
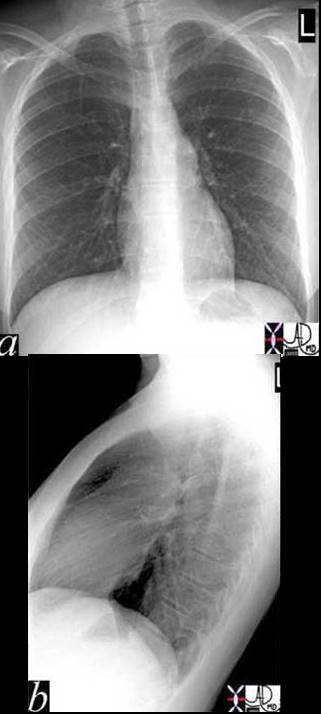
In the P-A projection the normal heart takes up about 30% of the diaphragmatic surface. Similarly in the lateral projection the heart takes up a third of the diaphragmatic surface. In addition the heart takes up the bottom 1/3 of the retrosternal air space.
Ashley Davidoff MD
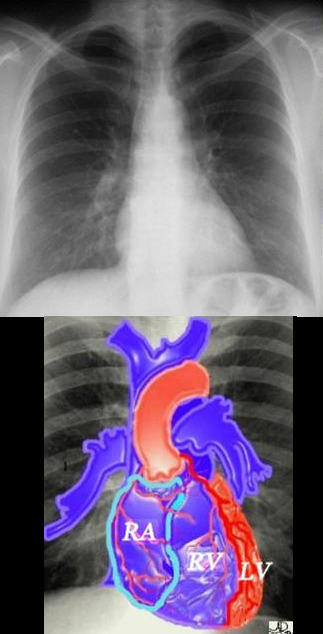
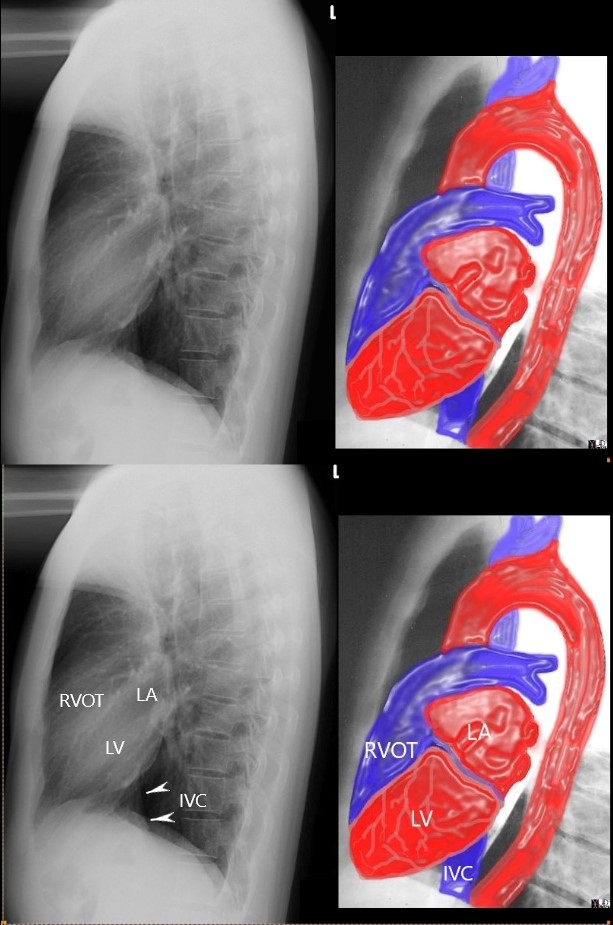
If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung. The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior view. It marks the position of the interventricular septum.
Ashley Davidoff MD
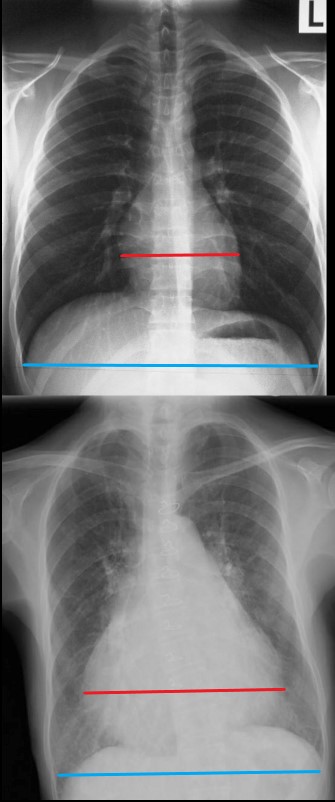
The maximum transverse length of the heart is expressed as a percentage of the maximum length of the internal diameter of the chest. When this ratio – the cardiothoracic ratio (c t r) is greater than 50% cardiomegaly is present. The top image is normal and the bottom reflects cardiomegaly
Ashley Davidoff MD
71 year old Asian female with rheumatic heart disease dominated by calcific mitral stenosis mild MR, moderate tricuspid regurgitation and secondary pulmonary hypertension.
Ashley Davidoff MD
Ashley Davidoff MD
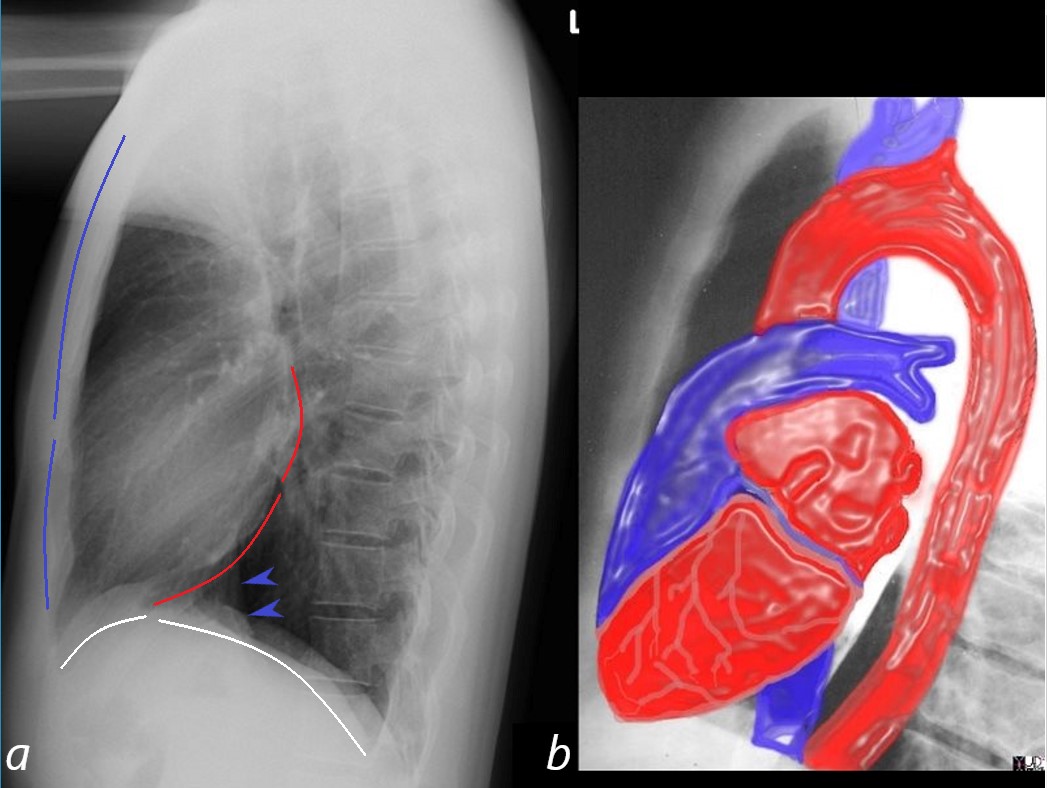
A normal lateral examination of the chest X-ray (CXR, a) shows the relative size and ratios of the anterior border of the heart in relation to the sternomanubrial junction (blue lines), the inferior border of the heart in relation to the diaphragm (white lines) and the posterior border of the heart (red lines)
The first rule of thirds states that the ratio or relative length of the anterior border of the heart is about 1/3 the length of the length from the inferior border of the heart to the sternomanubrial junction. In right ventricular enlargement the heart takes up more than a 1/3 and fills in the retrosternal space and this indicates right ventricular enlargement RVE).
The second rule of thirds states that the ratio or relative length of the inferior border of the heart is about 1/3 the length of the length from the posterior inferior border border of the heart to the insertion pint of the left hemidiaphragm posteriorly. When this ratio increases then there is left ventricular enlargement (LVE).
The third rule of thirds states that the ratio or relative length of the posterior border of the left atrium (LA) is about 1/3 of the length from the inferior border of the LA to the inferior border of the LV on the left hemidiaphragm. When this ratio increases then there is left ventricular enlargement (LVE).
A fourth rule (not shown states that if one draws a 2.5cms vertical line from point where the IVC emerges from the abdomen, and then measures 2.5cms posteriorly, if the border of the LV is beyond that horizontal line then LVE is implied
Ashley Davidoff MD
Ashley Davidoff MD
15416C02W lateral.thirds
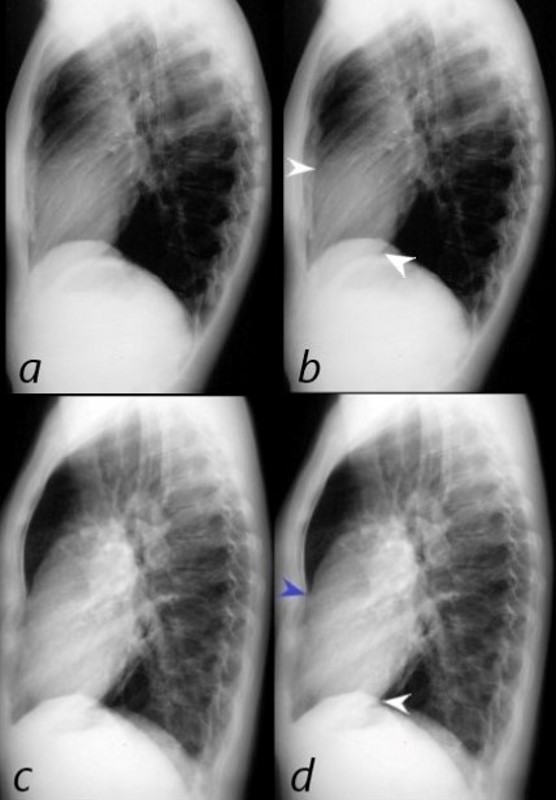
The normal lateral CXR (a,b), shows anterior and superior border of the heart (anterior white arrowhead) occupying 1/3 of the border between the sternomanubrial junction and the diaphragm.
The posterior and inferior white arrowhead shows the posterior border of the heart occupied by the RV taking up 1/3 of the distance of the diaphragm.
Images c and d represent left ventricular enlargement showing that the LV occupies about half the length of the diaphragm, (red arrowhead) while the retrosternal distance is unchanged and normal (white arrowhead).
Ashley Davidoff MD
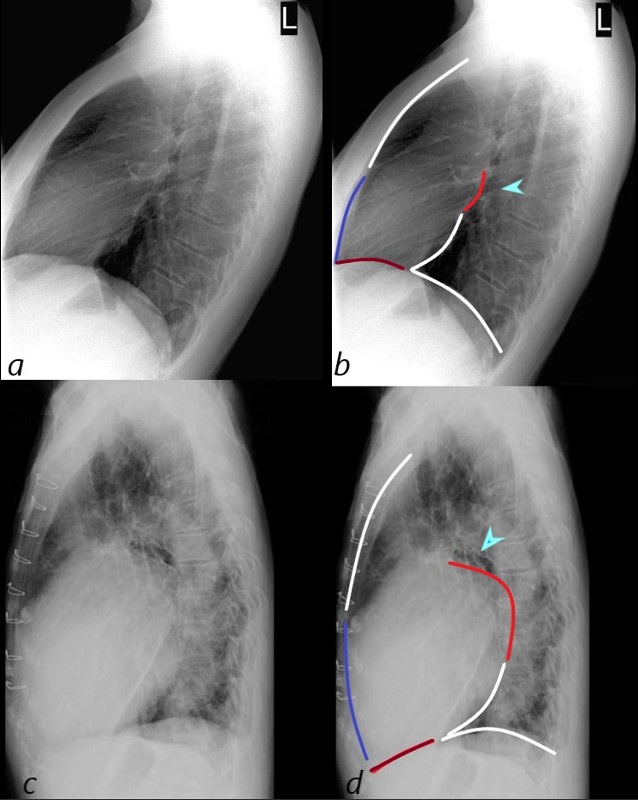
71 year old Asian female with rheumatic heart disease dominated by calcific mitral stenosis mild MR, moderate tricuspid regurgitation and secondary pulmonary hypertension.
The lateral examination (a, and b) show normal ratios of the length of the retrosternal air space, (upper anterior white line 2/3, and normal 1/3 length of the anterior RV border (blue line).
In images c and d the anterior overlay shows an increase in the ratio of the RV (navy blue-line to the upper 2/3 of the retrosternal space (white line) indicating RVE. Posteriorly, there is an increase ratio of the distance between the upper left atrial length (red – of posterior border of the left atrium (LA) and the lower border of the LV (white line) indicating LAE. In addition the straight left main bronchus (b – teal arrow) is shifted upward and is almost horizontal indicating LAE. Inferiorly the ratio of the length of the LV (maroon line is normal when compared to the rest of the diaphragm (white) indicating no evidence of LVE
Ashley Davidoff MD
Other Examples

87 year old male with findings consistent with mitral stenosis , characterised by calcified mitral valve, enlarged left atrium, normal sized left ventricle,with enlarged right atrium, right ventricle and main pulmonary artery.
Pure mitral stenosis is most commonly caused by rheumatic heart disease
Ashley Davidoff MD

87 year old male with findings consistent with mitral stenosis , characterised by calcified mitral valve, enlarged left atrium, normal sized left ventricle,with enlarged right atrium, right ventricle and main pulmonary artery.
Pure mitral stenosis is most commonly caused by rheumatic heart disease
Ashley Davidoff MD
27-year-old female presents with dyspnea and a past history of SLE, Raynaud’s disease, and Lupus nephritis.
Chest X-ray shows cardiomegaly with right ventricular configuration on the PA and an enlarged main and probably left pulmonary and an enlarged descending RPA. The lateral confirms the enlarged RV and raises the possibility of LV enlargement.

SLE and PULMONARY HYPERTENSION without ILD

CARDIOMEGALY WITH RVE
Ashley Davidoff MDThe CT scan confirms an enlarged MPA, RPA, RA and RV, and shows calcification on the posterior leaflet of the mitral valve consistent with Libman Sacks vegetation. There is mild ground glass opacity at the lung bases but no sign of ILD.
A current non contrast abdominal CT shows a pericardial effusion and normal sized kidneys

Ashley Davidoff MD

Ashley Davidoff MD

Ashley Davidoff MD