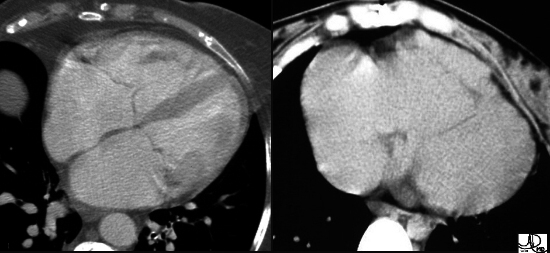
Right Atrium Normal and Enlarged |
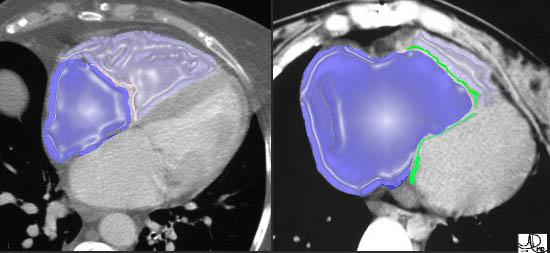
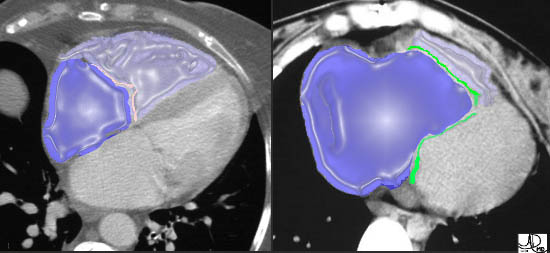
| These two images are enhanced CT images through the tricuspid valve. The first image is normal, while the second image demonstrates a TV that lies too far forward and low associated with a huge RA and a diminutive RV. This appearance is classical of a congenital condition called Ebstein’s anomaly. In this disease, the posterior leaflet is stuck down to the posterior wall of the RV and the anterior leaflet is larger than normal often giving a flapping sound to the listening ear. The anterior leaflet behaves like a flapping sail in the wind of the blood flow.
In the overlays, the RA is in royal blue and the RV is in light purple overlay. The normal TV in the first image is in pink while the malformed valve in the second image is in green. Note how large the RA is and how small the RV is in Ebstein’s anomaly. Courtesy of Ashley Davidoff M.D. 32102 32101 copyright 2009 |
Clinical Considerations :
The right atrium is the site for catheter ablation of right atrial arrhythmias, AVNRT, for guiding transseptal puncture, for coronary sinus cannulation, and for correct positioning of atrial pacing leads or atrial septal occluder devices. For the interventionist, it is the most commonly used cardiac chamber for entering the heart 3.
After the “dance of the scaffold”, we positioned it rightward and inferior to the LA – with the added piece that it forms a border with the middle lobe of the right lung. As mentioned before, the right and left atria are structurally different beasts – as we say – as different as “chalk and cheese”.
Pectinate muscles, tenia saginata, and limbic bands, all make the right atrium an extremely interesting chamber, as opposed to the more boring smooth walled left atrium. Even as you look on the outside, the atrial appendages are different. The right appendage is more triangular in shape – like Snoopy’s nose and the left appendage is shaped like a crooked index finger, or some say like the tip of the map of South America.
Diseases of the RA, in isolation are rare but usually manifest as RA dilation secondary to RV dysfunction, tricuspid incompetence, pulmonic stenosis, intracardiac shunts or congenital disorders like Ebstein’s anomaly.
Courtesy of: Ashley Davidoff, MD
aka 37758b01c01.8s
aka heart anatomy P 040
Courtesy of: Ashley Davidoff, M.D heart-anatomy-P-047

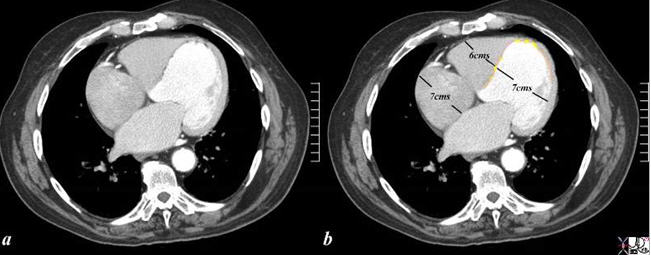
The axial CT scan through the right side of the heart shows an enlarged right atrium and right ventricle in this 88 year old patient with right heart failure with known tricuspid regurgitation The round capaciousness of both chambers provides the subjective impression of RAE and RVE.
key words
cardiac heart CVS RA large enlarged imaging radiology CTscan
Courtesy Ashley Davidoff MD 2019
70344a
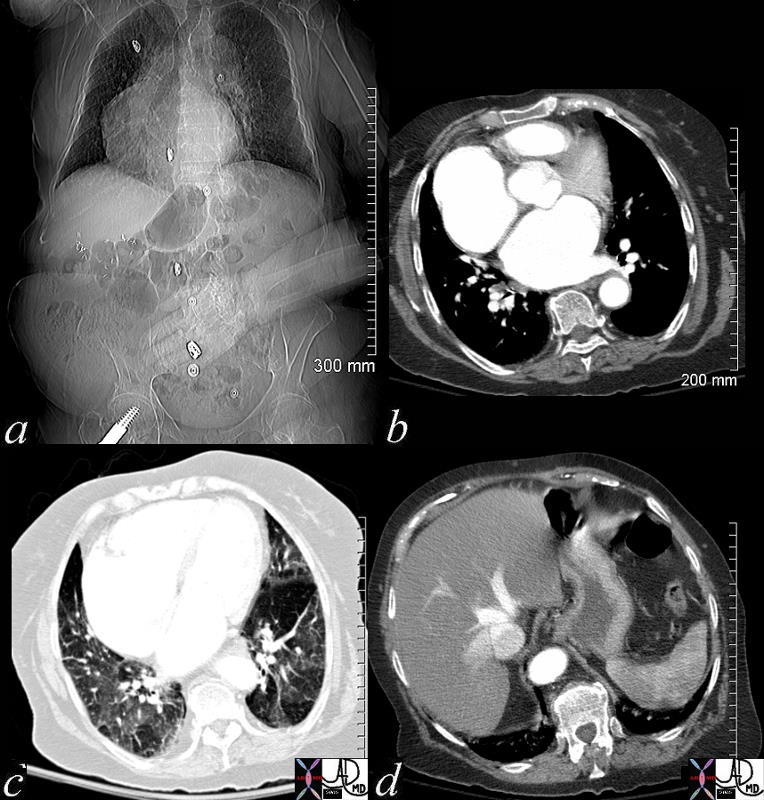
48098c02 heart cardiac right atrium RA left atrium LA fx enlarged fx dextrocardia lung ground glass changes mosaic perfusion Kerley B lines liver enlarged hepatic veins fx reflux into the hepatic veins dx tricuspid regurgitation tricuspid valve dx acquired dextrocardia congestive heart failure CHF CTscan scout Davidoff MD 48098c01 48098c02 48089b01
Diagnosis of RA disease is rarely suspected clinically but is an accompaniment of RV dysfunction which presents with signs of elevated jugular veins, hepatic congestion, hepatomegaly, ascites , bilateral pitting pedal edema. On examination a RV heave may be palpated in the left parasternal area. Chest radiography shows RV enlargement. EKG characteristics of RA enlargement are narrow P wave of increased amplitude (P pulmonale) on lead I1. Two dimensional echocardiography serves to accurately predict the size and function of the RA.
References
Google Books ( Last Accessed on 03-31-08)
Ho SY, Anderson RH and Quintana DS. Atrial structures and fibers: morphological basis of atrial conduction. Cardiovascular Research 54 (2002) 325 –336.
Duytschaever M, Ho SY, Devos D and Tavernier R. The left hand as a model for the right atrium: a simple teaching tool. Europace 2006 8(4):245-250.
Sachin et al Radiographics The Right Atrium: GAteway to the Heart