
Copyright 2020
Size is one of the most important descriptors of the heart. It is a measurable entity, and determining whether the heart is normal or abnormal can be verified against a normal standard. Size and weight of many organs differ between the sexes and among age groups, and it is no different for the heart. Measurements may be linear, portray a volume, mass, rate or frequency. Size may be reflected as a ratio, such the size of the left atrium and the base of the aorta that should have close to a 1:1 ratio.
The analogy of the heart being fist sized is helpful conceptually, but has limited use in the clinical realm. The evaluation of the size of the heart in clinical medicine is of the utmost importance. Although the global size of the heart is important, the size of the individual chambers is even more so, and in fact essential.
| Structure | dimension | CT MRI | Echo |
| Left Atrium | diameter | 4cms | 4cms |
| LA volume | <40ccs | ||
| LV diameter | end diastole | <5cms | <5cms |
| end systole | <4cms | <4cms | |
| LV wall thickness | end diastole | <12mm | <12mms |
| end systole | <16-18mm | ||
| LV mass not indexed | mass | <200 gms | <200gms |
| LV mass not indexed | mass | <100gms | <100gms |
| RV diameter | diameter | <4cms | |
| RV wall thickness | diameter | 5mm | |
| Right Atrium | diameter | <5cms | <5cms |
| IVC | diameter | <2cms | <2cms |
| SVC | diameter | <2cms | <2cms |
| Azygous vein | diameter | <7mms | |
| Aortic annulus | diameter | <2.5cms | |
| Sinuses of Valsalva | diameter | <4cms | |
| Sino-tubular junction | diameter | <3cms | |
| Ascending aorta | diameter | <3.5cms | |
| PA | diameter | <3.0cms | |
| Branch PA | diameter | <2.0cms |
Size of the heart is one of the key determinants in the diagnosis of heart disease. Each of the chambers is so unique that separate criteria have been developed for each of the chambers. Linear measurements are still the standard for most evaluations.
Anatomical Evaluation
The post mortem evaluation of the heart historically has been the manner in which the measurements of the heart evolved, but cannot be accurately transposed to the living and beating heart, that is filled with blood and interstitial fluid.
The adult heart measures about 12 cm in length by 8 to 9 cm in width at the broadest part, by approximately 6 cm in thickness. Translated into inches, it would approximate 4.5 by 3.5 by 2.5. The weight of the heart varies from 280 to 340 grams in the adult male and from 230 to 280 grams in the adult female. Thus for the adult male it is just over half a pound and for the adult female it is about half a pound.
At post mortem LV thickness of the adult heart ranges from about 8mms to 1.3cms and is usually less than 1.5cms. The RV wall thickness ranges from 4mm-8mms., being thinnest on its free wall.
The volumes of the left ventricle have been well studied. The left ventricular end diastolic volume ranges from 55ccs to 190ccs, and end systolic volume from about 15ccs to 70ccs with a stroke volume of 35-130ccs, and ejection fraction ranging from 55% to 75%. For males the volumes are slightly higher and for females slightly lower.
The heart increases in weight and size as human’s age. At birth, the heart appears large in proportion to the diameter of the chest cavity. Between puberty and 25 years of age the heart attains its adult shape and weight. The size of the heart is governed by its overall mass, which reflects ventricular thickness, as well as the volume of the cavities.
The Normal Left Ventricle |
|
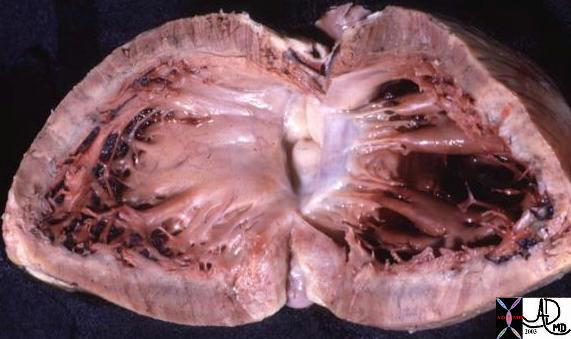
This anatomic specimen shows the LV with septal side to the left and free wall side to the right. Note the relatively smooth walled septal surface and the papillary muscle apparatus attached to the free wall side. The thickness of the anterior, lateral, and posterior wall is equal and symmetrical, and although the thickness of the septum is not visible in this view, its thickness approximates the thickness of the other walls. The left ventricular wall thickness is normal and was less than 15mms. Courtesy Ashley Davidoff MD 01817 |
LV Systole and Diastole Mild LVH
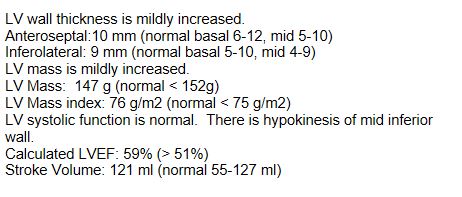
The Normal LV in diastole should be less than 12mm and in systole less than about 18mm. In this case the septum appears slighter thick (15.7mm) but the free wall is 8mm
Note the Mitral Valve is open
Ashley Davidoff MD TheCommonVein.net wall-thickness-001b
The Normal LV in diastole should be less than 12mm and in systole less than about 18mm.
Note the Mitral Valve is open
Ashley Davidoff MD TheCommonVein.net wall-thickness-001
Thickening in Systole
The LV in systole shows concentric thickening and this case demonstrates LVH Septum measures 25mm and the free wall measures 14.5 mm
Note the mitral valve is closed
Ashley Davidoff MD TheCommonVein.net wall-thickness-002b
The Normal LV in systole shows thickening
Note the mitral valve is closed
Ashley Davidoff MD TheCommonVein.net wall-thickness-002

The Normal Right Ventricle at Post Mortem |
|
The free wall in this normal post mortem specimen has been opened exposing the septum to the right of the image, the tricuspid valve to the left, the RVOT and pulmonary valve superiorly and the moderator band inferiorly. The right ventricular free wall is relatively thin and the normal range of thickness is between 4-8mm. In this instance the thickness of the free wall next to the ruler was not more than 5mms. Davidoff MD 06409b01 copyright 2009 |
Principles in Disease
Tubular structures remain normal in size if the pressure, volume, flow, and integrity of the walls is maintained. The heart is in effect a tube with modifications and therefore will follow the principles that govern tubular function.
In general tubular structures enlarge as a result of
increased pressure
increased volume
turbulent flow
loss of wall integrity.
Enlargement of the heart may result from hypertrophy or dilatation. Hypertrophy is caused by increased pressure and is usually results from stenotic valves, or increased afterload as a result of hypertension.
|
Left Ventricular Hypertrophy Normal Right Ventricle |
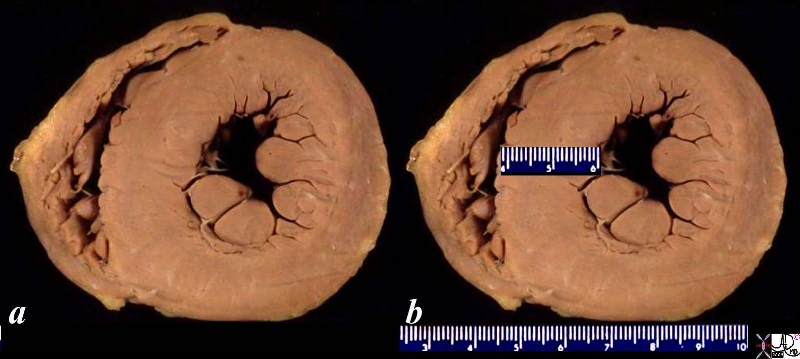
| The post mortem specimen shows a short axis transverse view through the right and left ventricle showing hypertrophy of the left ventricle. The ventricular septum measures about 2cms and should normally be less than 15mm. The right ventricle in this view is crescentic in shape with a wall that is normal in thickness.
Courtesy Ashley Davidoff copyright 2009 all rights reserved |
Increased volume is caused by an increased preload. An incompetent aortic valve, left to right shunt or a failing heart that cannot pump out what it receives will result in an increased preload. Loss of structural integrity, caused by a myocardial infarct for example will cause a dilated heart for multiple reasons. The weakened tissue will bulge, and the accumulation of blood in the chambers as a result of a failing pump may both contribute to the enlargement.
|
Dilated Left and Right Ventricle Complex Size Changes with Disease Atrophy Caused by Old Infarction, Swelling with New Infarction, Compensatory Hypertrophy and Normal
|
|
This pathological specimen shows a short axis through the heart with the left ventricle (right of image) and the right ventricle ( left of the image). The free wall of the left ventricle contains the papillary muscles and is slightly thickened either as compensation to the remaining diseased myocardium or due to other comorbid diseases such as the hypertension or aortic stenosis. There is a fresh infarction (black) posteriorly in the left ventricle extending to the posterior wall of the RV as well. The septum is thinned and fibrotic from an old infarction. The anterior wall of the right ventricle is hypertrophied. Courtesy Ashley Davidoff Md copyrighht 2009 all right reserved 15365b01b |

Causes of a small heart are much less common, though smallness of individual structures such as stenotic valves, hypoplasia, aplasia, and dysplasia commonly occur in the congenital disorders of the heart. There are usually compensatory mechanisms in the heart that will attempt to overcome the deficiencis so that the overall size of the heart increases. For example in tricuspid hyploplasia or atresia, the right atrium will enlarge as it attempts to push blood through the narrowed tricuspid valve, so that the overall size of the heart may increase to the extent that the child presents with a gigantic heart caused by a very dilated right atrium.
When the heart enlarges in disease, the cause of the enlargement can be approached in many ways. An anatomical differential diagnosis is one place to start. First, the parts of the structure being analyzed must be identified. Next, the enlargement should be localized to one or more of the components of the heart. If a heart is enlarged on a chest X-ray an important branch point depends on determining whether the left side is abnormally big, the right side or both. Left sided enlargement allows deduction that the left atrium and or left ventricle is enlarged. If it is finally established that the left ventricle is normal and the left atrium is enlarged, then stenosis of the mitral valve becomes the most likely candidate for the cause of the disease. Since mitral stenosis in an adult is almost always caused by rheumatic fever, one can further deduce that the cause of mitral stenosis was a pediatric infection with Lancefield type A beta hemolytic streptococcus bacteria. The patient probably acquired cardiac involvement from streptococcus pharyngitis when he or she was between 5-15 years. The polymers in the wall of the organism, called M proteins, are highly antigenic and at the time forced the patient’s defense mechanism to create antibodies. While responding to the foreign organism, these antibodies also inadvertently reacted to the patients own tissues, including the myocardium, and or mitral valve, and possibly the pericardium, brain and even joints. The depth of the detail in the diagnosis depends on the physicians knowledge, but the story would not have been a story, and the diagnosis would not have been made, and treatment would not have been instituted, had a diagnostic finding not been identified – in this case the change in size of the heart. The beginning of diagnosis, even if it involves complex disease, starts with simple observations of aberrant structure or function. In this case it started with the simple observation of a change in size in the heart.
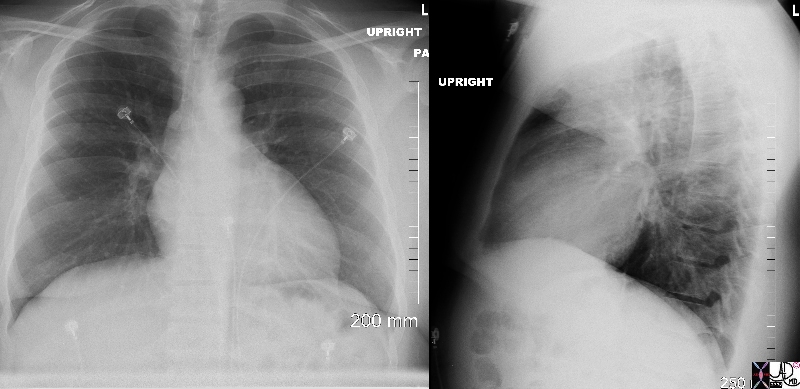
Normal and Enlarged Heart |
|
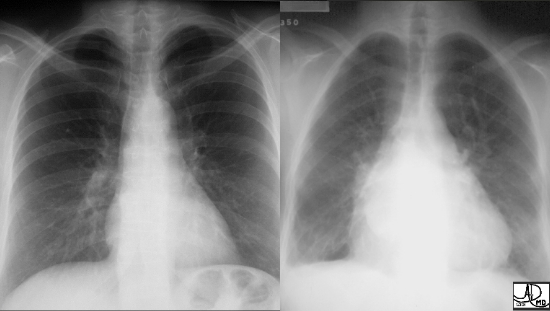
Two different patients showing the normal patient on the left and the CXR of a patient with an enlarged triangular shaped heart on the right. The triangular heart with upturned apex is characteristic of right ventricular enlargement, and the elevation of the carina and a double density seen on the right side of the heart suggests left atrial enlargement. These findings are consistent with rheumatic mitral stenosis. Courtesy of Ashley Davidoff M.D. 32113 copyright 2009 |
Clinical Medicine
In clinical medicine palpation of the heart is the most valuable tool to assess heart size. Most of the right ventricle is positioned anteriorly while only a small portion of the left ventricle, dominantly the apex, is anterior. The position of the apex enables the assessment of left ventricular size. It is normally palpated with the tips of index and middle fingers in the midclavicular line in the 5th intercostal space. In left ventricular enlargement the apex is projected down and out (laterally). The right ventricle lies anteriorly and is not usually felt but when enlarged a prominent parasternal heave is felt with the palm of the hand.
EKG
EKG is better able to evaluate individual chamber enlargement with atrial evaluation identified in the p wave and ventricular enlargement evaluated in the QRS complex. Right sided structures are evaluated in the leads overlying the right side of the heart, and left sided enlargement similarly on the leads on the left side of the heart. When the right atrium is enlarged the p wave becomes enlarged. The characteristic “p pulmonale” characterized by a high amplitude, (greater than 2.5mm) peaked, and narrowed p wave is present. When the left atrium enlarges the p wave, “p mitrale” results which is broader (>.11msecs) and notched so that the shape of the wave becomes shaped like an “M’ . Right ventricular hypertrophy is characterized by an R wave in leads V1 > 7mm, or if the R wave is larger than the T wave in V1. Right axis deviation is also a sign of right ventricular dominance.
Left ventricular hypertrophy has a number of criteria
QRS height
R in lead I plus S in lead III greater than 25 mm.
Increased precordial QRS voltage: S in lead V1 plus R in either V5 or V6 greater than 35 mm.
Large leftward voltage: R wave in lead L greater than 11 mm.
Typical ST and T abnormalities:
ST depression or T wave inversion (or both) in the “lateral” leads (I, L, V4-V6)
Imaging
There are a wide range of technologies that are able to measure cardiac size with variable accuracy. The CXR was the first imaging technique to evaluate heart size and was the only imaging technique for about 70 years until modern technology evolved. It is still commonly used but is not as accurate as echo CT or MRI.
CXR
The cardiothoracic ratio is the ratio between the transverse diameter of the heart and the widest diameter of the chest. The normal cardiothoracic ratio is less than 50%.

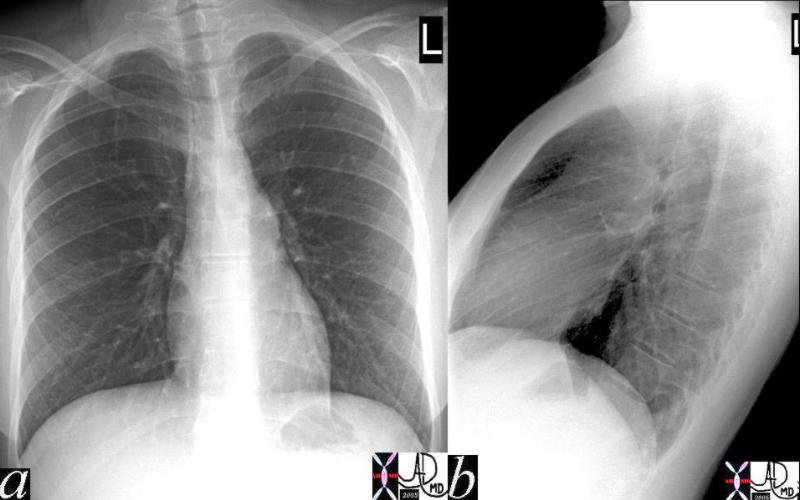
Historical Image The Cardiothoracic Ratio How to Measure |
| This CXR is of historical interest showing the manner in which cardiomegaly was assessed using the cardiothoracic ratio before the era of echocardiography and advanced imaging. The transverse dimension of the heart was measured to the the left and right of midline using the maximum diameter. In this instance the dimension to the right of midline was 3cms and to the left it was 10.2 cms giving a total of 13.2cms. The maximum dimension of the chest from inner ribs to inner ribs was 28.2 cms. The cardiothoracic ratio was therefore less than 50% (13.2/28.2)and thus considered normal.
Courtesy Ashley Davidoff MD copyright 2009 all rights reserved 36642b.8s |
The actual measurement of the cardiothoracic ratio is not used in clinical practice, but a geshtalt of the approximate cardiothoracic ratio is commonly used. The distinction between lung disease and heart disease for example in a patient with shortness of breath may rest in identifying cardiomegaly. The A-P examination magnifies the heart so evaluation of cardiomegaly with this projection should be used with caution.
|
Heart Size on the CXR and the Rules of Thirds |
| In the P-A projection the normal heart takes up about 30% of the diaphragmatic surface. Similarly in the lateral projection the heart takes up a third of the diaphragmatic surface. In addition the heart takes up the bottom 1/3 of the retrosternal air space.
41819c Courtesy Ashley Davidoff MD Copyright 2009 |
Applied Anatomy
In order to fully evaluate heart size on the chest X-ray (and any other imaging technology for that matter) knowledge of the relative position of the structures is important. A useful overlay is shown below.
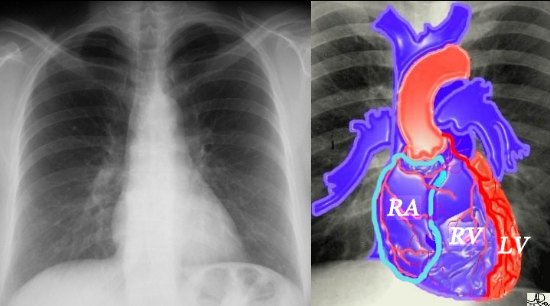
The Chambers of the Frontal Examination |
|
If we were to “crack open” the chest of the chest X-ray, the structures that would dominate this bloody, black and white scene, would be the right sided chambers. The right ventricle (RV) would be the dominant anterior chamber, and would form the dominant interface with the diaphragm. The right atrium (RA) would form the border with the right lung, and the RV . The RA would of course be slightly posterior to the RV. The left border would be formed by the left ventricle. Most the left ventricle is hidden posteriorly in this view. The left anterior descending artery would be visible from this anterior viewas well marking the position of the interventricular septum. Courtesy Ashley Davidoff M.D. 32064 copyright 2009 |

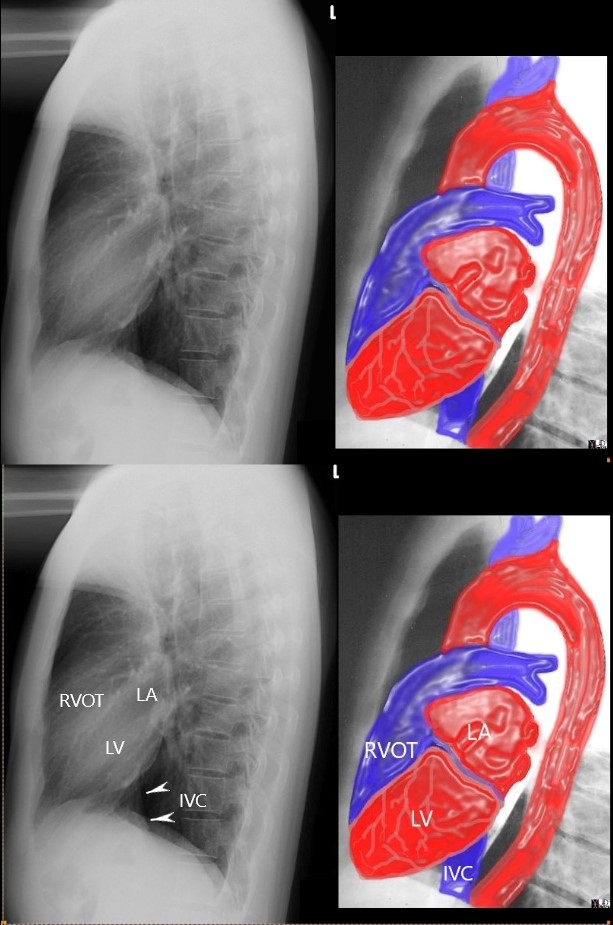
The lateral chest examination reveals an overlay of the structures that are visible, with the right ventricle (triangular blue structure) being anterior giving rise to the pulmonary outflow tract. The heart occupies 1/3 of the length of the sternum, with the upper 2/3 being occupied by lung (black tissue) The left ventricle is posterior and inferior most (2/3) of the posterior border of the heart and occupying the most inferior portion. The left atrium forms the upper 1/3 of the posterior border.
Ashley Davidoff MD
aka 15416C02W.8s
aka heart anatomy P 068
Ashley Davidoff MD
The echocardiogram provides a real time, safe, accurate, and relatively inexpensive method of evaluating the structures of the heart at any phase of the cycle. Measurements of size including volume, ejection fraction, wall thickness, valve areas, velocity and direction of flow are relatively easy to measure. This technique is the bread and butter of structural cardiac evaluation.
Courtesy Philips Medical Systems 33186
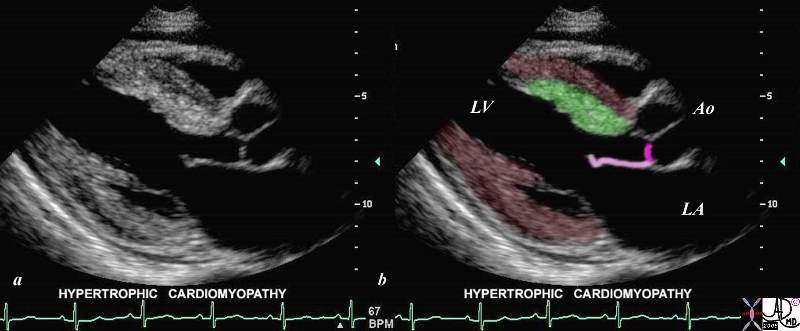
This gray scale echo of the heart shows the left ventricle, anterior (light pink) and posterior leaflets of the mitral valve, the aortic valve (dark pink), and the base of the aorta. There is a focal thickening of the ventricular septum (green) in the left ventricular outflow tract just proximal to the aortic valve. The region is also slightly more echogenic than the remaining myocardium (maroon). This case demonstrates a case of asymmetric septal hypertrophy or muscular subaortic stenosis.
Courtesy Philips Medical Systems 33134 33134c04.8s
CT scan for the evaluation of size
CT scan is being utilised increasingly for the evaluation of the heart and coronary arteries. It is used routinely for examinations of the chest, and although this examination is not tailored for cardiac evaluation.
Volume measurements and wall thickness measurements requires a diastolic frame in order to standardize the measurement and also because there is thickening of the myocardium during systole as it shortens. This requires a gated study in order to determine the phase of the heart
However the size of the atria and to some extent the ventricles can be fairly accurately and subjectively assessed often by reviewing the shape of the chambers.
Courtesy of: Ashley Davidoff, MD
aka 37758b01c01.8s
aka heart anatomy P 040

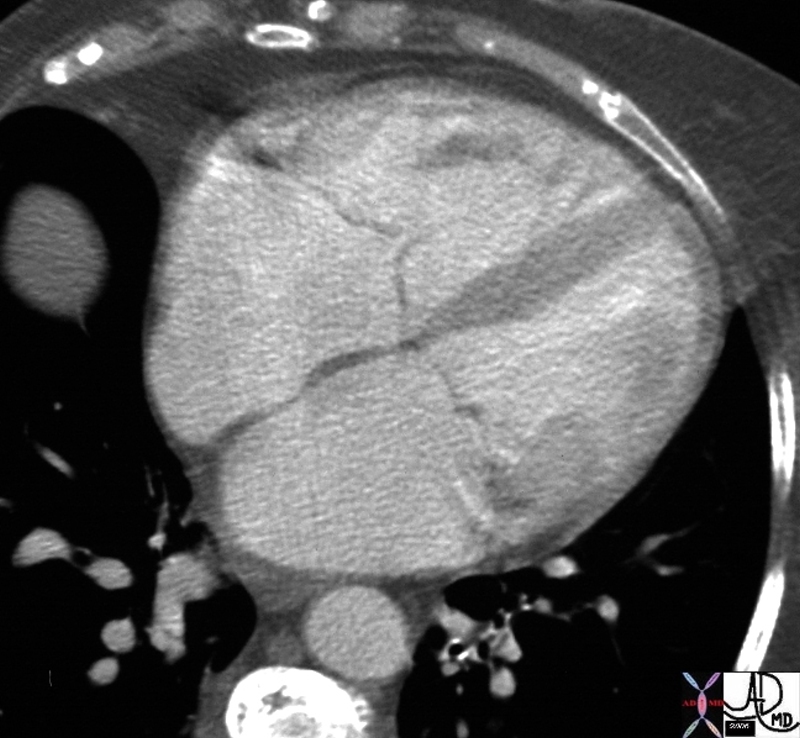
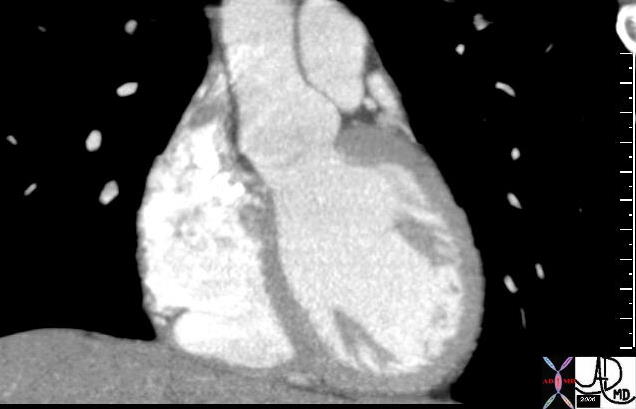
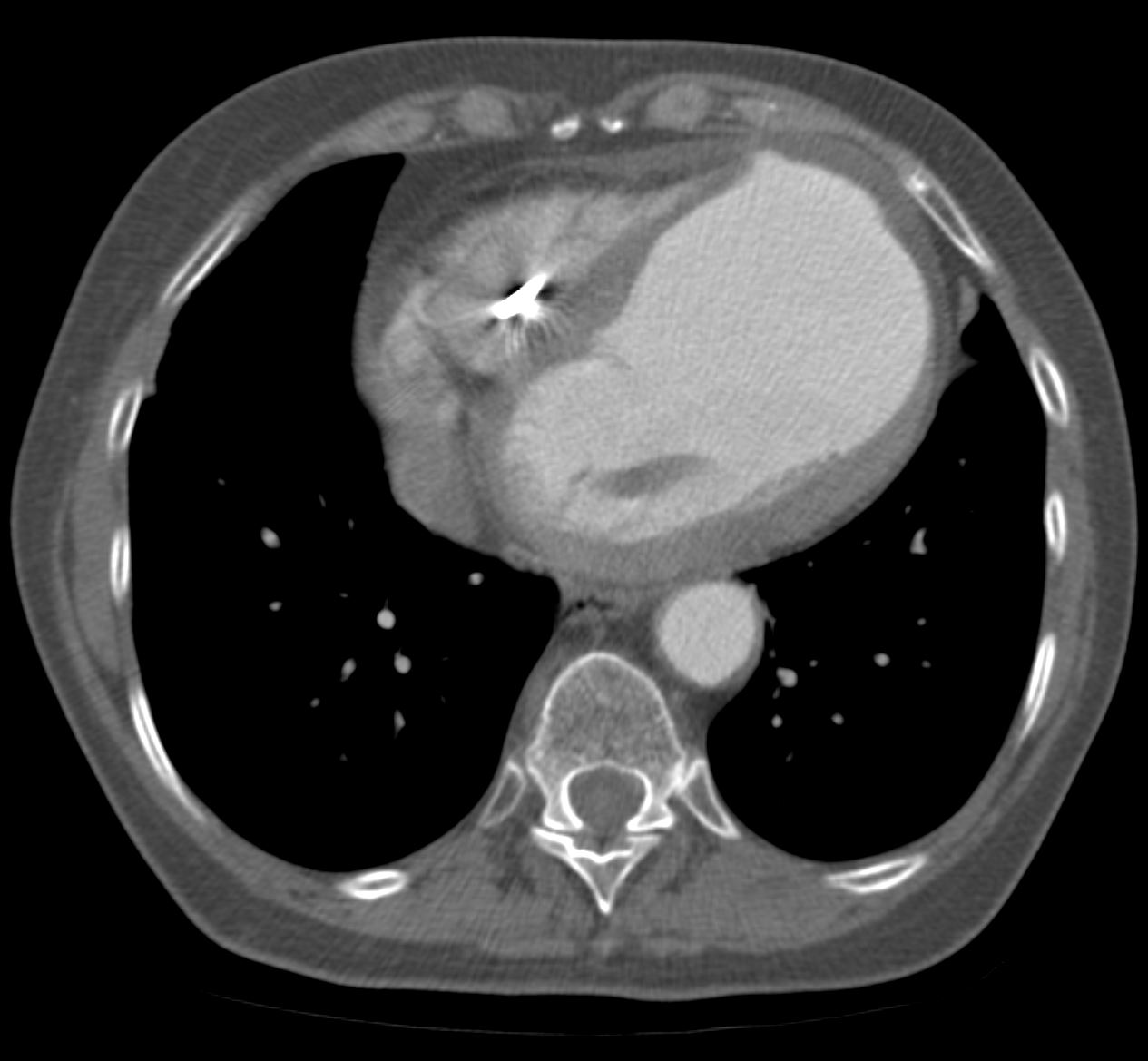
This elderly female recently sustained an acute MI complicated by cardiac arrest. Loss of myocardial mass and functional tissue has resulted in globular deformity of the heart as seen on this non gated CT through the chest. Note the malorientation of the posterior papillary muscle that prohibits normal function of the mitral valve and results in mitral regurgitation. A Small pericardial effusion is present.
Courtesy Ashley Davidoff MD TheCommonVein.net 75517
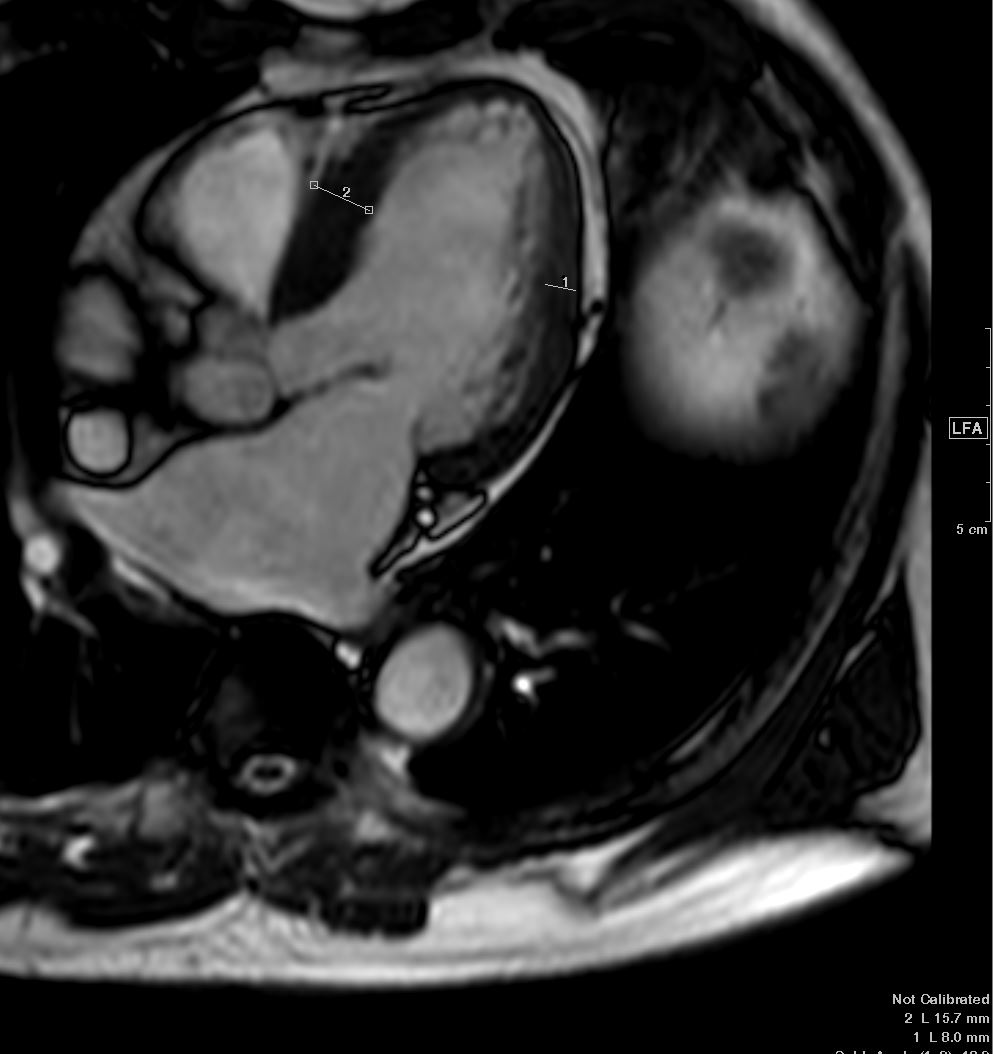
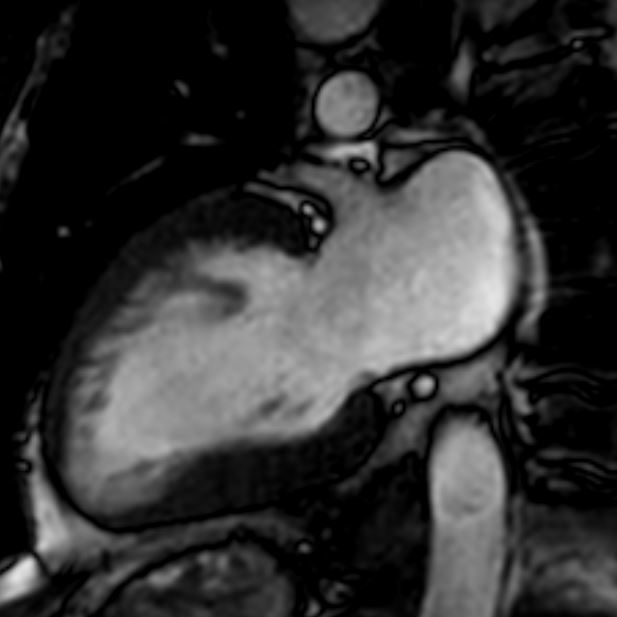
MRI is not a routine method for the evaluation of heart size due to the accurate capabilities of echocardiography which is safe, inexpensive and accurate. However there are many advantages that gated cardiac MRI offers in the evaluation of the heart.

In the gated MRI systole and diastole can be differentiated and so standard measurement to thickness, and volume can be applied for evaluation of size.
This MRI series demonstrates the heart in systole and diastole. Image 1 demonstrates ventricular systole. The atrial chambers are full, the A-V valves are closed and the ventricular chambers are contracted. Image 3 is a color overlay of the closed A-V valves of image 1. Image 2 demonstrates ventricular diastole. The atrial chambers are emptying, the A-V valves are open and the ventricular chambers are full. Image 4 is a color overlay of the open A-V valves of image 2.
Ashley Davidoff TheCommonVein.net
32073
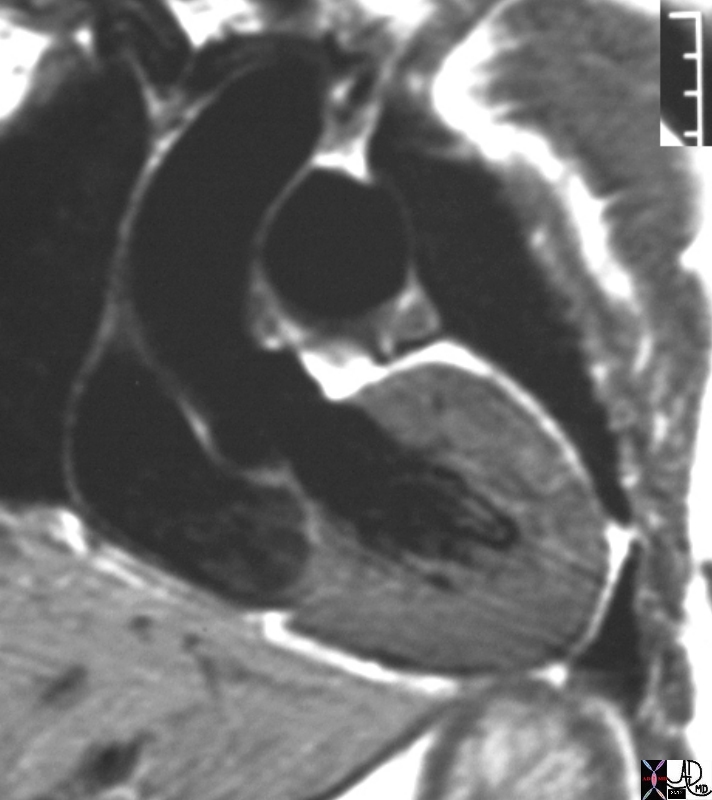
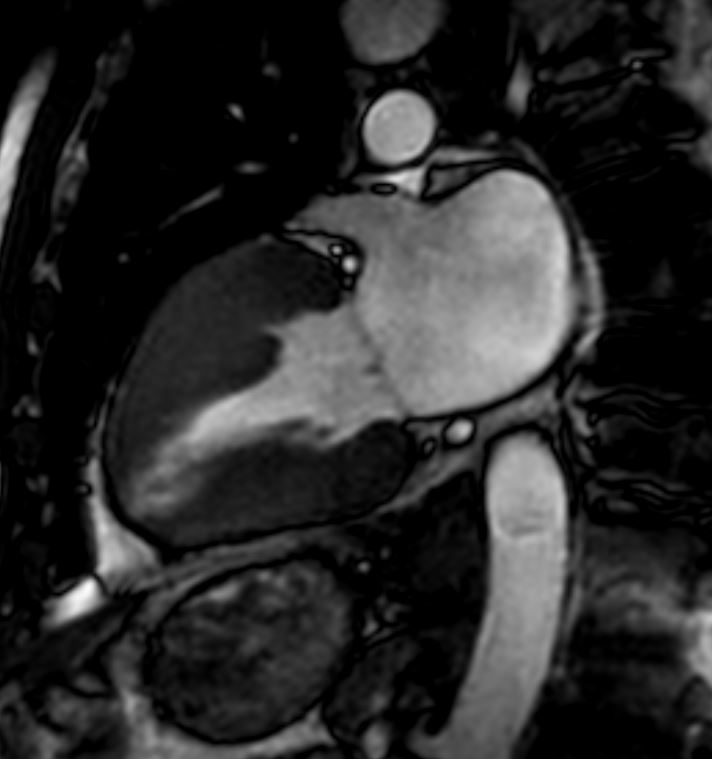
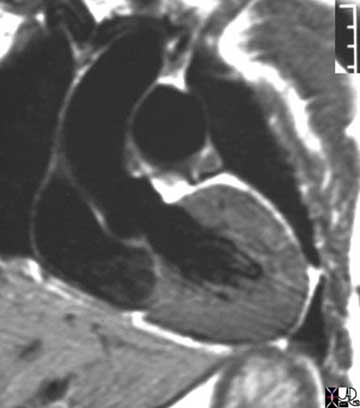
# heart LV left ventricle aorta coarctation left ventricular hypertrophy fx LVH concentric hypertrophy dx coarctation imaging radiology T1 weighted MRI Courtesy Ashley Davidoff MD TheCommonVein.net 16906.800
Angiography
Overall heart size is not easily evaluated by angiography since only the cavity is visible. However the hypercontractile ventricle is an indirect sign of ventricular hypertrophy.
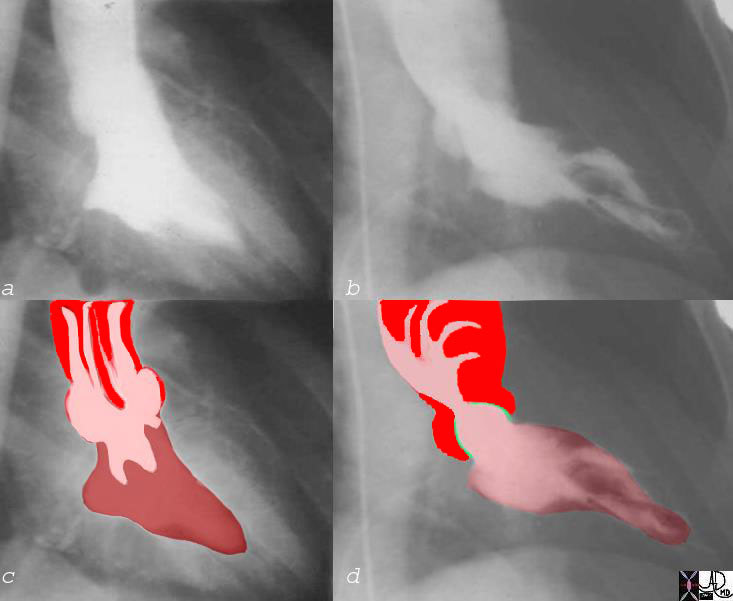
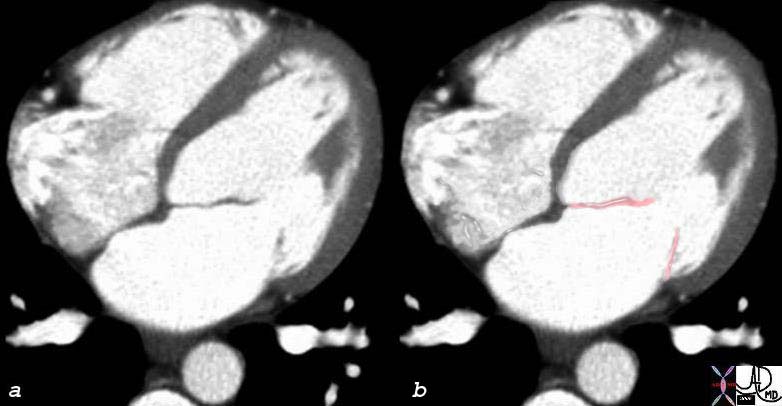
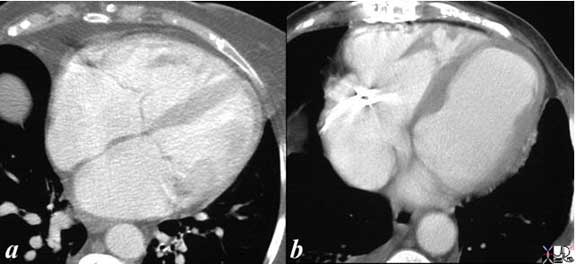
The normal ventriculogram in the RAO projection is demonstrated in image a and overlaid in c, while the hypercontractile LV caused by aortic stenosis manifests with a ballet slipper like appearance of the LV at end systole (image b and d). The ejection fraction of left ventricle in the patient with aortic stenosis was 80%. The aortic valve is mildly thickened and has minimal doming. (green overlay)
Courtesy Ashley Davidoff MD TheCommonVein.net 07969c06
Left Atrium
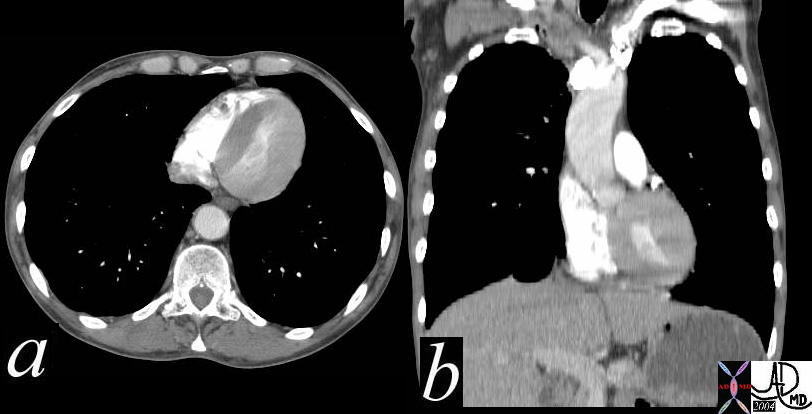
Cor Bovinum |
|
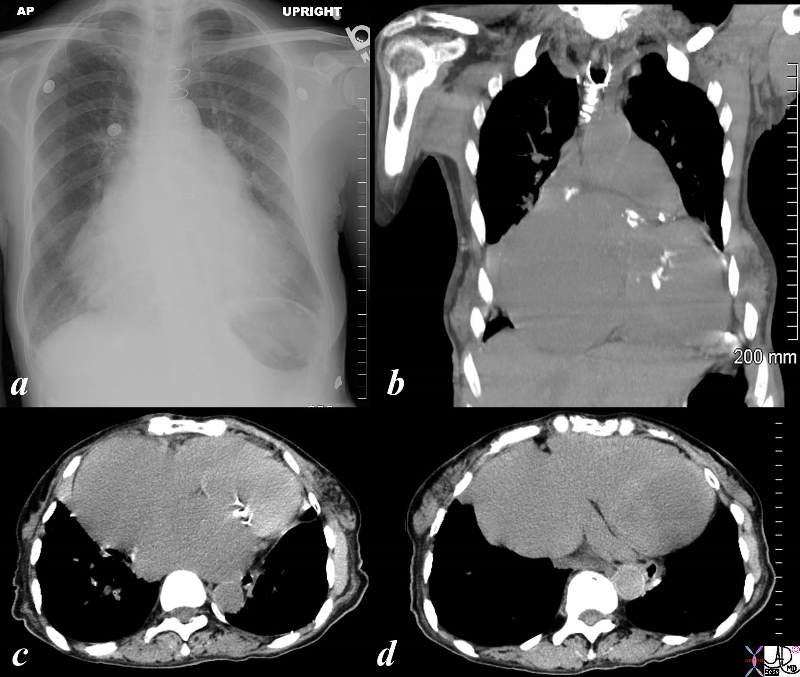
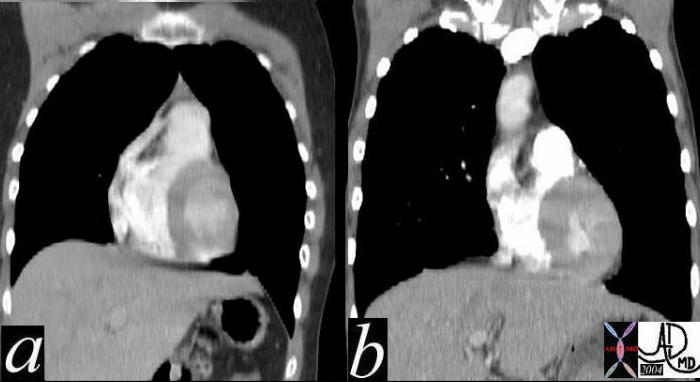
The series of a plain film of the chest (a), and coronal image of reconstructed CT (b), reveals an almost wall to wall heart called a cor bovinum – literally a bull’s heart – corresponding to its very large size. The axial images c, show calcified mitral valve consistent with mitral stenosis, secondary left atrial enlargement and pulmonary hypertension and extremely dilated right atrium seen in both image c, and d. Courtesy Ashley Davidoff copyright 2009 all rights reserved 86859c02.8s |
76287c02 |
| 76287c02 heart cardiac LV left ventricle MV mitral valve open diastole diastolic phase atrial septum normal anatomy CTscan Courtesy Ashley Davidoff MD |
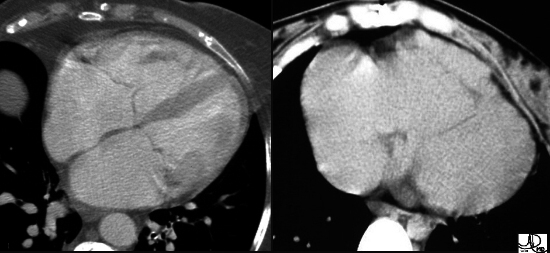
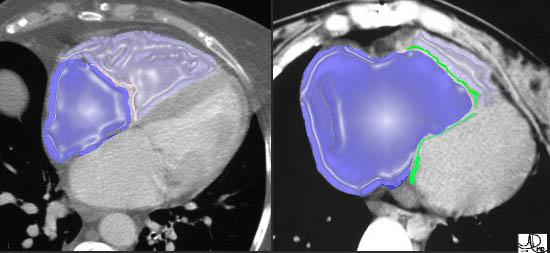
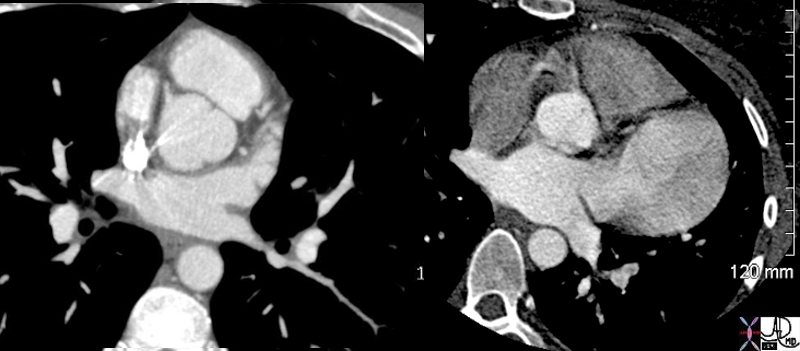
What is the Cause of the Cardiomegaly? |
|
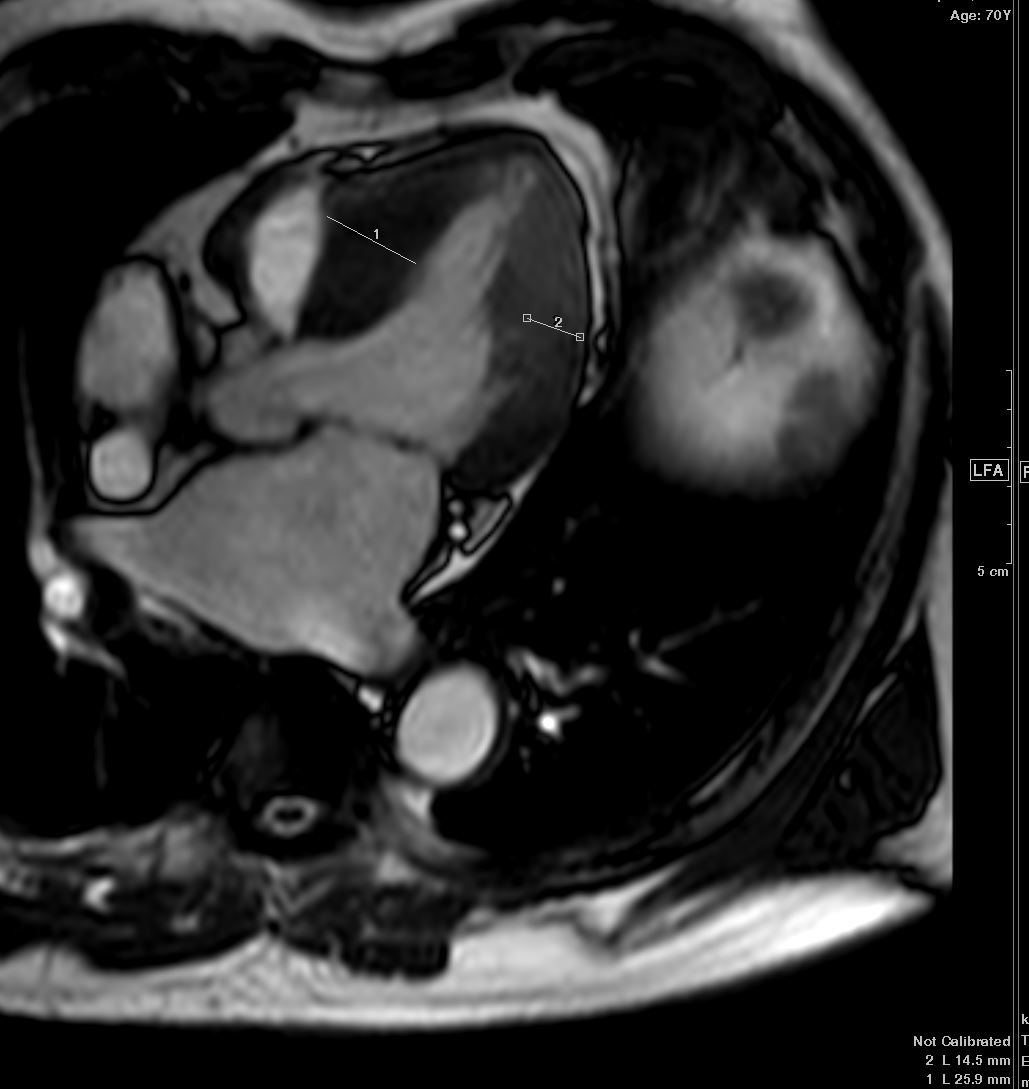
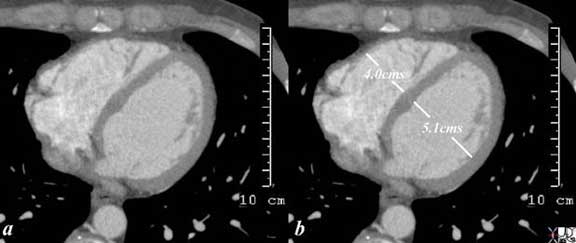
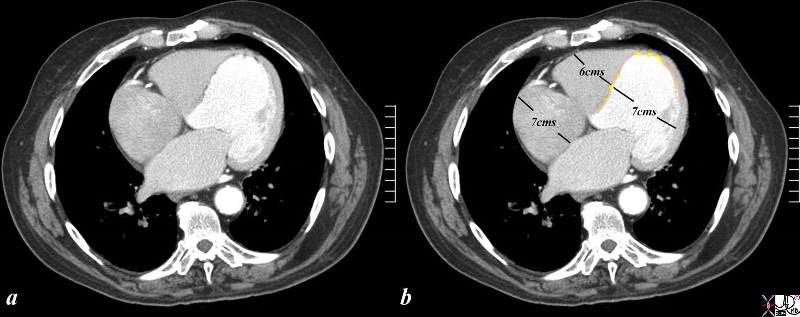
The CTscan is from a 76 year old man in whom the dominant finding is of left ventricular enlargement characterized by the rotund shape of the ventricle. The RA and RV are also enlarged based on this image, and LA was enlarged as well suggesting global cardiomegaly consistent with a cardiomyopathy. The clue to the cause of the enlargement is the segmental nature of the disease characterized by the asymmetry thickness when the free wall thickness is compared to that of the thinning of the septum. In addition the presence of fat (yellow overlay) in the thinned and probably scarred myocardium making ischemic cardiomyopathy the likely diagnosis. At the apex, there is there is a subtle calcification as well. Courtesy Ashley Davidoff Copyright 2009 All rights reserved 86984c05.8s01 |

The CT of this patient shows a severe pectus excavatum causing compression of the right atrium, left atrium and right ventricle. Note the right sided breast prosthesis. Pectus excavatum does not usually affect the function of the heart
Courtesy Ashley Davidoff TheCommonVein.net 25133b.8s
The Right Atrium
The linear measurements for the normal right atrium are a short axis of 3.5 cms and a long axis of 5.5cms. Since it has the same volume as the left atrium it should be about the same size but comparison is not that easy for a few reasons, including the different orientations of the chambers as well as the fact that they often lie in different planes making comparison at a single level difficult.. The long axis of the right atrium is mostly in an A-P direction,whereas the long axis of the left atrium is mostly in a transverse direction. They also lie only a slightly different axial plane so theat theright strium (like most right sided structures
Normally, right and left atria are the same size.
This axial image of the heart is through the mitral (right ) and tricuspid valve (left) right atrium and left atrium (right) which are normal and about the same size. The left ventricle with the papillary muscles and the right ventricle with its papillary muscle are well seen. Note the right sided structures tend to be anterior and left sided structures tend to be posterior. Note also that the right atrium and the left atrium are about the same size and shape in this view with flat walls.
Ashley Davidoff MD TheCommonVein.net 27531d01.8s
|
Right Atrium Normal and Enlarged |
| These two images are enhanced CT images through the tricuspid valve. The first image is normal, while the second image demonstrates a TV that lies too far forward and low associated with a huge RA and a diminutive RV. This appearance is classical of a congenital condition called Ebstein’s anomaly. In this disease, the posterior leaflet is stuck down to the posterior wall of the RV and the anterior leaflet is larger than normal often giving a flapping sound to the listening ear. The anterior leaflet behaves like a flapping sail in the wind of the blood flow.
In the overlays, the RA is in royal blue and the RV is in light purple overlay. The normal TV in the first image is in pink while the malformed valve in the second image is in green. Note how large the RA is and how small the RV is in Ebstein’s anomaly. Courtesy of Ashley Davidoff M.D. 32102 32101 copyright 2009 |
Right Ventricle
RV (major) 6.5 – 9.5cms RV (minor) 2.2 – 4.4cms
RV dilatation was identified in case RV end-diastolic diameter was greater than 46mm (inflow tract) or 24mm (outflow tract),
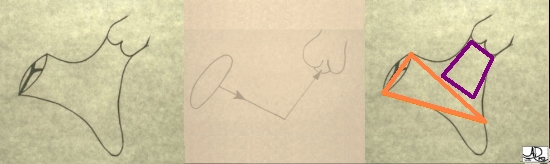
Inflow and Outflow Components of the Right Ventricle |
| The first diagram is a simple drawing of the right ventricle as seen in a frontal projection. The tricuspid valve is to the left and inferior and the pulmonary valve to the right and superior. The arrows of the second diagram show the inflow portion of the right ventricle and the outflow portion. The third and last diagram shows the two chambers that make up the right ventricle. The right ventricular inflow chamber also called the RV sinus is triangular and in orange while the outflow chamber is more tubular or cylindrical and has been called many names – but somehow it does not seem to care. Right ventricular outflow tract (RVOT), and infundibulum seem to be the most popular.
Courtesy of Ashley Davidoff M.D. 32087 copyright 2009 |
The RVOT is usually crescentic in shape, and usually has an A-P diameter of 2.2cms and a long axis of 4.4 cms. If the A-P diameter is greater than 2.5cms then enlargement is suspected. The right ventricle has an unusual shape, and assessing its volume has always been a challenge and has been difficult to represent mathematically, but three dimensional methods may enable adequate measurement.
It is also reasonable to divide the right ventricle into an inflow portion and an outflow portion and to consider them separately.
Change in shape to a more rounded configuration of the free wall, bulging of the septum toward the left ventricle
“The shape of the RV limits quantitation of its function and volume. The left ventricle (LV), by contrast, has an elliptical shape and is readily evaluated. The shape of the right ventricle has been described as a pyramid with a triangular base; however, this description fails to take into account its crescentic shape in cross section or its outflow tract. A “teapot” configuration has been proposed as a model that includes the outflow tract, but this is difficult to represent mathematically. The tomographic nature of echocardiography makes it impractical to image this irregularly shaped organ in a single, encompassing plane. A number of studies have attempted to measure the size or volume of the RV, but no method has gained wide acceptance. Three dimensional methods may, however, provide the flexibility required to adequately measure this structure.” (Maysky)
“A number of simple approaches for determining RV size have been used:
– Inspection of the RV and LV from the standard M-mode echocardiogram that was recorded from the precordial long axis view. Antero-posterior dimension in excess of 2,5 cm is suggestive of right ventricular dilation (fig. 7.2, B). However, there are problems inherent in this approach as the recording of the RV chamber is usually obtained from a narrower portion of the chamber.
– Measurement of the RV directly from the two dimensional image is a preferred technique
– Qualitative inspection of four views of the RV obtained from the two dimensional echocardiogram also serves as a safety valve to avoid overlooking enlargement
1). In the long and short axis precordial views, where the RV outflow tract is seen coursing over the LV outflow tract and aortic root, the RV appears to be crescent shaped and its size, if normal, is considerably less than that of the LV. When right ventricle is equal to or larger than the left ventricle in these views, it is unequivocally enlarged. (fig. 2.12)
2). The second view is the short axis through the LV minor axis. Right ventricular dilation can be strongly suspected if its size appears to be the same or larger than the LV.
3). When RV dilation is suspected, particular attention is paid to the apical four chamber view in which the LV forms the cardiac apex and the normal RV appears to be the smaller of the two chambers. If the RV forms or even shares the apex, RV dilation is suspected. In frank RV enlargement it appears to dominate, and in extreme cases, the LV appears slit-like by comparison (fig. 7.3).
4). If there is still uncertainty about RV size, attention should be directed to the subcostal view, which is less likely to produce a false positive impression of RV enlargement. Normally, the LV appears to extend further than the RV, which appears shorter and smaller in diameter. When the RV fails to appear truncated and equals or exceeds the LV in length and diameter, RV dilation is suspected.
Right Ventricular Dilatation and Hypertrophy
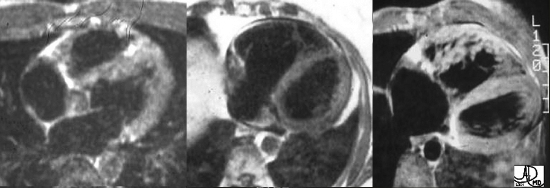
The Large Right Ventricle Dilatation and Hypertrophy |
|
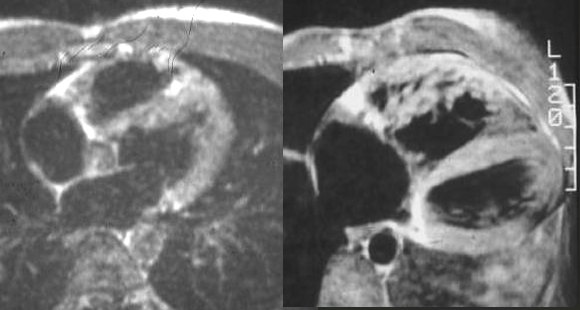
These three images represent T1 weighted images of the RV reflecting from left to right, normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV is the first image on the left with thin wall and triangular shape. The middle image is from a patient with an atrial septal defect (ASD) resulting in a volume overloaded – thin-walled, rounded, and dilated RV . The image on the right is from a patient with congenital heart disease with pressure overload of the right ventricle showing heavy trabeculations of the RV and thickened wall. Courtesy of Ashley Davidoff M.D. 32095 |
|
32095 |
| These three images represent T1 weighted images of the RV reflecting normal, dilated, and hypertrophied conditions. Normal thin-walled capacious RV (1) ASD (Atrial Septal Defect) with volume overloaded – thin-walled but dilated RV (2) Pressure overloaded , hypertrophied RV, with accentuated trabeculations (3) Courtesy of Ashley Davidoff M.D. 32095 |
Left Atrium
LA (major) 4.1 – 6.1cms LA (minor) 2.8 – 4.4cms
|
Normal left Atrium |
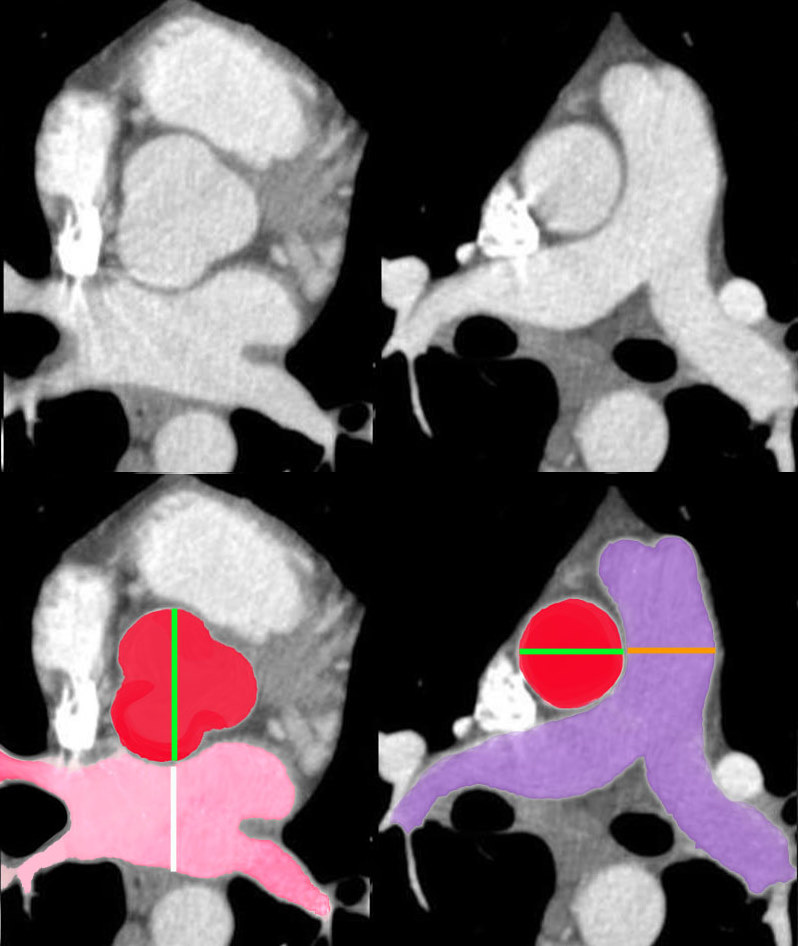
| The size of the left atrium (pink) is best assessed by comparing its A-P dimension with the dimension of the aortic root (red). It is usually just slightly larger than the root. The borders of the LA are usually flattened and the LA often has a rectangular appearance as seen in this image. The size of the PA is usually about the same size as the ascending aorta. this axila projection is therefore exteremely useful in assessing the size of the LA Pa and aorta.
34769c07b02 anatomy CTscan Davidoff MD |
Left Ventricle
Posterior LV thickness: 0.6-1.1 cm
Interventricular septum: 0.6-1.1 cm
Mass: 92± 16.0 gm/m2
End-Diastolic Volume: 70 ± 20.0 ml/m2
Stroke Volume: 45± 13.0 ml/m2
Ejection Fraction: 0.67 ± 0.08 .
LV (major) (ED) 6.9 – 10.3cms LV (minor) (ED) 3.7 – 5.7cms
LV (minor) (ES) LV %FS 27 – 50%
LVID (end diastole) 3.7 – 5.7cms LVID (end systole)
%Fractional shortening 25-53%
Interventricular septum (ED) .6 -1.4cms Interventricular septum (ES) .8 – 2.0cms
LVPW (ED) .5 – 1.3cms LVPW (ES) .9 – 2.1cms
Aorta (ED) 2.0 – 4.0cms (ref)
|
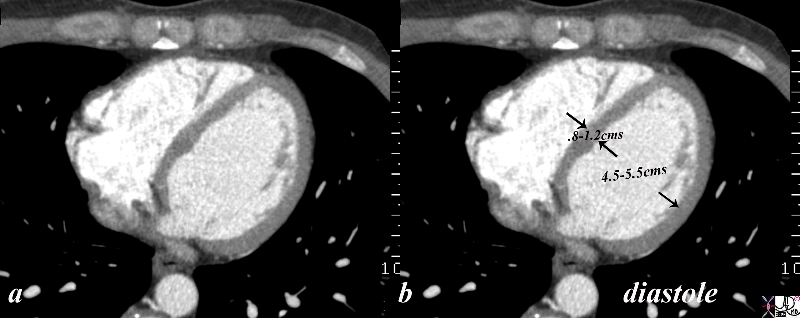
Normal Left ventricle Taken in Diastole |
| The gated CT scan was taken in diastole and shows the normal left ventricular dimensions which for the left ventricle wall is between .8cms and 1.2 cms, and for the cavity is 4.5-5.5cms. the measurement should be taken at the level of the papillary muscles which is in mid ventricular cavity.
Courtesy Ashley Davidoff copyright 2009 all rights reserved 34765c02.8s |
|
34780 |
| 34780 heart left ventricle LV mitral valve apparatus papillary muscles normal anatomy Davidoff MD |
|
39088c01 |
| Coronal reformats through the chests of two different patients. They are approximately at the same level of the RVOT. The left image (a) is normal, while image b shows concentric thickening of the LV. Courtesy Ashley Davidoff MD 39088c01 code cardiac heart normal LVH LV hypertrophy |
|
39088c |
| This axial and coronal reformatted CTscan of the left ventricle and the aorta show concentric hypertrophy of the LV and ectasia of the ascending aorta in this patient with severe systemic hypertension. Courtesy Ashley Davidoff MD. 39088c code CVS LV LVH AO ectasia hypertension |
|
Left ventricular Hypertrophy |
| The PA and lateral chest x-ray shows evidence of cardiomegaly with the left ventricle pointing down and out in the PA examination andtaking up more than a third of the diaphragmatic space on the lateral and bulging posteior to the IVC. These findings are characteristic of LVH – with ta change mostly in shape rather than an overt change in size.
Copyright 2009 Courtesy Ashley Davidoff MD 76788c.8s |
The Right Atrium
Range of Heart Rates per Minute and Average Heart Rate for Various Ages
| Age | Range | Average Rate
|
| 0-1 month | 100-180 | |
| 2-3 months | 110-180 | |
| 4-12 months | 80-180 | |
| 1-3 years | 80-160 | (130) |
| 4-5 years | 80-120 | (100) |
| 6-8 years | 70-115 | (100) |
| 9-11 years | 60-110 | (88) |
| 12-16 years | 60-110 | (80) |
| >16 years | 50-90 | (70) |
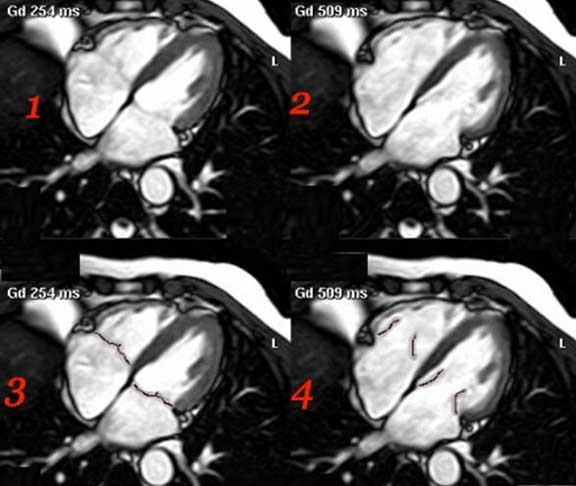
In the gated MRI, systole and diastole can be differentiated and so standard measurement to thickness and volume can be applied, for evaluation of size. This MRI series demonstrates the heart in systole and diastole. Image 1 demonstrates ventricular systole. The atrial chambers are full, the A-V valves (tricuspid valve and mitral valve) are closed and the ventricular chambers are contracted. Image 3 is a color overlay of the closed A-V valves of image 1. Image 2 demonstrates ventricular diastole. The atrial chambers are emptying, the A-V valves are open and the ventricular chambers are full. Image 4 is a color overlay of the open A-V valves of image 2. 32062
Normal Left Atrial Appendage and Aneurysm of LAA |
| 70025d01 heart cardiac left atrium LA left atrial appendage fx enlarged fx aneurysmal dx aneurysm of the left atrial appendage CTscan Davidoff MD |
Ashley Davidoff MD TheCommonVein.net LV aneurysm 005
Recent MI
This elderly female recently sustained an acute MI and the resulting functional myocardial loss has resulted in a globular deformity of the heart as seen on this non gated CT through the chest. Note the malorientation of the posterior papillary muscle that prohibits normal function of the mitral valve and results in mitral regurgitation. A Small pericardial effusion is present.
Courtesy Ashley Davidoff MD copyright TCV 2008 75517
The CT of this patient shows a severe pectus excavatum causing compression of the right atrium, left atrium and right ventricle. Note the right sided breast prosthesis. Pectus excavatum does not usually affect the function of the heart
Courtesy Ashley Davidoff TheCommonVein.net 25133b.8s
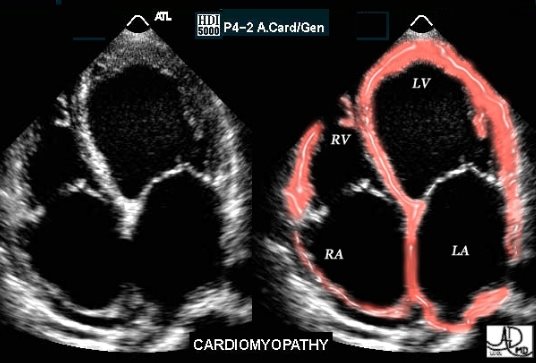
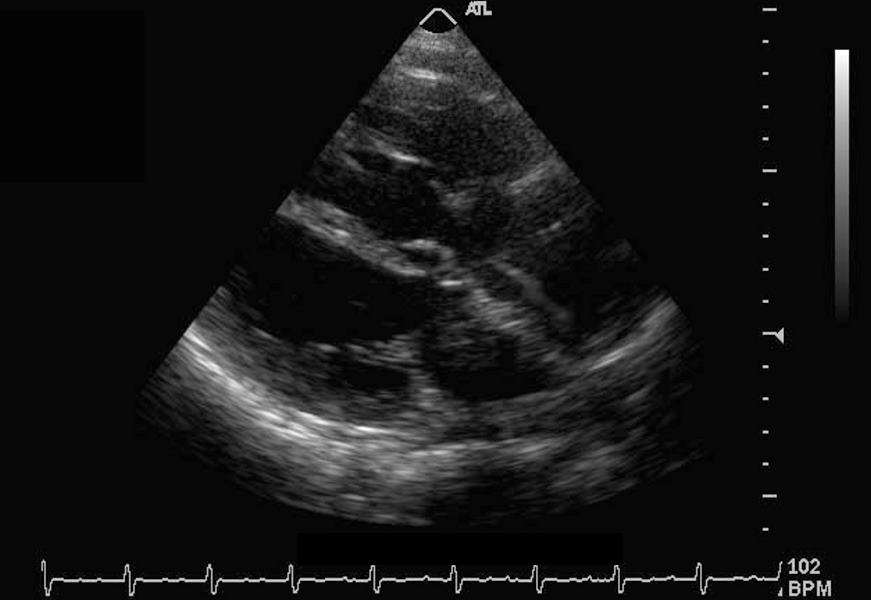
This image is a real time echocardiogram, projecting a 4 chamber view. The patient is suffering from cardiac failure as a result of cardiomyopathy. All four chambers are dilated in this instance. All the chambers appear to be full and distended. In previous studies we have noted that the functional phases of atria and ventricles are opposite so that at peak systole the atria in general are fullest whereas the ventricles are “empty”, with the opposite being true in peak diastole. In this image all 4 chambers appear to be full and distended so that they all appear to be in peak diastole. This is obviously abnormal.
(Images courtesy of Philips Medical Systems, Ultrasound, and modified by Ashley Davidoff M.D.)
| Structure | dimension | CT MRI | Echo |
| Left Atrium | diameter | 4cms | 4cms |
| LA volume | <40ccs | ||
| LV diameter | end diastole | <5cms | <5cms |
| end systole | <4cms | <4cms | |
| LV wall thickness | end diastole | <12mm | <12mms |
| end systole | <16-18mm | ||
| LV mass not indexed | mass | <200 gms | <200gms |
| LV mass not indexed | mass | <100gms | <100gms |
| Right Atrium | diameter | <5cms | <5cms |
| IVC | diameter | <2cms | <2cms |
| SVC | diameter | <2cms | <2cms |
| Azygous vein | diameter | <7mms | |
| Aortic annulus | diameter | 2.5cms | |
| Sinuses of Valsalva | diameter | 4cms | |
| Sino-tubular junction | diameter | 3cms | |
| Ascending aorta | diameter | 3.5cms | |
| PA | diameter | 3.0cms | |
| Branch PA | diameter | 2.0cms |
Applied biology
references